3451
Procedure for Normalization of Cerebrovascular Reactivity in Bilateral and Indeterminate Patterns of Hypoperfusion using Dynamic BOLD-CVR1Bernard and Irene Schwartz Center for Biomedical Imaging, Department of Radiology, New York University Grossman School of Medicine, New York, New York, USA., New York, NY, United States, 2Center for Advanced Imaging Innovation and Research (CAI2R), Department of Radiology, New York University Grossman School of Medicine, New York, New York, USA., New York, NY, United States, 3Department of Radiology, Weill Cornell Medical College. New York, New York, USA., New York, NY, United States, 4Department of Neurology, New York University Grossman School of Medicine, New York, New York, USA, New York, NY, United States
Synopsis
Keywords: fMRI Analysis, fMRI
Motivation: The BOLD response to acetazolamide offers robust estimation of cerebrovascular reactivity (CVR) with dynamic interrogation for maximal (CVRmax) augmentation. The lack of physiologic units limits use to relative CVR reductions versus normal hemispheres, confounding use for bilateral steno-occlusive disease (SOD).
Goal(s): Develop normal voxel search procedure for BOLD-CVR informed by DSC perfusion in SOD.
Approach: DSC in unilateral SOD patients undergoing BOLD-CVR were used to train random forest classifiers and identify voxels with CVRmax within 10% of ground-truth normal hemispheric CVRmax.
Results: Median percent-differences <8% from ground-truth were achieved, indicating robust performance for extension of BOLD-CVR to bilateral SOD.
Impact: We demonstrate the feasibility of a random forest classifier as a normal voxel search algorithm, in order to identify candidate voxels serving as an auto-normalization for CVR studies in settings of bilateral or indeterminate patters of steno-occlusive disease.
Introduction
Cerebrovascular reactivity (CVR) reflects the capacity for cerebral resistance vessel dilatation in response to hemodynamic stimuli.1 Decreased CVR is associated with increased stroke risk in chronic steno-occlusive disease (SOD).Blood-oxygen-level-dependent (BOLD) MRI following acetazolamide (ACZ) infusion has emerged as an approach to study CVR, with unique attributes including remarkable dynamic capabilities.1, 2 Recently, we introduced a flexible computational pipeline permitting extraction of full CVR dynamics, including isolation of transient and unsustained maxima (CVRmax) in the ACZ response.3, 4
As with most approaches to assessing hemodynamic failure, including implementations of gold-standard 15O PET, the absence of true physical units for parameters of interest limits their use as relative estimates of diseased tissues versus contralateral normal tissues.5 Constraints to pragmatic use of such techniques in patients with bilateral or indeterminate distributions of SOD thus severely limits their utility in clinical practice and undermines clinical trial design, due to the frequency with which bilateral or multi-territory cerebrovascular disease may be encountered in high-risk patients. Extension of these techniques to bilateral disease subjects would greatly enhance the contribution of CVR and related measurements for clinical and scientific use.
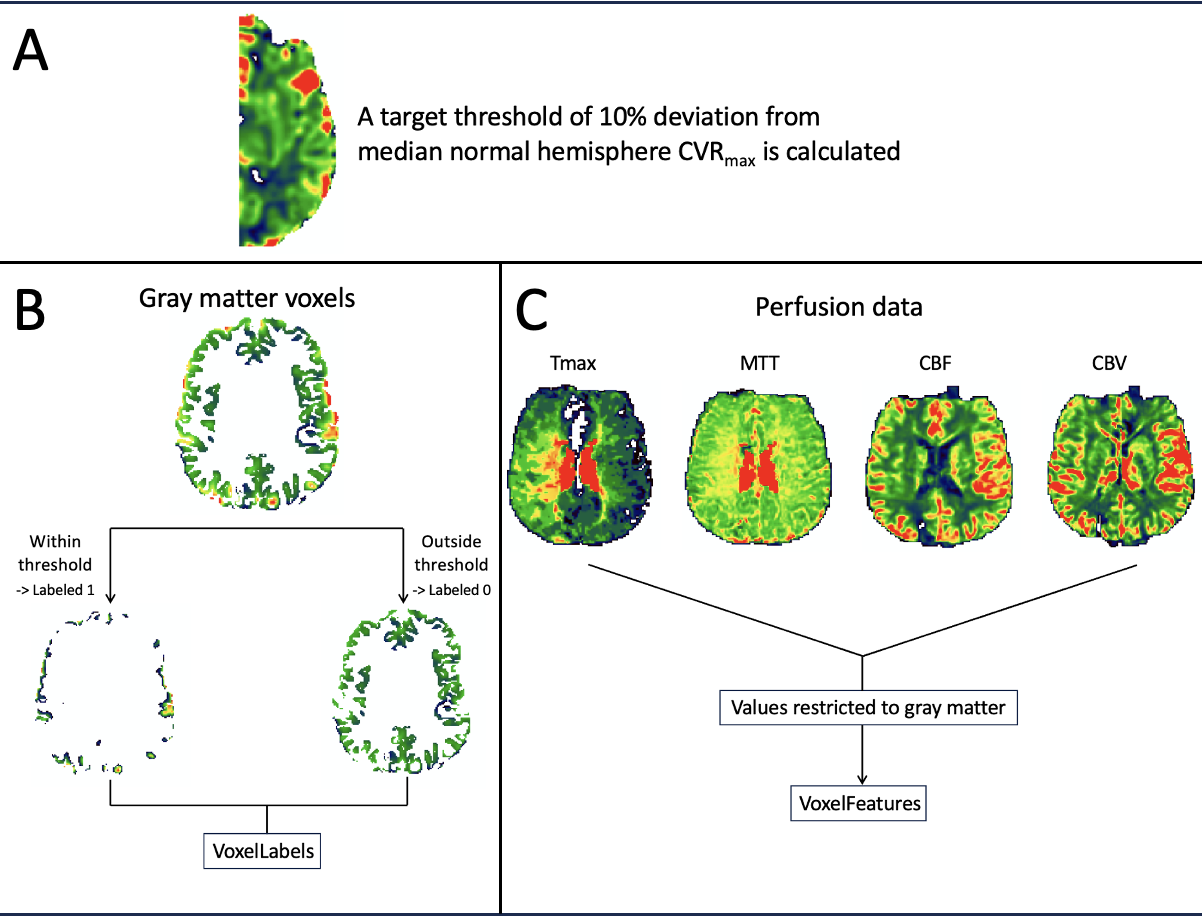
We propose to develop a novel normal candidate voxel search procedure, trained on contemporaneous DSC perfusion parameters, and tuned to identify brain-wide aggregates of voxels that best approximate the CVRmax of a ground-truth batch of normal hemispheric voxels. A random forest classifier (RFc) algorithm is optimized for this purpose in a population of angiographically-proven unilateral SOD undergoing contemporaneous DSC and ACZ-BOLD, targeting CVRmax within 10% of the normal hemisphere CVRmax.
Methods
16 patients with unilateral chronic SOD (mean age 52.4 years) underwent 22 ACZ-BOLD exams at 3T (SIEMENS Prisma, 64-channel head coil). Isotropic whole-brain T1-MPRAGE were obtained together with a 20-minute resting-state functional MRI (TR/TE=2150/36ms, voxel size=2x2x5mm3) ACZ-BOLD exam using one-gram ACZ dissolved in 10mL normal saline and infused over 3-5 minutes following 4–5-minute baseline BOLD as previously reported.3 DSC perfusion (T2* GRE-EPI, TR/TE=1740/40ms, FA=70°, voxel size=1.7x1.7x6mm3) were obtained in all patients.DSC were processed using a delay-insensitive deconvolution to generate Tmax, MTT, CBF, and CBV maps, which were registered to anatomic and BOLD images. CVRmax was extracted from the maximal, pre-binned denoised BOLD time-signal curve for each voxel at the per-TR level.
MATLAB (2022a, The MathWorks, Inc., Natick, Massachusetts, United States) was used to train a RFc algorithm with leave-one-out cross-validation (LOOCV). 13 of 22 studies were randomly selected for training and validation. Median normal hemispheric CVRmax was calculated and a whole-brain binary gray matter mask was created comprising voxels for which CVRmax was within 10% of this value. Tmax, MTT, CBF, and CBV per-voxel were concatenated into a voxel-feature array. The TreeBagger function was used to train the RFc using 100 trees to predict candidate voxels from voxel features (Figure 1). In each LOOCV iteration, 12/13 studies were used as training data with the remaining held out for validation. In each iteration, the median CVRmax of predicted voxels was compared to median normal hemispheric CVRmax. The model with the lowest percentage difference between ground-truth and candidate voxel median CVRmax was selected and applied to a test set of the remaining studies.
Results
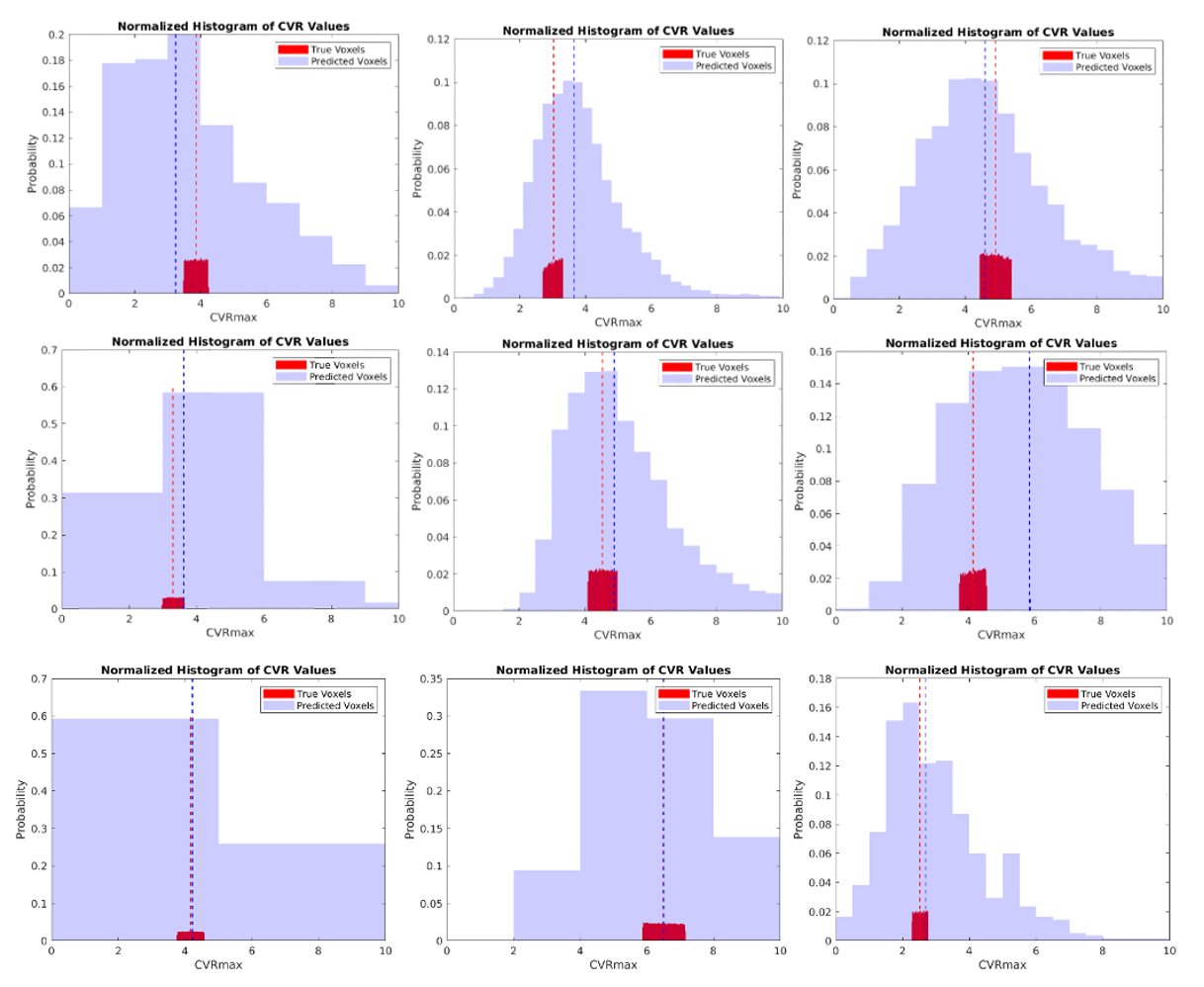
Among the gray matter voxels selected by the best RFc during LOOCV, the median CVRmax was 3.65, while the median CVRmax among the ground-truth (i.e., normal hemispheric) gray matter voxels within the threshold was 3.68, resulting in a difference of 0.70%.When used to predict gray matter voxels in the test cases, the median absolute percent difference was 7.9% (interquartile range 3.9% to 18.7%). Histograms of predicted and ground-truth voxel CVRmax are shown in Figure 2, with dashed lines indicating both population medians.
Discussion
We trained a RFc algorithm to identify candidate voxels whose median CVRmax best approximated median CVRmax of normal voxels in subjects with angiographically-proven unilateral SOD.The ease with which DSC perfusion imaging can be integrated into essentially any neuroimaging protocol facilitates use of our proposed approach in order to extend paradigms of hemodynamic failure using CVR estimates to patients with bilateral or indeterminate patterns of disease, or even without prior knowledge of disease distribution.
Our model can still be improved. Histogram examinations shows that the number of voxels predicted by the algorithm is much smaller than the number of voxels truly in our target threshold. Although the median CVRmax can be successfully approximated, newer iterations of the algorithm aim to better capture and spatially match ground-truth voxels.
Conclusion
We trained a RFc to identify candidate healthy voxels brain-wide, informed by perfusion signatures from DSC parametric maps.Acknowledgements
No acknowledgement found.References
1. Vagal AS, Leach JL, Fernandez-Ulloa M, et al. The acetazolamide challenge: techniques and applications in the evaluation of chronic cerebral ischemia. AJNR Am J Neuroradiol 2009;30:876-884
2. Wu J, Dehkharghani S, Nahab F, et al. Acetazolamide-augmented dynamic BOLD (aczBOLD) imaging for assessing cerebrovascular reactivity in chronic steno-occlusive disease of the anterior circulation: An initial experience. Neuroimage Clin 2017;13:116-122
3. Dogra S, Wang X, Gupta A, et al. Acetazolamide-augmented BOLD MRI to Assess Whole-Brain Cerebrovascular Reactivity in Chronic Steno-occlusive Disease Using Principal Component Analysis. Radiology 2023;307:e221473
4. Dogra S, Wang X, Gee JM, et al. Diaschisis Profiles in the Cerebellar Response to Hemodynamic Stimuli: Insights From Dynamic Measurement of Cerebrovascular Reactivity to Identify Occult and Transient Maxima. J Magn Reson Imaging 2023;58:1462-1469
5. Powers WJ, Clarke WR, Grubb RL, Jr., et al. Extracranial-intracranial bypass surgery for stroke prevention in hemodynamic cerebral ischemia: the Carotid Occlusion Surgery Study randomized trial. Jama 2011;306:1983-1992
Figures