3432
A Deep Learning Prediction Model for Deep Brain Stimulation Optimization by fMRI1GE HealthCare, Niskayuna, NY, United States, 2University Health Network and University of Toronto, Toronto, ON, Canada
Synopsis
Keywords: Task/Intervention Based fMRI, Parkinson's Disease
Motivation: Maximization of clinical benefits in the treatment of Parkinson’s disease (PD) using deep brain stimulation (DBS) requires clinical parameter optimization with a time-to-optimization per patient of ~1year.
Goal(s): To build a deep-learning-based model for the prediction of optimal DBS parameters from a single functional MRI response map obtained during DBS.
Approach: Multilayer perceptron based optimal DBS parameter prediction model was trained and tested (five-fold cross-validation) using features extracted by an autoencoder model from DBS-fMRI responses.
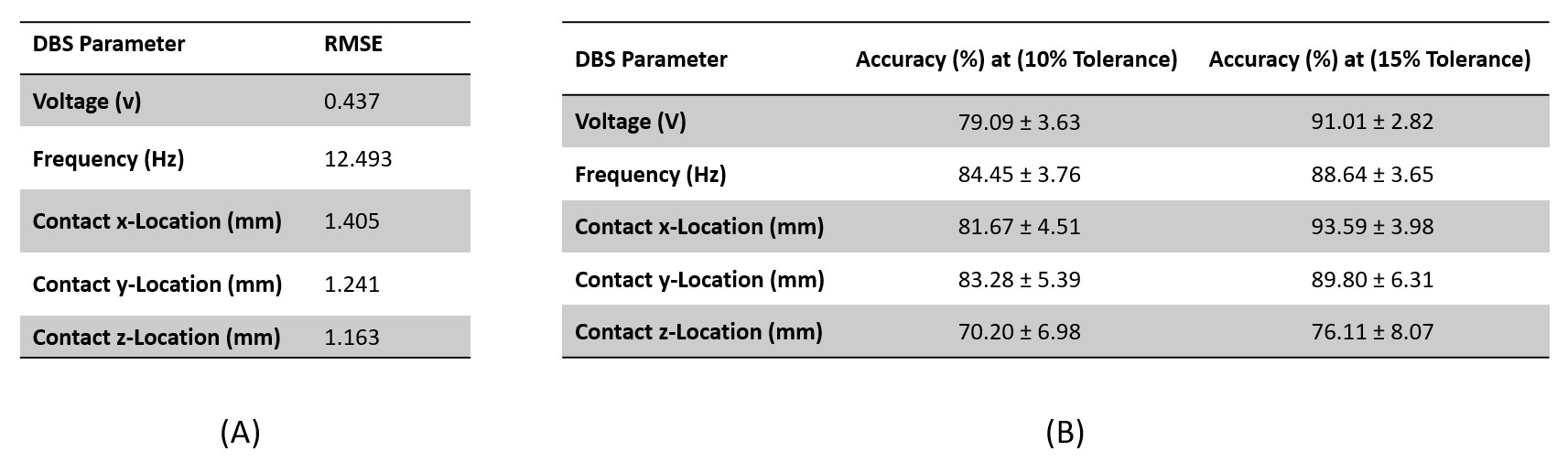
Results: Accuracies of 79.1%, 84.5%, 81.7%, 83.3% and 70.2% (at 10% deviation from ground truth) were achieved in the prediction of voltage, frequency, and x-y-z contact locations respectively.
Impact: This study gives an initial evaluation of a prediction model for DBS parameter optimization, which has the potential to reduce the time-to-optimization per patient from ~1 year to few hours during a single clinical visit, thereby reducing patient’s financial burden.
Introduction
Deep brain stimulation (DBS) is commonly used for the treatment of Parkinson’s disease (PD)1,2. The previous generation of DBS electrodes have four stimulation parameters – signal frequency, voltage, pulse width, and contact location – that require optimization to maximize patient clinical benefits and minimize adverse effects. In the current standard-of-care DBS optimization protocol, with a time-to-optimization per patient (TPP) of ~1 year, stimulation parameters are manually and sequentially adjusted until the physician determines an optimal parameter combination3,4. The TTP is even longer for newer generation of directional DBS electrodes with >16 parameter combinations5,6. Previously established functional magnetic resonance imaging (fMRI) and machine learning-assisted DBS parameter optimization for PD treatment has provided a way to rapidly classify a patient’s DBS parameter set as either optimal (patient clinical benefits are maximized and adverse effects are minimized) or non-optimal from their DBS-fMRI response maps7. The ability to rapidly and accurately classify multiple DBS parameters set as either optimal or non-optimal (based on their DBS-fMRI responses) can significantly reduce the TTP. However, the TTP can be further reduced significantly by a DBS parameter prediction model that is able to forecast a patient’s optimal DBS parameters using a single DBS-fMRI map as input. Here, we implement and test the performance of a deep-learning-based model for the prediction of optimal DBS parameters such as voltage, frequency and contact location.Materials and Methods
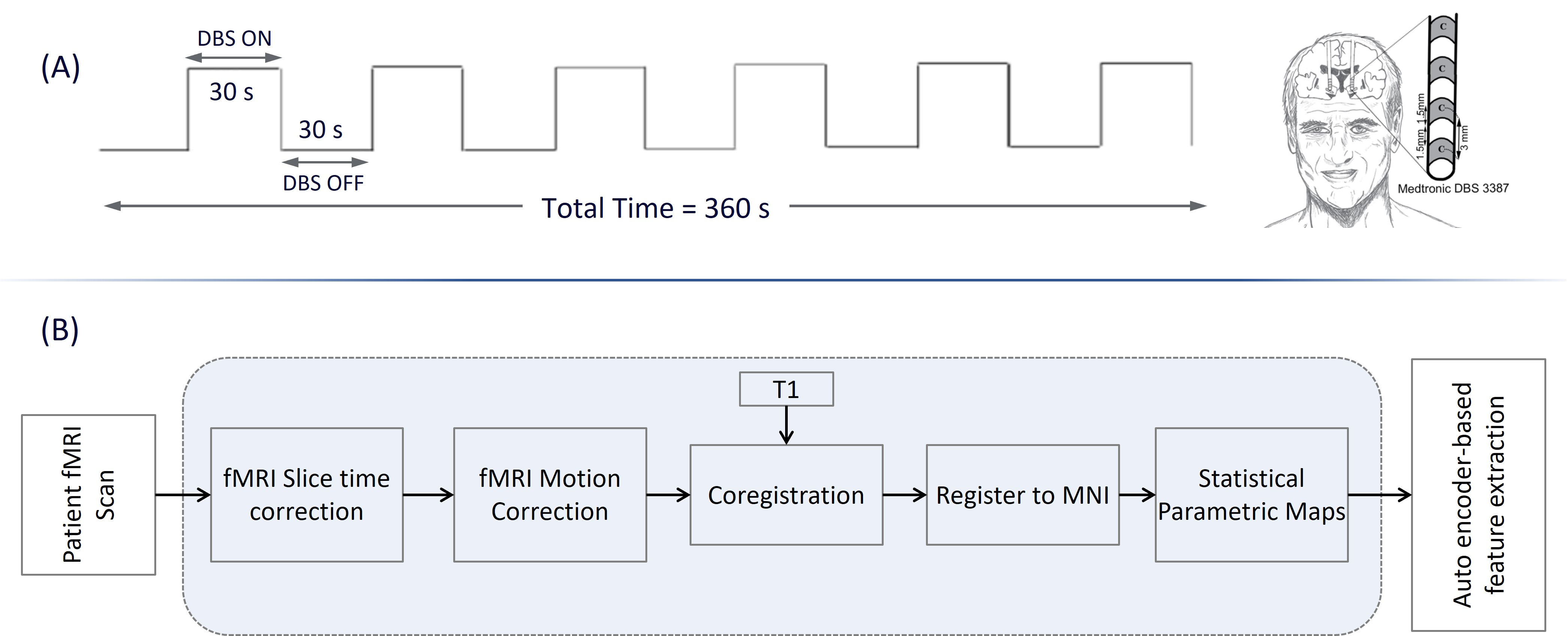
Our previously acquired 122 blood oxygenated level dependent DBS-fMRI data from 39 a priori clinically optimized PD patients (mean age=62.4±7.1, 20 males, 19 females) at 3.0 T were used in this work7.Single subject fMRI analyses: The DBS-fMRI processing pipeline adopted in this work has been previously described7,8 and is summarized in Figure 1. Briefly, all DBS-fMRI data was slice-time corrected, motion corrected, rigidly registered to a T1-weighted image, non-linearly registered to a standard space Montreal Neurological Institute brain, and spatially smoothed using a 6 mm Gaussian kernel after motion regression9. Statistical parametric maps were estimated from the preprocessed fMRI data using the designed 30-second DBS-ON/OFF paradigm. All data were processed using MATLAB (Mathworks−Natick, MA, USA) version of SPM12.
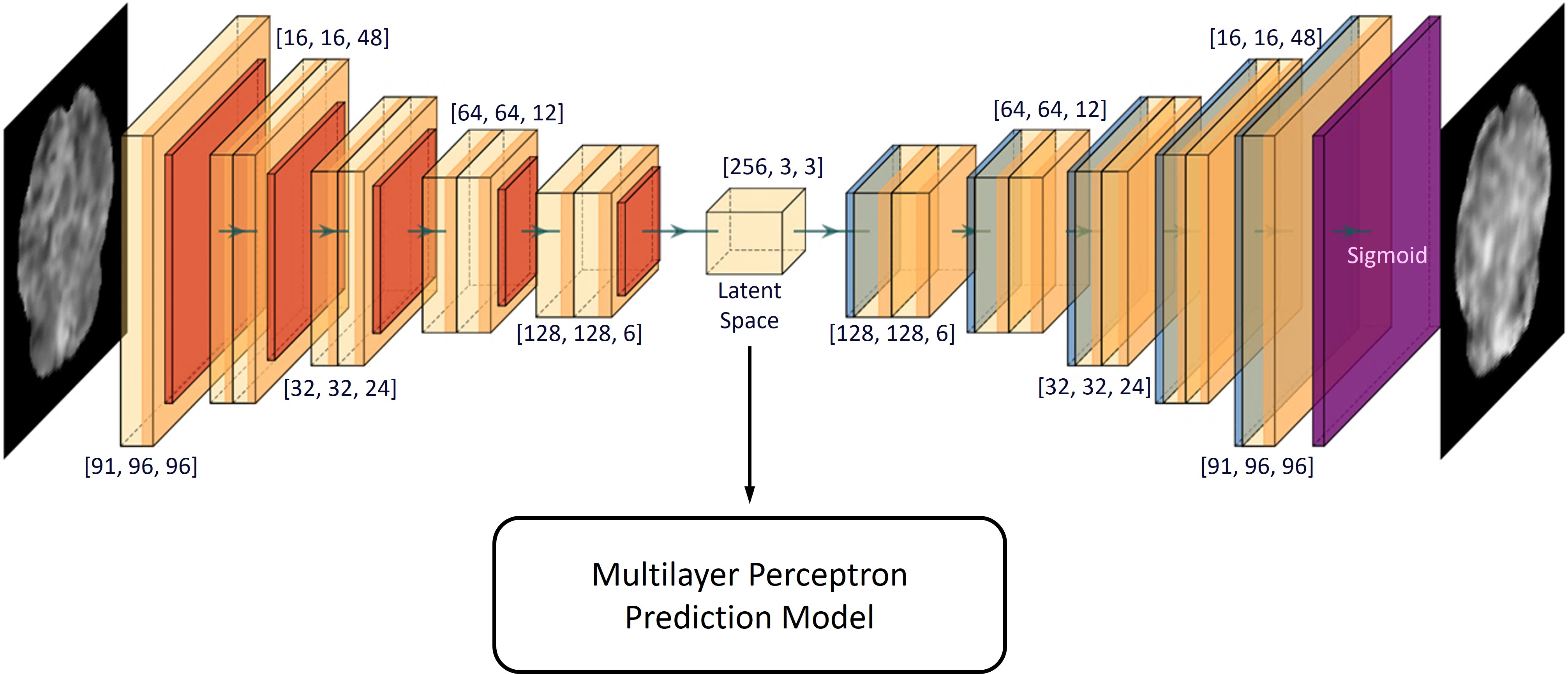
Model training and analyses: An autoencoder (AE) model was used to extract features from the DBS-fMRI maps as previously described8. A separate multilayer perceptron (MLP) prediction model was trained for each DBS parameter (voltage, frequency, and x-y-z location of optimal contact) over 100 epochs. The AE-MLP training network was composed of 8 hidden layers, and each neuron at any given hidden layer was fully connected to all neurons at the next hidden layer. All hidden layers (except the 8th layer) consisted of a linear layer and a ReLU activation function. Four dropout layers were added to the end of the first 4 blocks with feature dropout percentages of 25%, 15%, 15%, and 15%, respectively, to minimize potential over-fitting. The 8th layer was a fully connected layer that maps 16 neurons to 1 neuron, which represents the final predicted DBS parameter value (Figure 2). A mean square error loss function was used for training the model. The pulse width parameter was excluded as all data were acquired at 60 µs. We calculated the prediction accuracy at 10% and 15% tolerance - predictions were correct if they were within ±10% and ±15% respectively from the ground truth - within a five-fold cross-validation framework.
Results and Discussion
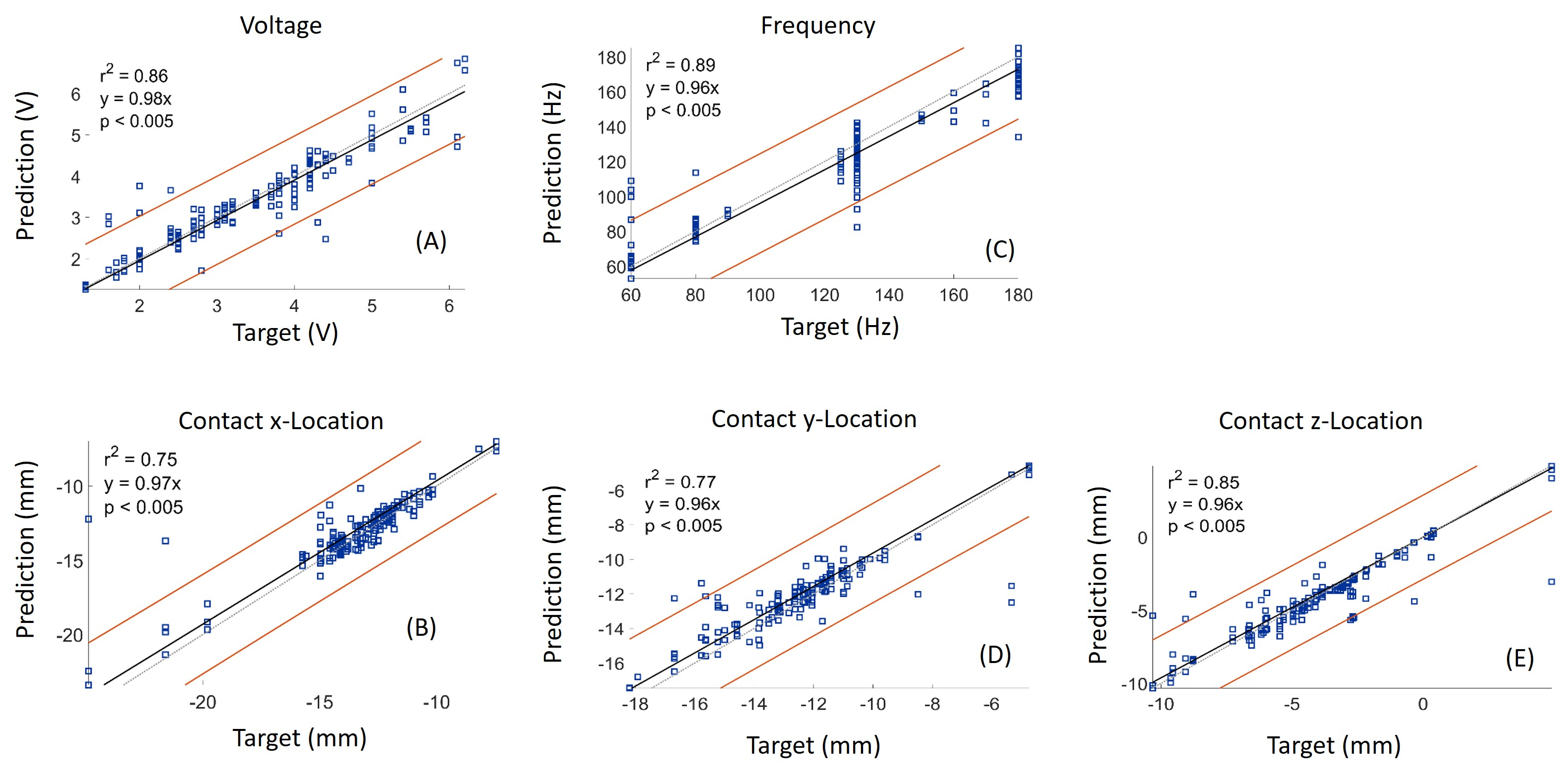
A comparison of the predicted DBS parameters and target values are shown in Figure 3 for the voltage, frequency and contact location DBS parameters. The root mean square error of the prediction model yielded values that are within tolerable clinical limits (Figure 4A). As expected, DBS prediction accuracy at 15% tolerance was higher than the accuracy at 10% tolerance, with the lowest accuracy (76.11%) recorded in the prediction of z-location of the optimal contact (Figure 4B). We acknowledge that the small size and variety of our data may reduce the accuracy of the current AE-MLP prediction model when deployed for the optimization of newer DBS electrodes with directionality. However, as we continue to gather more DBS-fMRI data from directional DBS electrodes, we anticipate that the performance of the prediction model will improve. These preliminary results show the effectiveness of our DBS parameter prediction model that has the potential to reduce the TTP from ~1 year to a couple of hours during a single clinical visit. This is timely as new DBS electrodes are being implemented clinically.Conclusion
The deep-learning prediction model shows promising results for DBS parameter optimization and has the potential to reduce the TTP from ~1 year to few hours during a single clinical visit.Acknowledgements
Research reported in this work was supported by the National Institute of Neurological Disorders and Stroke (NINDS) of the National Institutes of Health under award number 1R01NS133433-01 and Michael J. Fox foundation under grant number MJFF-008877. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.References
1. Lozano, A. M. et al. Deep brain stimulation: current challenges and future directions. Nat Rev Neurol 15, 148–160 (2019).
2. Limousin, P. & Foltynie, T. Long-term outcomes of deep brain stimulation in Parkinson disease. Nat Rev Neurol 15, 234–242 (2019).
3. Picillo, M., Lozano, A. M., Kou, N., Puppi Munhoz, R. & Fasano, A. Programming Deep Brain Stimulation for Parkinson’s Disease: The Toronto Western Hospital Algorithms. Brain Stimulation 9, 425–437 (2016).
4. Picillo, M., Lozano, A. M., Kou, N., Munhoz, R. P. & Fasano, A. Programming Deep Brain Stimulation for Tremor and Dystonia: The Toronto Western Hospital Algorithms. Brain Stimulation 9, 438–452 (2016).
5. Krauss, J. K. et al. Technology of deep brain stimulation: current status and future directions. Nat Rev Neurol 17, 75–87 (2021).
6. Schüpbach, W. M. M. et al. Directional leads for deep brain stimulation: Opportunities and challenges. Movement Disorders 32, 1371–1375 (2017).
7. Boutet, A. et al. Predicting optimal deep brain stimulation parameters for Parkinson’s disease using functional MRI and machine learning. Nat Commun 12, 3043 (2021).
8. Ajala, A. et al. Autoencoder-Based Deep Learning Classifier for Deep Brain Stimulation Parameter Settings by fMRI. in OHBM 2022 Annual Proceedings (2022).
9. Mazaika, P. K., Hoeft, F., Glover, G. H., Reiss, A. L., & others. Methods and software for fMRI analysis of clinical subjects. Neuroimage 47, S58 (2009).
Figures