3424
7T fMRI connectivity analysis reveals decreased cerebellar motor function in MS patients1Spinoza Centre for Neuroimaging, Amsterdam, Netherlands, 2Computational Cognitive Neuroscience and Neuroimaging, Netherlands Institute for Neuroscience, Amsterdam, Netherlands, 3Biomedical Engineering and Physics, Amsterdam UMC, Amsterdam, Netherlands, 4Neurology, MS Center Amsterdam UMC location VUmc, Amsterdam, Netherlands, 5Institutes of Neurology and Healthcare Engineering, University College London, London, United Kingdom
Synopsis
Keywords: Functional Connectivity, Multiple Sclerosis, cerebellum
Motivation: The cerebellum is a prevalent lesion site in Multiple Sclerosis but due to lack of acquisition methods its function remains understudied in MS.
Goal(s): Our goal was to compare the cerebellar motor (network) function of Multiple Sclerosis patients to Healthy Controls using 7T fMRI.
Approach: We employed a B1-shimmed 7T fMRI protocol and submillimetre anatomical acquisitions. This enabled us to identify cerebellar function during a motor task and identify subject specific regions of interest to analyse cerebellar motor network connectivity.
Results: Our methods revealed decreased connectivity as well as lower motor task activation in Multiple Sclerosis patients compared to Healthy Controls.
Impact: Our results demonstrate the use of 7T-fMRI to study cerebellar function in patients with Multiple Sclerosis. The differences found in motor and resting state activation may contribute to the overall understanding of the role of cerebellar function in Multiple Sclerosis.
Introduction
The human cerebellum forms an important part of the clinically relevant sensory and motor networks1,2. Cerebellar damage across multiple neurological diseases such as multiple sclerosis (MS) often leads to motor impairment3. Specifically, the cerebellum is a prevalent lesion site MS patients3. Research suggests that cerebellar pathology can be an early biomarker for the severity of MS4. Therefore, understanding the underlying mechanisms through studying cerebellar function can be of high clinical interest. While functional MRI (fMRI) can noninvasively measure brain function, fMRI in the cerebellum remains underused in patients as damage is difficult to quantify due to the thin and highly-foliated cerebellar cortex. In the neocortex, fMRI methods have revealed altered network connectivity in MS patients both in cognitive and motor domains5, 6, 7. Task-based fMRI studies show higher activity in MS patients compared to healthy controls (HCs)8,9. It has been hypothesised that increased functional activity compensates for structural damage when performing a task12,13. However, the direction of change depends on the stage of the disease as a decrease in activation is reported in patients with severe disability8,10. Studies specifically looking at cerebellar connectivity are rare, with preliminary studies showing that compared to HCs, MS patients show reduced connectivity between the sensory motor cortex and the contralateral cerebellar hemisphere7,11. Recent 7T-fMRI results show reduced activation in the cerebellum during a lower limb task14. While HCs show somatomotor network hubs in the anterior and posterior lobe of the cerebellum2,15, it remains unclear whether this activation pattern is altered in MS16,17. This study compares functional changes within the cerebellum including motor task responses and network connectivity in MS patients compared to HCs using 7T fMRI and submillimetre resolution anatomical images.Methods
6 MS patients (2F) and 3 HCs (1F), ages (M=55,SD=9.29), were scanned using a 7T-Philips MRI-scanner (8Tx/32Rx whole-head coil). Selected patients showed signs of cerebellar neurodegeneration. The following was acquired for all participants (Fig-1A): A 3D-EPI slab covering the cerebellum (1mm-isotropic,TR/TE=3288ms/21ms, SENSE=2.6/3.27-AP/RL FOV=192x60x192mm3, α=20°) while participants performed a 5min motor task (right hand flex 10s-ON 10s-OFF) and a 7min resting state task (fixation on cross) (Fig-1B). A 0.4mm isotropic MP2RAGE covering the cerebellum (; 5.65/1.88; TI1/TI2, 1000ms/2900ms ; TI1/TI2, α =7°/5, FOV=210×120×60mm3 , sensitivity encoding y/z, 1.5/1) with prospective motion correction (realigning reconstructed fat navigators in real time to update the FOV, 2mm isotropic fat navigator (3D EPI with fat- selective binomial excitation pulse;; 5.65/1.88; Tvol=550ms; α=1°; sensitivity encoding y/z, 4/2; Tacq=0.55s, FOV=240×240×120mm3). A whole-head 1.0 mm-isotropic MP2RAGE-sequence (TR/TE=2.3ms/6.2ms, TI1/TI2=800/2700,TRvolume=5500ms, α=7°/5°,FOV=230x230x185)18. Previously calculated group B1+ phase offsets were used to optimise B1+ over the cerebellum20. FMRI data were motion/distortion-corrected. 0.4mm isotropic MP2RAGE images were denoised using a spatially adapted filter19,21. A first level GLM (Flex>rest, Z>3.1 P<0.05) was fitted to the motor task using FSL20. A cerebellar motor function mask17 was projected into the anatomical space of each participant. The mask was manually divided into the left/right and anterior/posterior cerebellar lobes to identify relevant clusters (Fig2-A). A spherical seed mask (radius=4px) was created using the voxel with the maximum Z-score resulting from the motor task (Fig-3-A). Mean time-courses were extracted from this seed and used as input for a first level GLM (Motor-seed>rest, Z>3.1, P<0.05) investigating cerebellar connectivity.Results
The flexing task resulted in significant (Z>3.1,P<0.05) bilateral activation in the cerebellum for all HCs, contrary to less than 50% of MS patients (Fig-2B/C). Activation levels were lower in MS: maximum Z-scores were higher in HCs (Right Anterior: MED=7.85, SD=0.5, Posterior: MED=5.37, SD=0.62) compared to MS patients (Right Anterior: MED=4.28,SD=2.07, Posterior: MED=4.22, SD=1.08). The resting state seed based GLM analysis revealed all HCs and MS patients had significant (Z>3.1,P<0.05) connectivity within the cerebellar parts of the motor network (Fig3-B/C). Mean connectivity Z-scores were higher for HCs in all four cerebellar motor ROIs compared to MS patients (Fig-3B).Discussion and Conclusion
The motor task consistently engaged cerebellar motor areas in HCs whereas MS patients showed lower and inconsistent activation in both the anterior and posterior lobes. Conversely, some comparisons in the cerebral cortex show higher fMRI activation for MS patients during flexing tasks12,14. The resting state analysis indicates decreased connectivity in MS patients but a larger cohort and a more in depth analysis are necessary to identify specific differences in motor network connectivity.In conclusion, we successfully compared fMRI activation during a motor task in MS patients and HCs in the human cerebellum using 7T fMRI. Our high-resolution anatomical data enabled us to employ subject specific ROIs for each participant in our resting state connectivity analysis.
Acknowledgements
This study was supported by an NWO TTW VIDI grant (VI.Vidi.198.016).References
1.Xue et al. 2021 2. Boillat et al, 2020 3.Weissert et al, 2017 4.Weinshenker et al, 1991 5.Rocca et al, 2022 6.Eijlers 2019 7.Rocca 2009 8.Rocca 2005 9.Reddy et al, 2002 10.Ciccarelli et al, 2006 11.Saini et al, 2004 12.Rocca,2002 13.Lenzi ,2007 14.Strik et al, 2021 15.Van der Zwaag et al, 2013 16.Buckner et al, 2011 17.King et al, 2019 18.Marques et al, 2010 19.Advanced Normalization Tools software,2010 20.Mark et al, 2012 21. Priovoulos et al, 2023
Figures
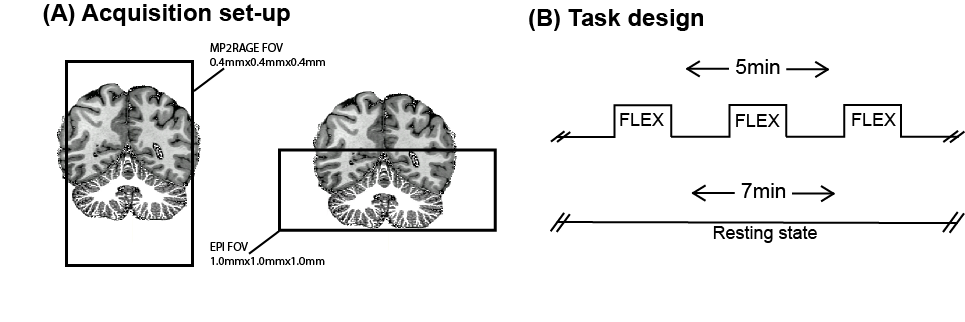
Figure 1: (A) The FOV of the 0.4mm isotropic MP2RAGE acquisition and the FOV of the 1mm isotropic EPI overlaid onto the whole brain 1mm isotropic MP2RAGE including the cerebellar white matter segmentation. (B) The motor task design: 15 cycles of a right hand flex (10s) alternated by 10s of rest. The resting state task design: 7 minutes in which the participant was asked to focus on a cross.
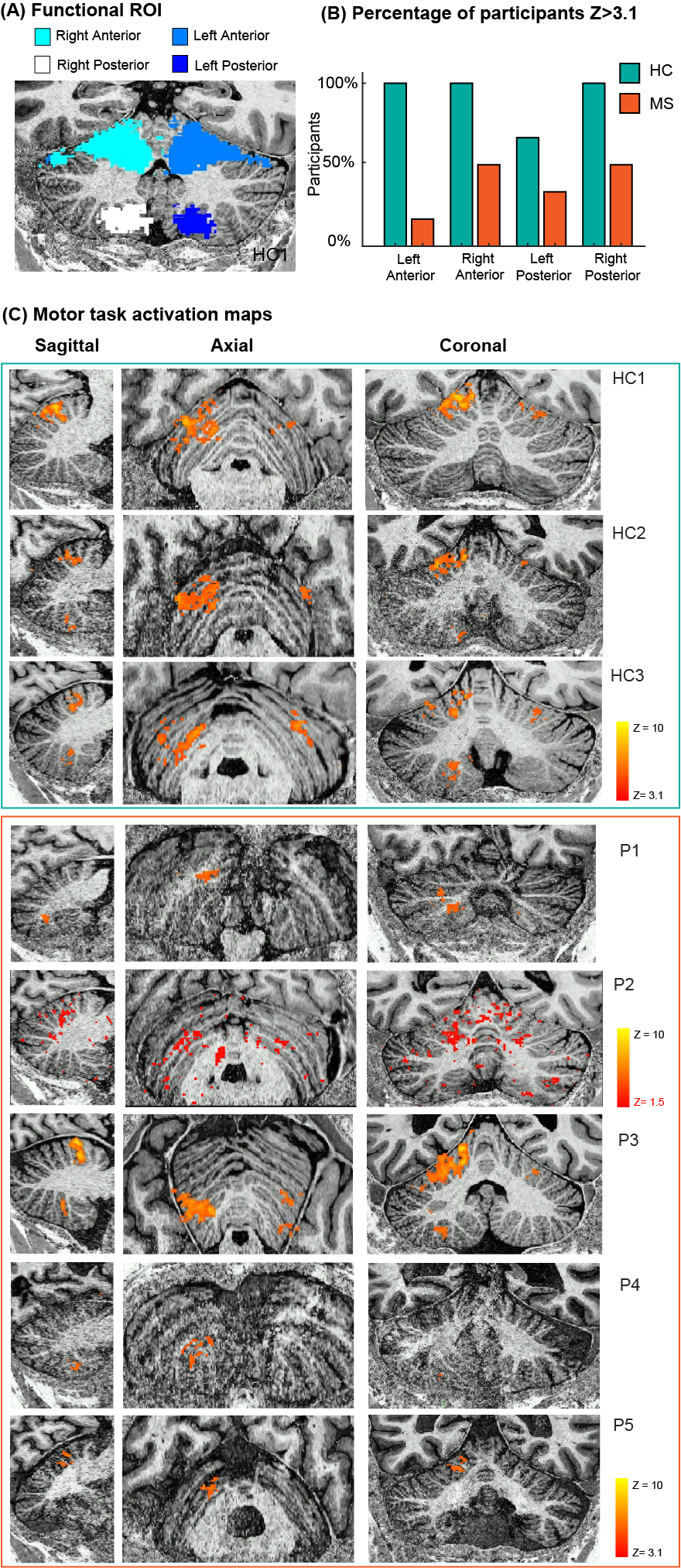
Figure 2: (A)The functional motor ROI registered into the 0.4mm isotropic anatomical space of the participant. (B)The percentage of participants with a significant cluster in the cerebellar ROIs. (C) Motor task activation Z>3.1 overlaid onto the 0.4mm isotropic anatomical space of the participant. HC=Healthy control MS = MS Patient. *Participant 6 is not visualised due to a failed anatomical acquisition.
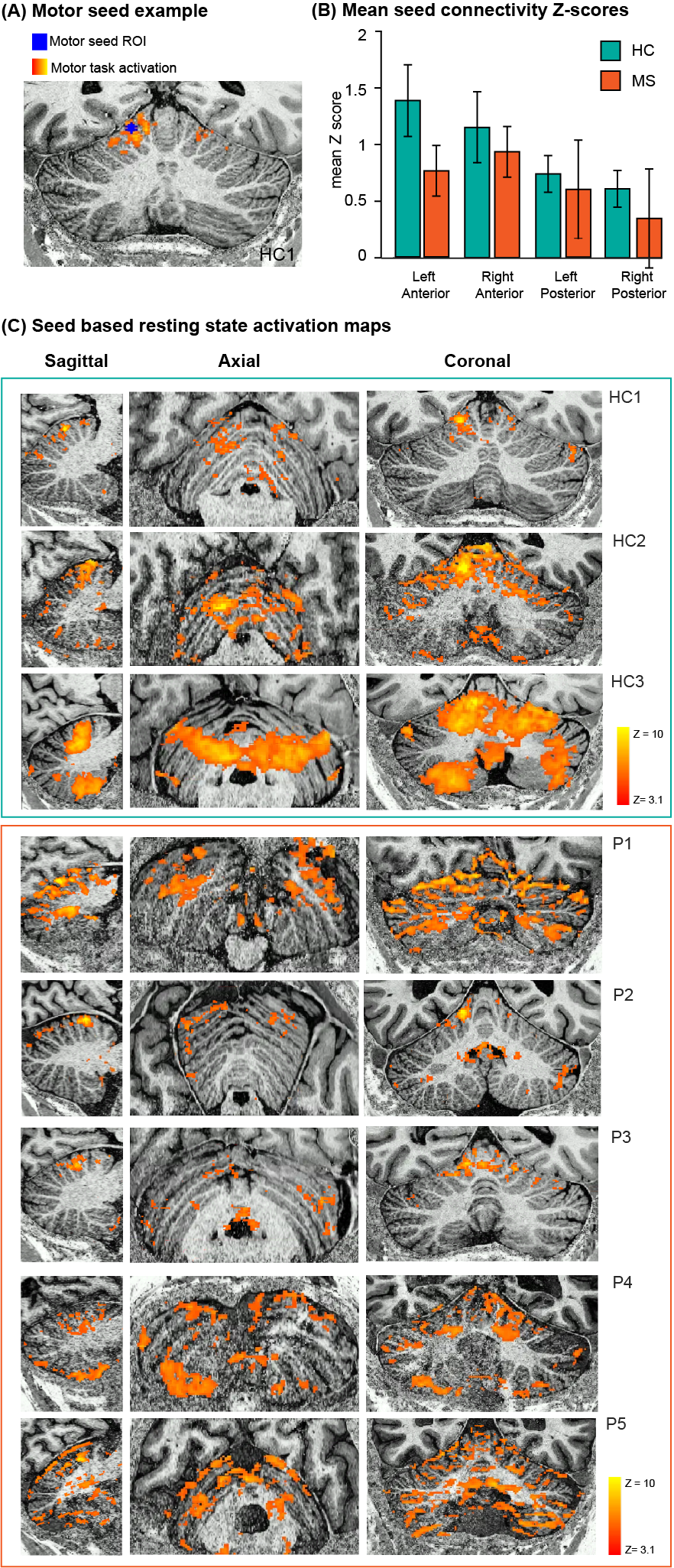
Figure 3: (A)Motor seed of HC1 overlaid on the functional motor task activation and the 0.4mm isotropic anatomical acquisition. (B) Mean z-scores of the seed based resting state GLM. (C) Seed based resting state activation Z>3.1 overlaid onto the 0.4mm isotropic anatomical space of the participant. HC=Healthy control MS = MS Patient. *Participant 6 is not visualised due to a failed anatomical acquisition.