3407
Reliability of fetal 4D flow in healthy volunteers and patients with suspected congenital cardiovascular anomalies1Radiology, University of Colorado Anschutz Medical Campus, Aurora, CO, United States, 2Department of Radiology, Children's Hospital Colorado, Aurora, CO, United States, 3Pediatric Cardiology, University of Colorado Anschutz Medical Campus, Aurora, CO, United States, 4Bioengineering, University of Colorado Anschutz Medical Campus, Aurora, CO, United States
Synopsis
Keywords: Fetal, Fetus, 4D flow
Motivation: Fetal 4D flow provides useful information related to cardiovascular structure and function, but its reliability is not yet defined.
Goal(s): Here, we seek to define the accuracy, precision, internal consistency, and repeatability of fetal 4D flow.
Approach: Pregnant women in their third trimester with healthy developing fetuses (N=22) and fetuses with suspected cardiovascular anomalies (N=12) were scanned with 2D phase contrast and 4D flow sequences. Quantitative flow metrics were compared.
Results: 4D flow underestimated net flow in the great vessels relative to 2D-PC, but had reasonable precision, internal consistency, and repeatability. Fetal 4D flow can reliably measure percentage contributions from various vascular territories.
Impact: Fetal 4D flow allows for quantitative hemodynamic evaluation of the fetal cardiovascular system with good precision, internal consistency, and repeatability. Flow was underestimated relative to 2D-PC, therefore presently percent contribution from various vascular territories is the most appropriate clinical endpoint.
Background & Introduction
The fetal cardiovascular system has several distinctive features that work together to deliver oxygenated blood from the placenta to the brain and body of the fetus. While typically evaluated with fetal echocardiography, MRI can provide a comprehensive assessment of fetal cardiovascular anatomy and function. Prior studies evaluating fetal blood flow used multiple, carefully placed individual 2D phase contrast (PC) planes1, employed an iteration of the slice-to-volume approach, acquiring multi-planar, multi-slice 2D PC-MRI reconstructed in 3D2, or more recently used a Doppler ultrasound-gated 4D flow acquisition3,4. Here, we sought to evaluate the accuracy, precision, internal consistency, and repeatability of flow metrics quantified from fetal 4D flow in healthy controls and patients with known or suspected congenital cardiovascular anomalies.Methods
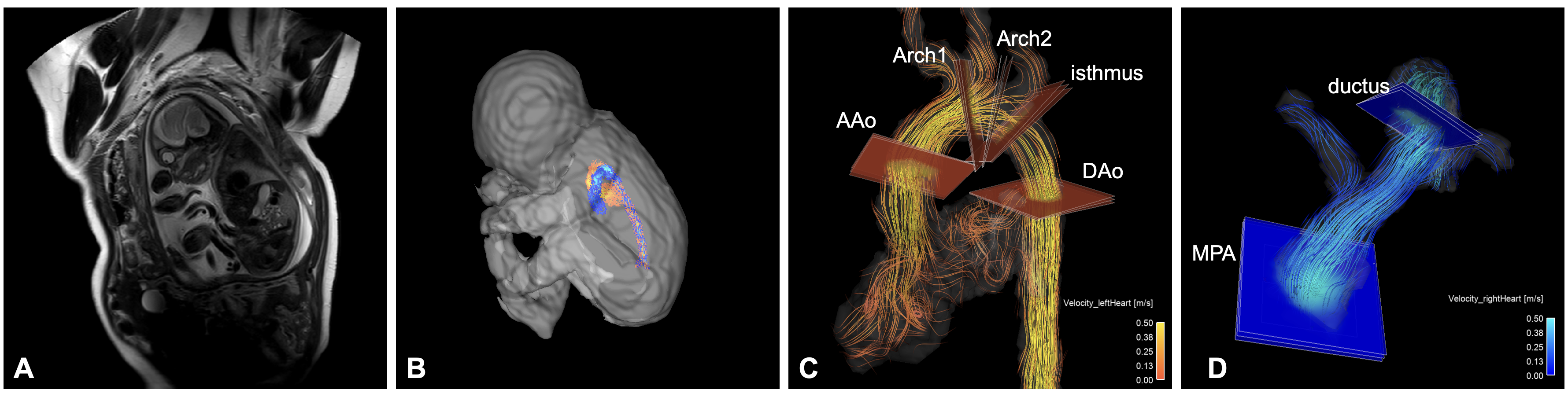
With IRB approval, 22 healthy pregnant volunteers (maternal age=34±4 years, gestational age, GA=34±2 weeks) and 12 patients with suspected congenital cardiovascular abnormalities from fetal echocardiography (age=33±6 years, GA=35±3 weeks) were prospectively recruited and scanned at 3T (Philips Ingenia). Fetal cardiac gating was achieved with a MR-compatible Doppler ultrasound device (Northh Medical)5,6. Localizers covering the entire fetus were acquired and segmented to determine fetal body mass7. 4D flow data encompassing the fetal heart and major vessels were acquired with fixed isotropic resolution=2.5mm3, VENC=150cm/s, temporal resolution=38-50ms and duration=132-263s. When possible (dictated by fetal motion, available time, and gating signal stability), 2D PC data were acquired in planes perpendicular to the descending aorta, ascending aorta, main pulmonary artery, and ductus arteriosus with in plane resolution=1.25×1.25mm2, slice thickness=5mm, VENC=150cm/s, temporal resolution=24-30ms, and duration=30-37s/slice.Custom Matlab code and 3D slicer was used for pre-processing and segmentation of 4D flow data. Using EnSight (Ansys), flow was quantified in three adjacent planes separated by ~1mm in seven vascular territories (Fig 1). The mean across measurement planes for each territory was normalized by fetal mass to obtain flow in mL/min/kg.
2D PC analysis was performed in Circle CVI. Contours were placed around the vessel of interest, and net flow was quantified and converted to mL/min/kg based on fetal heart rate and mass.
Statistical analyses were performed in GraphPad Prism:
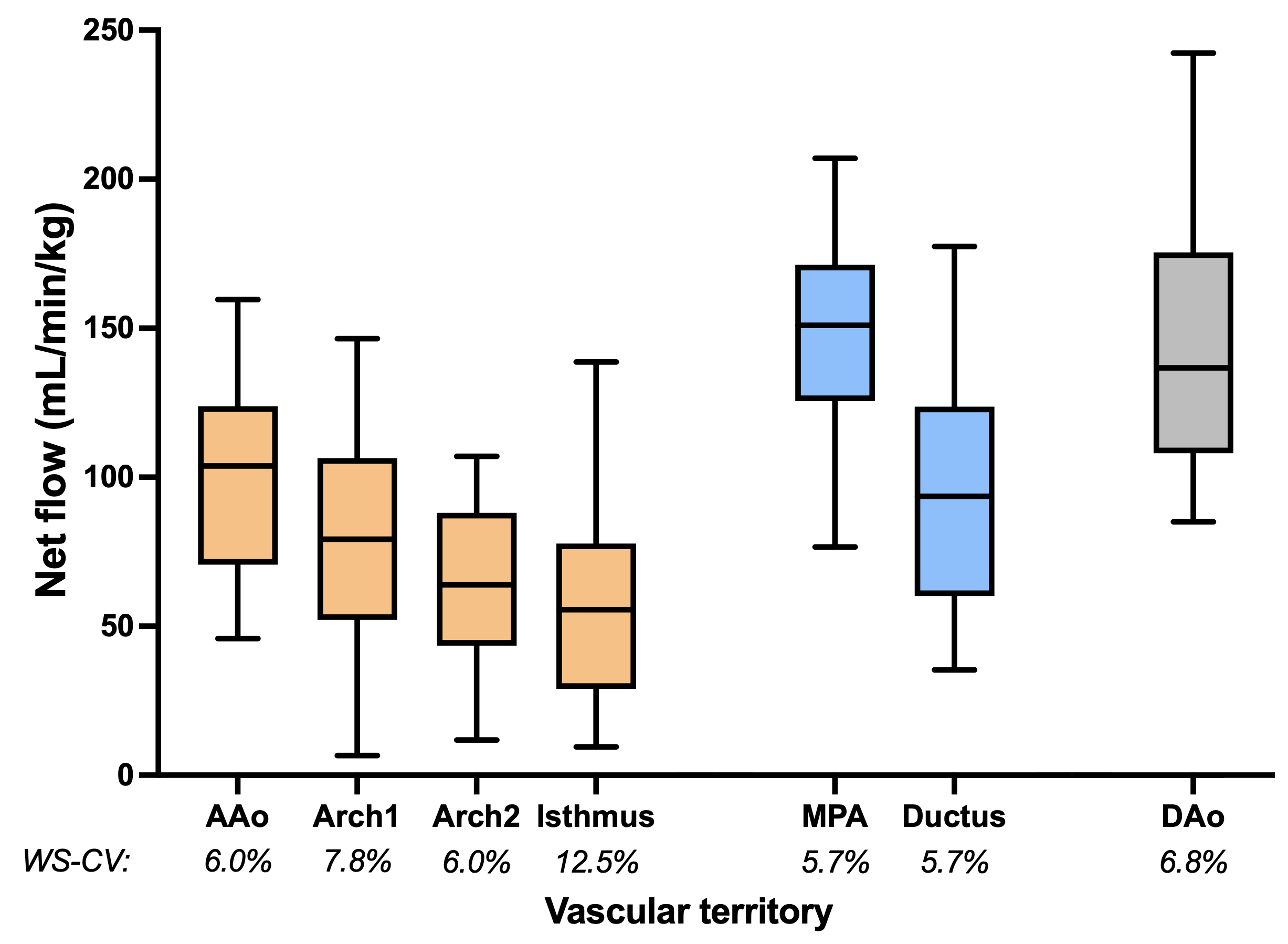
- 4D flow precision: Within-subject coefficient of variation (WS-CV) was computed across adjacent measurement planes in all healthy volunteers (N=22).
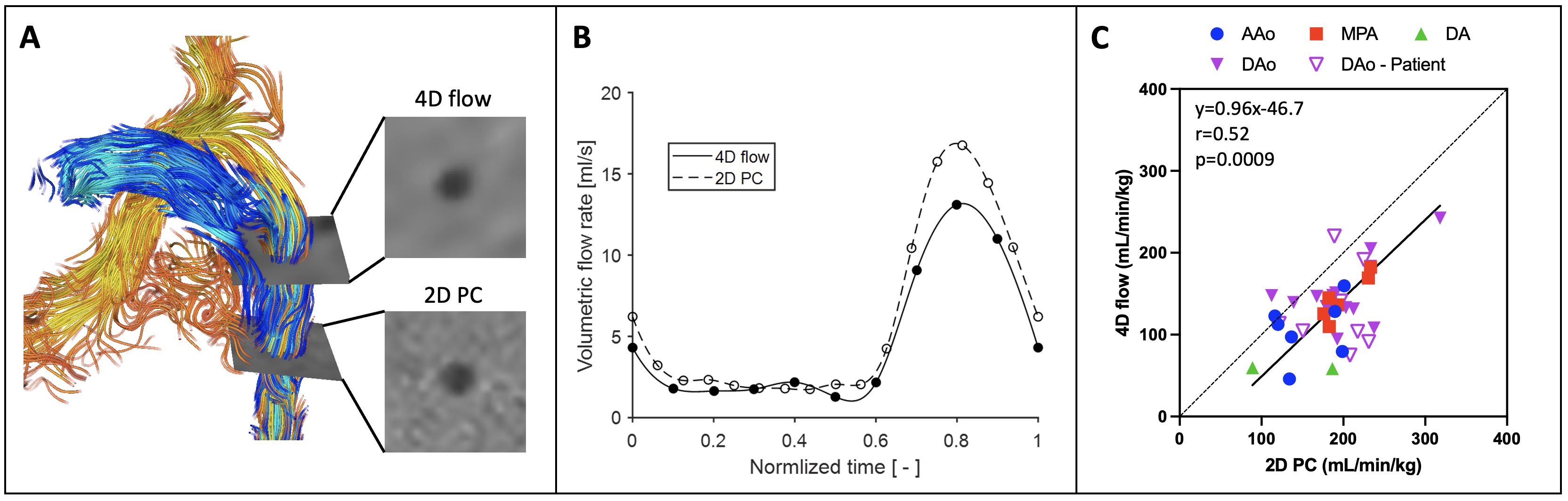
- 4D flow accuracy: Net flow derived from 4D flow was compared to 2D PC in participants in which both data were available (healthy=17, patient=8) via orthogonal regression and Pearson’s correlation.
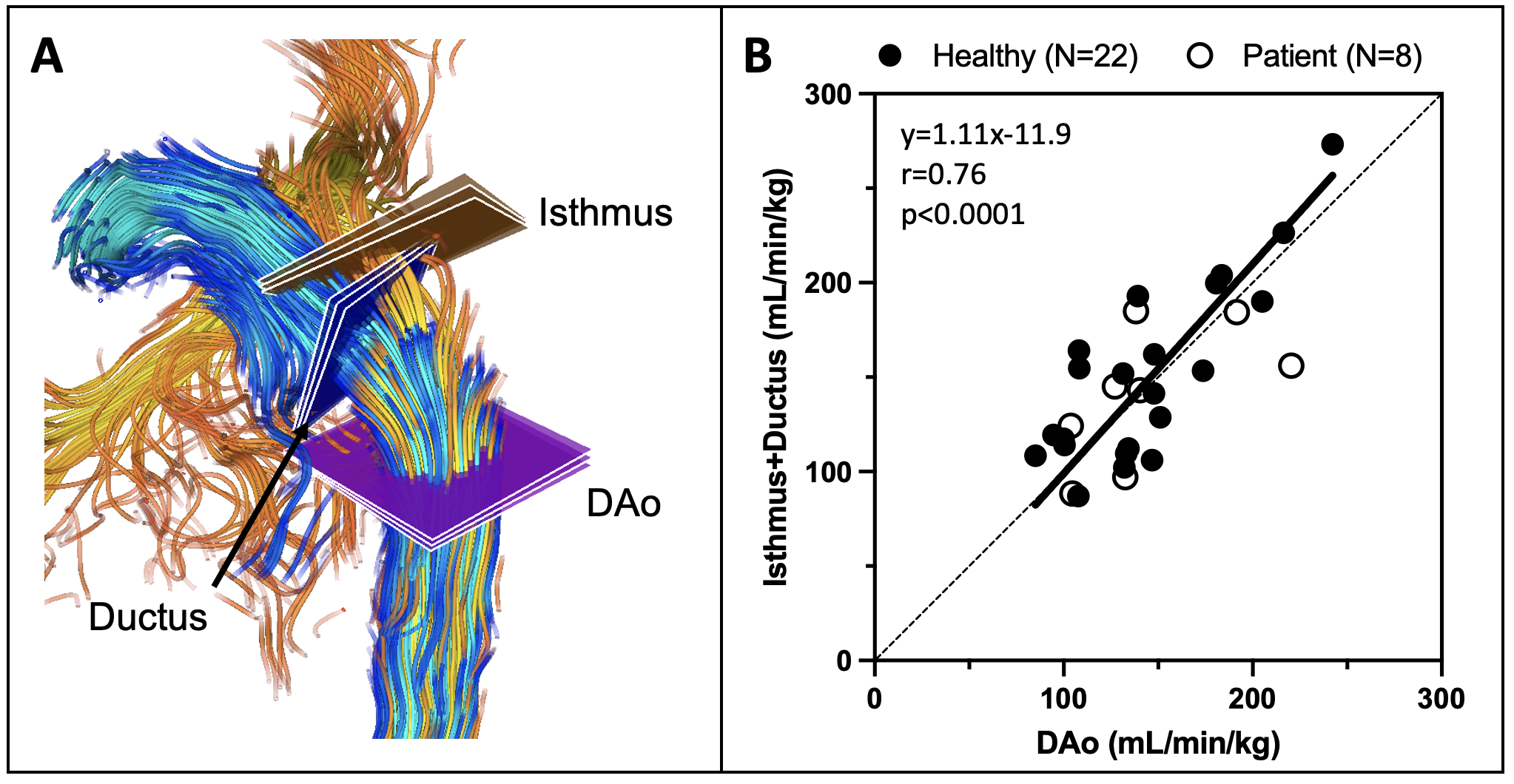
- 4D flow internal consistency (based on conservation of mass): The sum of net flow at the aortic isthmus and ductus arteriosus was compared to flow measured in the descending aorta (healthy=22, patient=8).
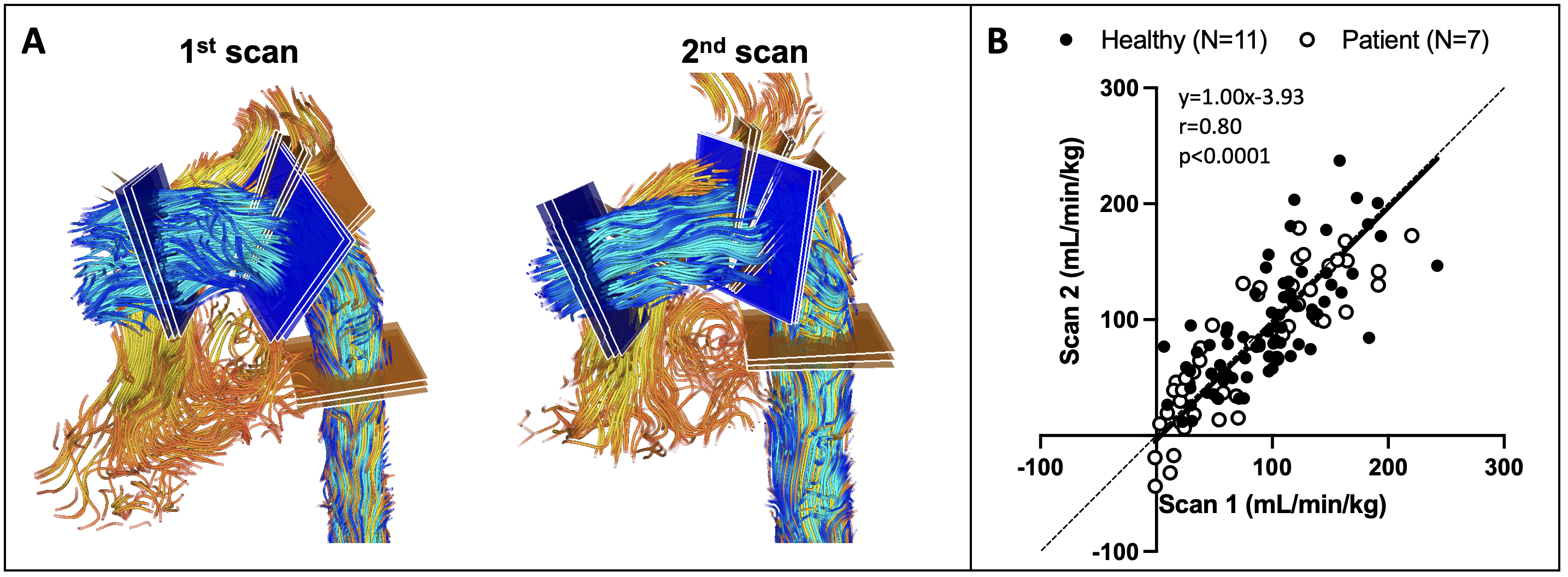
- 4D flow repeatability: Comparison between two separate acquisitions within the same scan session was performed (healthy=11, patient=7) by orthogonal regression, Pearson’s correlation, and Bland-Altman analysis.
Results
Across all participants, the mean±SD fetal mass was 2549±475g and fetal heart rate was 141±10bpm. In healthy volunteers, the mean combined ventricular output was 253±44 mL/min/kg. As expected in the healthy fetuses, flow decreases from to ascending aorta to arch to isthmus due to branching head vessels, then increases in the descending aorta post ductal and aortic arch convergence (Fig 2). Across all segments, WS-CV<13% and average WS-CV=7.2%. Blood flow was underestimated by 4D flow compared to 2D PC results by approximately 46.7mL/min/kg (Fig 3). Mass conservation had an average 19±12% difference between ductus arteriosus + isthmus flow versus descending aorta (Fig 4). Hemodynamic parameters quantified from repeated 4D flow acquisitions had good agreement in both healthy controls and patients (Fig 5), with bias=3.8mL/min/kg and limits of agreement=-62.8 to 70.4mL/min/kg.Discussion
4D flow MRI successfully evaluated the fetal circulatory hemodynamics in third trimester fetuses. Overall, there was good precision of 4D flow hemodynamic parameters across measurement planes. In line with prior reports8, 4D flow underestimated flow compared to 2D PC, likely due to its reduced spatial and temporal resolution. Motion during the longer 4D flow acquisition could also lead to errors in blood flow quantification. In general, mass conservation was comparable to a prior report in fetal sheep (~14% difference)8, however the measurement locations differ. Across the 18 participants included in repeatability analysis, there was negligible bias, but relatively wide limits of agreement, which could likely be improved with advanced motion compensation.Conclusion
Fetal 4D flow underestimated absolute blood flow relative to 2D PC, but maintained internal consistency in both healthy developing fetuses and those with suspected cardiovascular anomalies, with good precision and repeatability. Percent contribution from various vascular territories is the most appropriate clinical endpoint at present, however future advances in acquisition and motion compensation strategies may improve accuracy and repeatability.Acknowledgements
Supported by NIH/NCATS Colorado CTSA Grant Number KL2 TR002534, the Colorado Center for Translational Science Institute Translational Methods Grant TM-T-23-197 with support from NIH/NCATS Colorado CTSA Grant Number UL1 TR002535, and seed funding from the Colorado Fetal Care Center.References
- Prsa M, Sun L, van Amerom J, Yoo SJ, Grosse-Wortmann L, Jaeggi E, Macgowan C, Seed M. Reference ranges of blood flow in the major vessels of the normal human fetal circulation at term by phase-contrast magnetic resonance imaging. Circ Cardiovasc Imaging. 2014; 7(4):663-670.
- Roberts TA, van Amerom JFP, Uus A, Lloyd DFA, van Poppel MPM, Price AN, Tournier JD, Mohanadass CA, Jackson LH, Malik SJ, Pushparajah K, Rutherford MA, Razavi R, Deprez M, Hajnal JV. Fetal whole heart blood flow imaging using 4D cine MRI. Nat Commun. 2020; 11(1):4992.
- Knapp, J., Tavares de Sousa, M., Lenz, A. et al. Fetal 4D flow MRI of the great thoracic vessels at 3 Tesla using Doppler-ultrasound gating: a feasibility study. Eur Radiol 2023; 33:1698–1706.
- Englund EK, Fujiwara T, Smith S, Cuneo B, Moghari MH, Meyers ML, Friesen RM, Browne LP, Barker AJ. 4D flow MRI for investigation of fetal cardiovascular hemodynamics in healthy development and ductal dependent lesions. Proceedings of the International Society for Magnetic Resonance in Medicine 31st Scientific Meeting and Exhibition. 2023; 1243.
- Kording F, Yamamura J, de Sousa MT, Ruprecht C, Hedström E, Aletras AH, Ellen Grant P, Powell AJ, Fehrs K, Adam G, Kooijman H, Schoennagel BP. Dynamic fetal cardiovascular magnetic resonance imaging using Doppler ultrasound gating. J Cardiovasc Magn Reson. 2018; 20:17.
- Kording F, Schoennagel BP, de Sousa MT, Fehrs K, Adam G, Yamamura J, Ruprecht C. Evaluation of a Portable Doppler Ultrasound Gating Device for Fetal Cardiac MR Imaging: Initial Results at 1.5T and 3T. Magn eason Med Sci. 2018; 17:308-317.
- Baker PN, Johnson IR, Gowland PA, Hykin J, Harvey PR, Freeman A, Adams V, Worthington BS, Mansfield P. Fetal weight estimation by echo-planar magnetic resonance imaging. Lancet. 1994; 343(8898):644–645.
- Schrauben, E.M., Saini, B.S., Darby, J.R.T. et al. Fetal hemodynamics and cardiac streaming assessed by 4D flow cardiovascular magnetic resonance in fetal sheep. J Cardiovasc Magn Reson 2019; 21:8.
Figures