3406
Augmented hemodynamic quantification of the fetal cardiovascular system using 4D flow MRI and slice to volume 3D black blood imaging1Department of Radiology, Section of Pediatric Radiology, Children's Hospital Colorado, University of Colorado Anschutz Medical Campus, Aurora, CO, United States, 2Department of Fetal Cardiology, Evelina London Children’s Hospital, London, United Kingdom, 3Department of Biomedical Engineering and Imaging Sciences, King’s College London, London, United Kingdom, 4Department of Pediatrics, Section of Cardiology, Children's Hospital Colorado, University of Colorado Anschutz Medical Campus, Aurora, CO, United States, 5Department of Bioengineering, University of Colorado Anschutz Medical Campus, Aurora, CO, United States
Synopsis
Keywords: Flow, Fetus, 4D flow
Motivation: Small blood vessel size relative to spatial resolution in fetal 4D flow MRI makes segmentation and flow quantification difficult.
Goal(s): To quantify blood flow from fetal 4D flow using black blood imaging-based segmentation and to compare hemodynamic results to 4D flow-only approach. We hypothesize black blood will provide better flow delineation for complex anatomies.
Approach: The great vessels were segmented from 4D flow and black blood for volunteers and coarctation cases; flow volumes were compared after alignment of segmentations.
Results: Black blood underestimated flow volume but captured vessel geometry and flow features 4D flow segmentation missed in several cases of coarctation.
Impact: While the combination of black blood imaging and fetal 4D flow did not offer flow quantification comparable to conventional 4D flow approach, its potential of capturing coarctation flow may assist prenatal diagnosis of coarctation, which is challenging solely with ultrasound.
Introduction
Fetal cardiovascular magnetic resonance (CMR) is a promising tool to better diagnose cardiovascular anomalies at the prenatal stage1. Time-resolved, three-dimensional (3D) phase-contrast CMR (4D flow CMR) could be useful since it can comprehensively capture 3D hemodynamics in the fetal heart and great vessels2. Given the size of fetal anatomy, high spatial resolution is desirable for fetal CMR. Simultaneously, to minimize fetal motion during acquisition, scan times for fetal 4D flow should be as short as possible. This necessity, however, limits the achievable spatial resolution to ~2.5mm3, making vessel segmentation and thus flow quantification challenging. On the other hand, 2D T2-weighted black blood (BB) imaging with 3D slice-to-volume reconstruction can provide motion-corrected images of blood vessels at a higher spatial resolution (~0.75mm3)3. We hypothesize that the use of BB images as a segmentation mask for 4D flow data will provide flow quantification comparable to conventional 4D flow-based segmentations and may improve hemodynamic analysis of fetal data, where segmentation of the extracardiac anatomy is especially challenging. Therefore, this study evaluates the flow quantification performance of BB-based 4D flow CMR in comparison to a conventional 4D flow analysis in healthy and suspected coarctation of the aorta fetuses.Methods
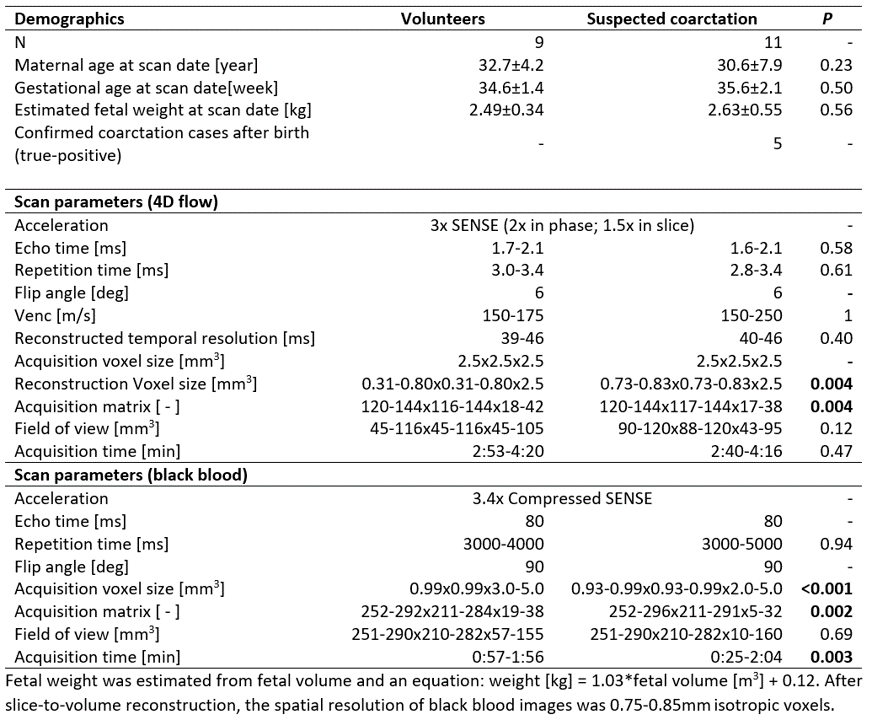
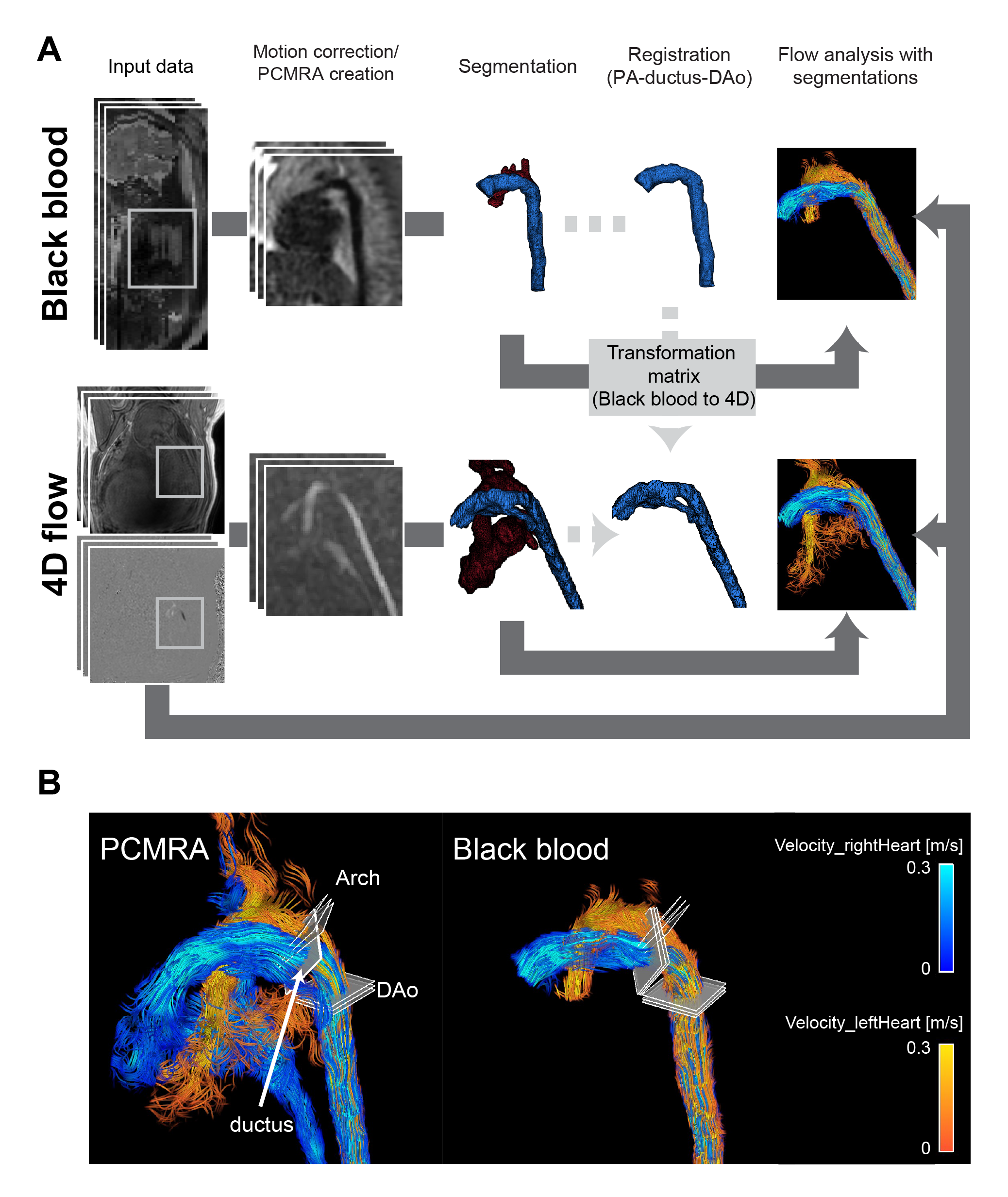
Out of 57 prospectively recruited participants who underwent 4D flow CMR scans (Doppler ultrasound gated, gradient recalled echo) on a Philips Ingenia 3T scanner, 9 healthy fetuses and 11 fetuses with suspected coarctation were identified to have multi-planar BB (T2-weighted single shot turbo spin echo) data (Table 1). Figure1A illustrates the analysis workflow. 4D flow data was processed using a custom MATLAB tool to obtain phase-contrast MR angiography (PCMRA)4. For BB images, 3-5 stacks acquired in different orientations were motion corrected and reconstructed in 3D using SVRTK5. The aorta, pulmonary arteries (PA), and ductus arteriosus (ductus) were then manually segmented for both BB and PCMRA by the same observer using 3D-slicer6. To align the BB segmentation to the 4D flow data, rigid registration was utilized7. The BB segmentation of the PA+ductus+descending aorta (DAo) was registered to the corresponding PCMRA segmentation to obtain a transformation matrix from BB to 4D flow coordinates. The transformation matrix was then applied to the entire BB segmentation including the aorta to mask the 4D flow velocity field using the BB images. Subsequently, the net flows at the ductus, distal aortic arch (arch), and DAo were quantified using both the PCMRA and BB segmentations (Fig.1B). Internal consistency was also evaluated based on mass conservation (ductus + arch flows vs. DAo flow). Streamlines, the ductus insertion point, flow direction at the arch, and aortic shape were visually compared between PCMRA, BB, and postnatal CT (when available). PCMRA and BB were compared using paired t-tests and linear regression using MATLAB R2021a and R4.3.1, with p<0.05 considered statistically significant.Results
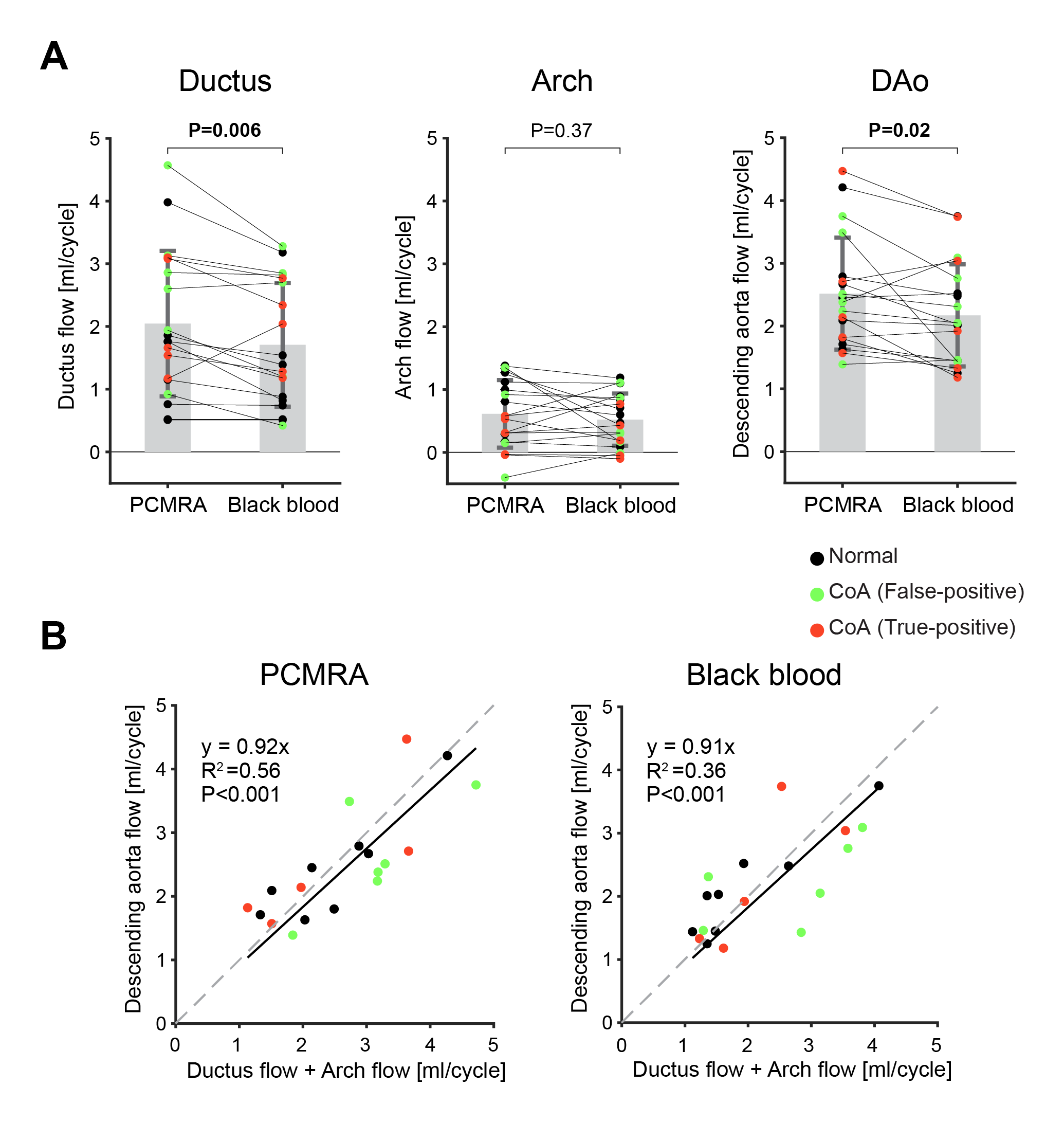
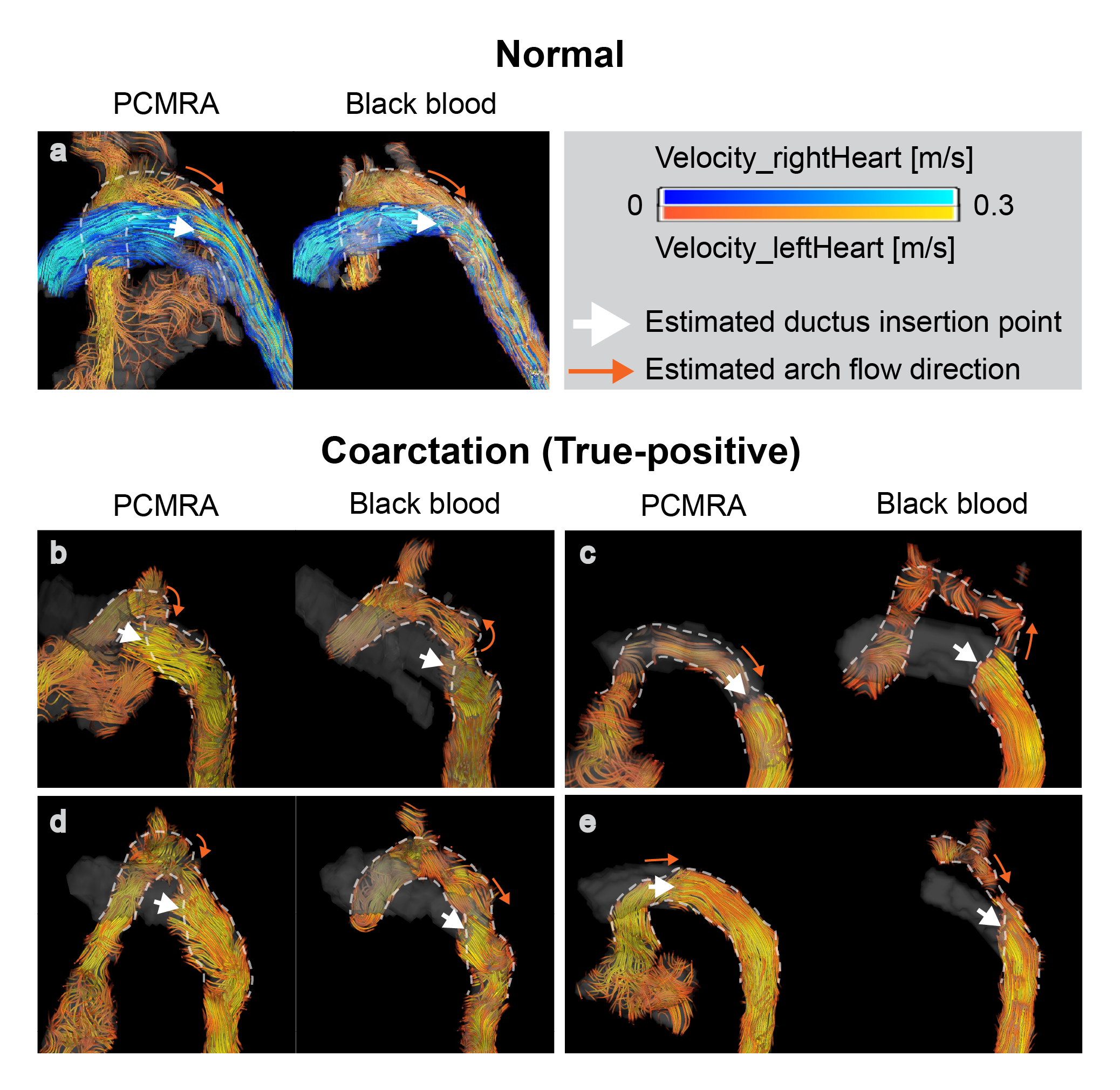
Out of 11 suspected coarctation cases, 5 were confirmed to have coarctation by postnatal echo (true-positives) while the remaining cases were found to be normal (false-positives). Registration was not successful for one volunteer and excluded from the analysis. Significantly lower net flows were detected for BB at the ductus (2.1±1.2ml in PCMRA vs 1.7±1.0ml in BB; P=0.006) and DAo (2.5±0.9ml in PCMRA vs 2.2±0.8ml in BB; P=0.02) (Fig. 2A). The slope of regression analysis for internal consistency were comparable (y=0.92x, P<0.001 vs. y=0.91x, <0.001) with a lower R2 value in BB (0.56 vs. 0.36; Fig.2B). Visual comparison found remarkabe differences between PCMRA and BB segmentations in 4/5 true-positive coarctation cases (Fig.3). BB-based geometry/flow exhibited closer agreement to postnatal CT (Fig.4).Discussion
Contrary to our hypothesis, net flows at the ductus and DAo were significantly lower, and internal consistency appears to have equivalent or worse behavior when using BB-based segmentation for 4D flow data. This could result from differences in spatial resolution between the reconstructed BB and 4D flow. In addition, motion artifacts in the 4D flow and a rigid registration approach may have led to discrepancies in the BB registration process. Nonetheless, the potential capability of better delineating the arch structure in complex patient cases implies BB images can possibly supply valuable anatomic/flow information in combination with 4D flow. Protocol optimization and motion corrected 4D flow as well as refinement of registration technique would further clarify the role of BB to augment fetal 4D flow8.Conclusion
The combination of BB imaging and 4D flow MRI was able to measure net flows, despite a possible systematic underestimation of flow. BB images may also be able to characterize the geometric/flow features of coarctation better than PCMRA. Performance in true-positive coarctation cases needs further investigation in a larger population.Acknowledgements
This work was supported by American Heart Association Grant #23POSTCHF1025444/2023 (PI: Fujiwara)
References
1. Nafisi BA, van Amerom JFP, Forsey J, Jaeggi E, Grosse-Wortmann L, Yoo SJ, Macgowan CK, Seed M. Fetal circulation in left-sided congenital heart disease measured by cardiovascular magnetic resonance: a case-control study. J Cardiovasc Magn Reson. 2013;15:65. doi:10.1186/1532-429X-15-65.
2. Knapp J, Tavares de Sousa M, Lenz A. Herrmann J, Zhang S, Kording F, Hergert B, Adam G, Bannas P, Schoennagel BP. Fetal 4D flow MRI of the great thoracic vessels at 3 Tesla using Doppler-ultrasound gating: a feasibility study. Eur Radiol. 2023;33:1698-1706. doi:10.1007/s00330-022-09167-7
3. Lloyd DF, Van Poppel MP, Pushparajah K, et al. Analysis of 3-Dimensional Arch Anatomy, Vascular Flow, and Postnatal Outcome in Cases of Suspected Coarctation of the Aorta Using Fetal Cardiac Magnetic Resonance Imaging. Circ Cardiovasc Imaging. 2021;14:e012411. doi: 10.1161/CIRCIMAGING.121.012411
4. Bock J, Kreher B, Hennig J, Markl M. Optimized pre-processing of time-resolved 2D and 3D phase contrast MRI data. Proceedings of International Society for Magnetic Resonance in Medicine. 2007;15:3138.
5. Uus A, Zhang T, Jackson LH, Roberts TA, Rutherford MA, Hajnal JV, Deprez M. Deformable slice-to-volume registration for motion correction of fetal body and placenta MRI. IEEE Trans Med Imaging. 2020;39(9):2750-2759. doi:10.1109/TMI.2020.2974844.
6. Fedorov A, Beichel R, Kalpathy-Cramer J, Finet J, Fillion-Robin J-C, Pujol S, Bauer C, Jennings D, Fennessy FM, Sonka M, Buatti J, Aylward SR, Miller JV, Pieper S, Kikinis R. 3D Slicer as an Image Computing Platform for the Quantitative Imaging Network. Magn Reson Imaging. 2012;30(9):1323-41. DOI: 10.1016/j.mri.2012.05.001.
7. Jenkinson M, Smith SM. A global optimization method for robust affine registration of brain images. Med Image Anal. 2001;5:143-156. doi:10.1016/S1361-8415(01)00036-6.
8. Goolaub, DS, Xu J, Schrauben E, Sun L, Roy CW, Marini D, Seed M, Macgowan CK. Fetal flow quantification in great vessels using motion-corrected radial phase contrast MRI: comparison with cartesian. J Magn Reson Imaging. 2021;53(2):540-551. doi:10.1002/jmri.27334.Figures