3404
Fetal Blood Flow Measurements at Low Field (0.55T) using Metric Optimized Gating1School of Biomedical Engineering and Imaging Sciences, St. Thomas’ Hospital, King's College London, London, United Kingdom, 2London Collaborative Ultra high field System (LoCUS),, King's College London, London, United Kingdom, 3Department of Congenital Heart Disease, Evelina Children’s Hospital, London, United Kingdom, 4Centre for the Developing Brain, School of Biomedical Engineering & Imaging Sciences, King's College London, London, United Kingdom, 5MR Research Collaborations, Siemens Healthcare Limited, Camberley, United Kingdom, 6Department of Women & Children's Health, King's College London, London, United Kingdom, 7Smart Imaging Lab, Radiological Institute, University Hospital Erlangen, Erlangen, Germany
Synopsis
Keywords: Fetal, Fetus
Motivation: To allow diagnosis of CHD at low field strengths in order to increase the accessibility of MRI.
Goal(s): To demonstrate that acquiring 2D phase contrast sequences in utero at 0.55T is possible.
Approach: Acquire 2D Phase contrast sequences, optimize sequences parameters, and perform metric optimized gating and flow measurements
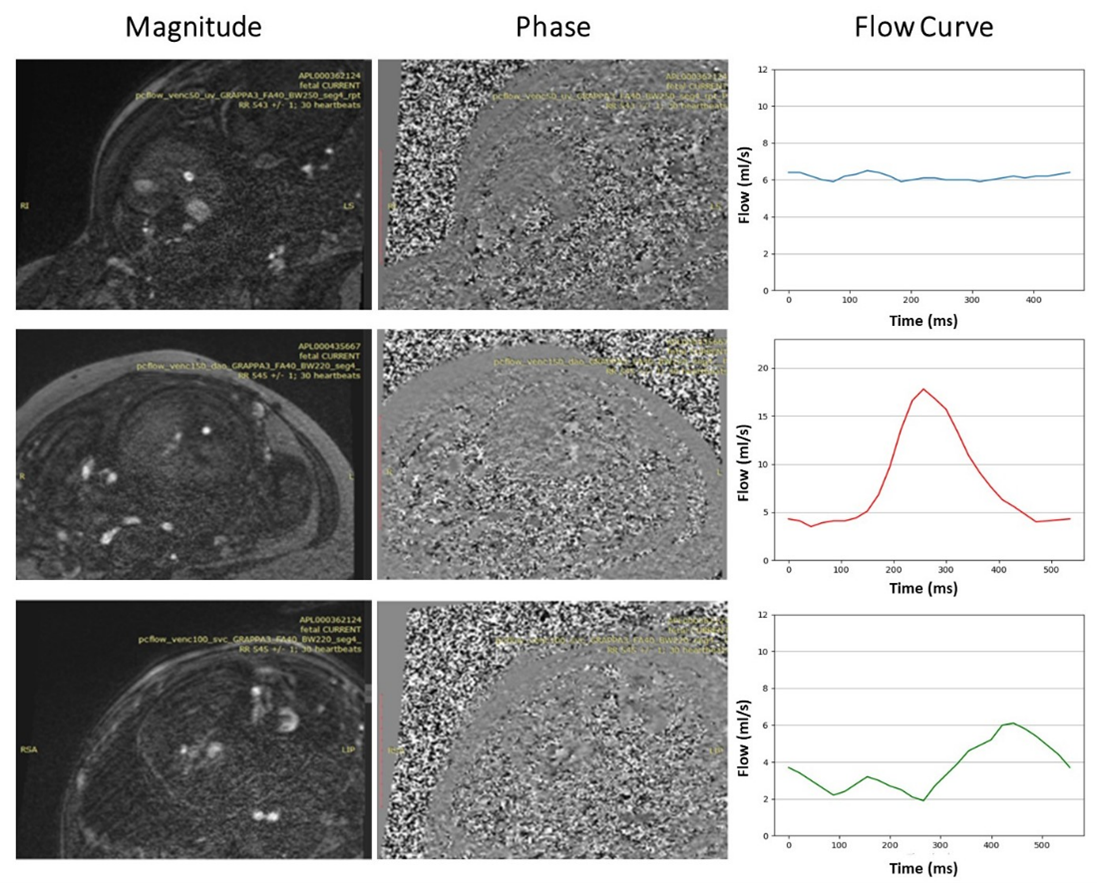
Results: Umbilical vein, descending aorta, and superior vena cava flow in utero measurements were calculated.
Impact: Fetal flow measurements provide additional information on the complex hemodynamics in complex CHD cases – potentially enhancing antenatal counselling and postnatal surgery planning. Optimizing these for emerging low field MRI scanners widens their availability.
Introduction
Congenital heart disease (CHD) is a common congenital disorder, affecting nearly 1% of births per year1. Diagnosing CHD prenatally allows to create a treatment plan and thus improves survival rates and outcome 2. Visualizing and quantifying blood flow in the major vessels can provide insights into subtle changes in the fetal circulation and can in addition inform on how altered fetal blood flow impacts fetal brain development3. Fetal cardiovascular magnetic resonance (FCMR) is increasingly used clinically as an adjunct to fetal echocardiography4, and can non-invasively and quantitatively measure vessel blood flow with velocity-encoded cine PC sequences4. With PC imaging, the MRI signal is used to visualize and quantify blood velocity using phase information. The acquisition of diagnostic-quality images relies on the selection of the correct imaging plane perpendicular to the flow and selection of the encoding velocity to balance aliasing and signal-to-noise ratio (SNR)5. Recently, low field MRI is increasing in popularity due to the availability of wide-bore clinical scanners. Certain properties of low field strengths are ideal for fetal MRI,67 such as shorter T1 and longer T2 times, as well as a more homogeneous B0 field. The wider bore also makes it possible to scan obese individuals, which typically have poor quality prenatal ultrasound scans8. However, the reduced gradient strength and the decreased SNR requires careful optimization of advanced imaging protocols. Structural FCMR has been shown to be possible at low field strengths,91011 but evidence and protocols for quantitative fetal cardiac blood flow measurements at low field strength are lacking. Here, we investigate the ability to use low field (0.55T) MRI to perform fetal blood flow measurements using retrospectively gated PC sequences12.Methods
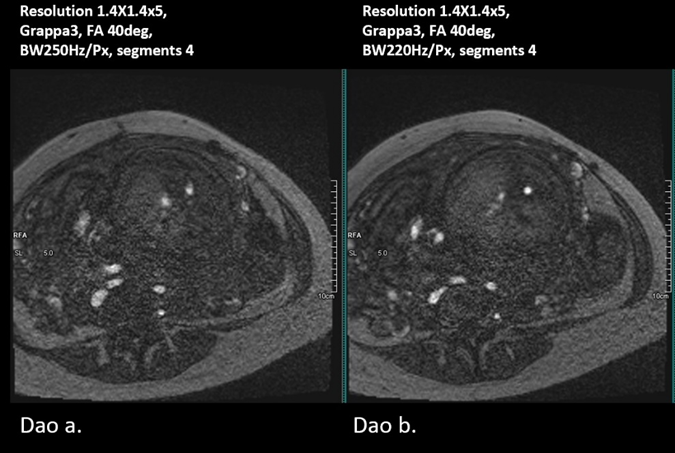
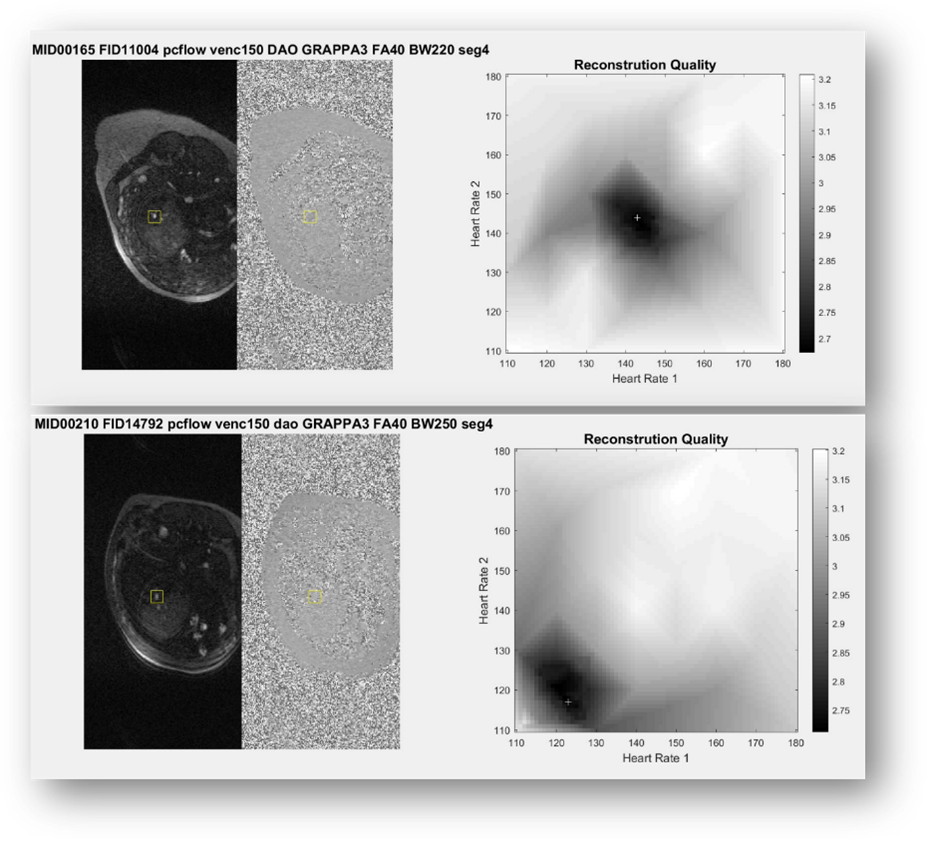
Fetal MRI was acquired as part of two ethically approved prospective single-centre studies (REC 21/LO/0742, REC 22/YH/0210) performed at St Thomas’ Hospital in London, UK on a clinical 0.55T scanner (MAGNETOM Free.Max, Siemens Healthcare, Germany) using a 6-element blanket coil and a 9-element spine coil between September-November 2023. Volunteers were scanned with continuous monitoring of heart rate and blood pressure, in the head-first position with frequent verbal interaction. Balanced steady state free precession (bSSFP) sequences were acquired in three orthogonal planes for planning with TR=729ms, TE=4.21ms, flip angle (FA)=120°, Resolution=0.8x0.8x4.0mm³, Grappa=2, Bandwidth (BW)=252Hz/Px. Initial 2D PC sequence parameters were taken from the existing 1.5T sequence2 with the following parameters: TR 51.4ms, TE=4.00ms, Averages=1, FA=20°, BW=449 Hz/Px, Segments=4, Resolution=1.3x1.3x5.0mm³, No in-plane acceleration. In order to optimize the PC sequence, the following parameters were varied and analysed: FA (20-40°), BW (220-250Hz/Px), resolution (0.6x0.6x8/1.4X1.4x5), GRAPPA (2-4), phase oversampling (50-100%), segments (3-4) with the goal of a scan time less than 40 seconds in order to limit the impact of fetal motion. Three vessels were imaged, and the velocity encoding was set according to the vessel: Umbilical Vein (UV, encoding velocity (venc): 50cm/s), Descending Aorta (DAo, venc: 150cm/s), and Superior Vena Cava (SVC, venc: 100cm/s). Each acquired sequence underwent a visual assessment for motion13, and any scans deemed to have too much motion were discarded. PC sequences were retrospectively gated (Fig.1) using metric optimized gating14.Results
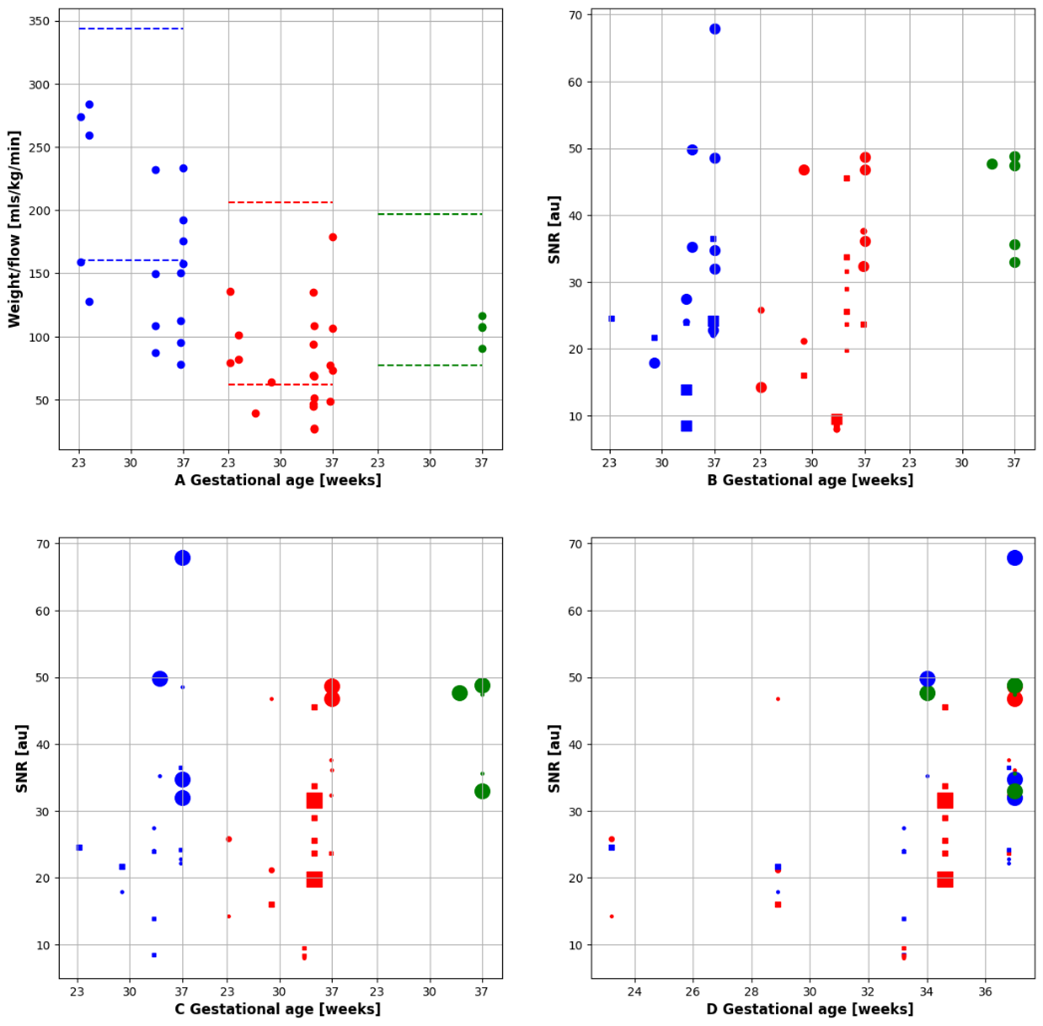
9 pregnant participants were scanned (23+3-37+0 weeks gestational age, GA) resulting in a total of 61 acquired 2D PC sequences. 47 were of sufficient quality to continue with the flow analysis (Fig.1). The initial parameters resulted in a scan time of 2 minutes and showed visible motion artefacts. In total, 61 2DPC sequences were acquired across the 9 subjects. After the visual assessment was performed, 47 were of sufficient quality to continue with the flow analysis (Fig.1). Signal-to-noise ratios (SNR) were calculated 15 and compared across the varying scan parameters, by comparing the mean signal of the vessel of interest and the standard deviation of the background using 3D Slicer16. Quantitative flow measurements and SNR calculations and visual assessment were used to determine optimal PC sequence parameters. (Fig.2) Quantitative flow measurements were made using cvi42 V5.11 (Circle Cardiovascular Imaging Inc. Calgary, Canada). (Fig.3-4) Optimal parameters were determined to be resolution=1.4X1.4x5mm³, FA=40°, BW=220Hz/Px, GRAPPA=3, segments=4.Discussion and conclusion
It is possible to measure fetal cardiac flow in the UV, DAo, and SVC at low field strengths and calculate values within the expected range. As at higher fields, the main limitation is fetal motion. By using metric optimized gating, we were able to account for the fetal heart movement, but not for gross fetal movement, resulting in our high rate of scan exclusion. Future work includes using a doppler ultrasound device for real-time gating rather than gating retrospectively, and testing the reproducibility and repeatability of flow at low field strengths.Acknowledgements
The authors thank all the participating families as well as the midwives and radiographers involved in this study. This work was supported by the NIH (Human Placenta Project—grant 1U01HD087202‐01), Wellcome Trust Sir Henry Wellcome Fellowship (201374/Z/16/Z and /B), UKRI FLF (MR/T018119/1), DFG Heisenberg funding [502024488], EPSRC (EP/V034537/1), the NIHR Clinical Research Facility (CRF) at Guy's and St Thomas' and by core funding from the Wellcome/EPSRC Centre for Medical Engineering [WT203148/Z/16/Z] and by the National Institute for Health Research (NIHR) Clinical Research Facility based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London. The views expressed are those of the authors and not necessarily those of the NHS or the NIHR or the Department of Health and Social Care.References
1. Wu, W., He, J. & Shao, X. Incidence and mortality trend of congenital heart disease at the global, regional, and national level, 1990–2017. Medicine (Baltimore) 99, e20593 (2020).
2. Roberts, T. A. et al. Fetal whole heart blood flow imaging using 4D cine MRI. Nat. Commun. 11, 4992 (2020).
3. Moerdijk, A. S. et al. Fetal MRI of the heart and brain in congenital heart disease. Lancet Child Adolesc. Health 7, 59–68 (2023).
4. Sun, L. et al. Update on fetal cardiovascular magnetic resonance and utility in congenital heart disease. J. Congenit. Cardiol. 5, 4 (2021).
5. Wymer, D. T., Patel, K. P., Burke, W. F. & Bhatia, V. K. Phase-Contrast MRI: Physics, Techniques, and Clinical Applications. RadioGraphics 40, 122–140 (2020).
6. Aviles Verdera, J. et al. Reliability and Feasibility of Low-Field-Strength Fetal MRI at 0.55 T during Pregnancy. Radiology 309, e223050 (2023).
7. Ponrartana, S. et al. Low-field 0.55 T MRI evaluation of the fetus. Pediatr. Radiol. 53, 1469–1475 (2023).
8. Paladini, D. Sonography in obese and overweight pregnant women: clinical, medicolegal and technical issues. Ultrasound Obstet. Gynecol. 33, 720–729 (2009).
9. Datta Singh Goolaub et al. Multireslution comparison of fetal CINE MRI at 0.55T. in (2023).
10. Ye Tian et al. Real-time fetal cardiac MRI at 0.55T enables assessment of ventricular function and heart great vessel anatomy. in (2023).
11. Joshua F.P van Amerom et al. Fetal cardiac 3D cine MRI at low field - whole heart slice to volume reconstruction from real-time SSFP at 0.55T. in (2023).
12. Roy, C. W., van Amerom, J. F. P., Marini, D., Seed, M. & Macgowan, C. K. Fetal Cardiac MRI: A Review of Technical Advancements. Top. Magn. Reson. Imaging TMRI 28, 235–244 (2019).
13. Schulz, A. et al. Structured analysis of the impact of fetal motion on phase-contrast MRI flow measurements with metric optimized gating. Sci. Rep. 12, 5395 (2022).
14. Jansz, M. S. et al. Metric optimized gating for fetal cardiac MRI. Magn. Reson. Med. 64, 1304–1314 (2010).
15. Kathleen E. Colford et al. Exploring the effect of elevated maternal BMI on image quality in fetal MRI. in (2023).
16. Fedorov, A. et al. 3D Slicer as an Image Computing Platform for the Quantitative Imaging Network. Magn. Reson. Imaging 30, 1323–1341 (2012).
Figures