3403
Optimization of bSSFP pulse sequence parameters for low-field fetal cardiac MRI at 0.55T1Centre for the Developing Brain, School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2Biomedical Engineering Department, School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 3Department of Congenital Heart Disease, Evelina Children's Hospital, London, United Kingdom, 4Department of Women & Children's Health, King's College London, London, United Kingdom, 5Smart Imaging Lab, Radiological Institute, University Hospital Erlangen, Erlangen, Germany
Synopsis
Keywords: Fetal, Low-Field MRI, Fetal Cardiac MRI
Motivation: Low field MRI at 0.55T offers advantages such as increased field homogeneities for fetal cardiac MRI and early diagnosis of congenital heart diseases (CHDs) but required careful optimization specific to the properties of low field.
Goal(s): This study aimed to optimize the bSSFP sequence parameters at 0.55T to compensate for the reduced SNR and improve diagnostic capabilities in fetal cardiac MRI.
Approach: Phantom experiments and in-utero studies were conducted to evaluate the impact of optimized parameters of bSSFP sequences on SNR, image quality, and clinical applicability.
Results: The optimized bSSFP sequence parameters demonstrate increased SNR and good visualization of cardiac structures.
Impact: The optimized bSSFP sequence at 0.55T has the potential to be used at low field strengths to prenatally diagnose congenital heart disease, thereby increasing accessibility for patients.
Introduction
Congenital Heart Disease (CHD) is a leading cause of infant morbidity and mortality1, but early and accurate diagnosis provide opportunities for prenatal planning, and treatment after birth, improving postnatal outcomes2. Fetal cardiac magnetic resonance imaging (MRI) is a useful tool for diagnosing CHD at conventional field strengths (1.5T, 3.0T)3,4. New clinical low-field (0.55T) MRI systems offer unique advantages for fetal imaging5,6, such as shorter T1 and longer T2* times, enhancing blood-myocardium contrast, and a larger bore (80 cm), widening access for claustrophobic and obese patients. The lower specific absorption rates (SAR) allow for higher flip angles (FA) to be used while maintaining safe levels in balanced steady-state free precession (bSSFP) pulse sequences. Additionally, the longer T2* and reduced distortion due to susceptibility differences allow for lower bandwidths (BW) settings. However, the decrease in signal-to-noise ratio (SNR) and the reduced gradient performance remains challenging at low field strengths. Previous studies demonstrated the feasibility of fetal cardiac imaging using bSSFP sequences at 0.55T7-9, but SNR calculations and a quantitative diagnostic assessment remains unexplored. Therefore, we aim to optimize the bSSFP sequence parameters at 0.55T to compensate for reduced SNR compared to 1.5T and evaluate its diagnostic quality for fetal cardiac imaging.Methods
All non-gated bSSFP scans were performed using a clinical 0.55T (MAGNETOM Free.Max) and 1.5T scanner (MAGNETOM Sola).Phantom experiments: Standard 1.5T clinical bSSFP scanning parameters10 (TR/TE=569/3.11 ms, BW=514 Hz/Px, FA=88°, FOV=350x350 mm2, resolution=0.7x0.7x5.0 mm3) were used at 1.5T and 0.55T to measure SNR using a doped water-filled cylindrical phantom. At 0.55T, different BWs (250-550 Hz/Px) and FAs (60-150°) were tested across different in-plane resolutions (0.7-1.25 mm2) and slice thicknesses (3.5-5.0 mm).
In-utero study: 14 pregnant women (gestational ages (GA): 18-38 weeks, all controls) were scanned at 0.55T with continuous life monitoring in the head-first supine position after providing written consent to an ethically approved study (REC 21/LO/0742). Coronal bSSFP stacks were acquired in 4/14 cases for parameter optimization. Optimized parameters (TR=670-729 ms, TE=4.21 ms, BW=250 Hz/Px, FA=120°, resolution=0.7x0.7x4.5 mm3) were used to acquire stacks in all three planes for the remaining 10 cases.
SNR calculations: SNR, defined as the mean signal in a region of interest (ROI) divided by the standard deviation of a background region11 was calculated using a 500 mm3 ROI in the phantom and 5 different ROIs (brain white matter, lung, heart, placenta, amniotic fluid) in the in-utero images.
Image quality assessment: Two experienced fetal cardiologists performed a clinical assessment for 10 cases. Images were scored based on the visibility of different cardiac structures12. For each structure, a score of 0 (not visible) to 3 (excellent visibility) was assigned.
Results
Phantom Experiments: An expected 2.5-fold SNR difference was measured between 1.5T and 0.55T at all resolutions and slice thicknesses (Figure 1). The SNR fluctuates slightly as FA increases and peaks at 120°. SNR increased at lower BW of 250 Hz/Px over all FAs and slice thicknesses (Figure 1), with a 1.6-fold SNR increase observed using the optimized parameters (TR/TE=670/4.21ms, BW: 250 Hz/Px, FA: 120°).In-utero study: The optimized sequence parameters qualitatively demonstrate improved contrast (Figure 2), and SNR measurements show how different ROIs were affected (Figure 3). SNR increased by a factor of 1.8 across 4 cases where images were acquired with both original and optimized parameters, compensating for 70% of the SNR loss from 1.5 to 0.55T.
Image quality assessment: Of the ten cases, three were excluded: one due to an early gestational age (18 weeks, too small to visualize structures), and two due to significant motion (GA: 30 and 38 weeks). Across seven cases, 9/12 structures were fully identified by both readers more than 50% of the time (Table 1, Figure 4), even for younger fetuses (GA: 25 weeks). Only three structures (LVOT, RVOT, Aortic Arch) were identified less than 50% of the time.
Discussion and Conclusion
Our results suggest that optimizing the bSSFP sequence parameters at 0.55T, primarily the bandwidth, can partially compensate for the reduced SNR and improve diagnostic quality for fetal cardiac MRI, with parameter optimization compensating for 70% of the overall SNR loss when moving from 1.5 to 0.55T. The in-utero experiments suggest good visualization of fetal cardiac structures with the optimized parameters, demonstrating its potential as a diagnostic tool for CHD. Future work could explore motion correction, real-time imaging, and scanning fetuses with CHD at 0.55T. The optimized bSSFP sequences at 0.55T demonstrate the potential for accurate diagnosis of CHD at low field strengths.Acknowledgements
The authors thank all the participating families as well as the midwives and radiographers involved in this study. This work was supported by the NIH (Human Placenta Project—grant 1U01HD087202‐01), Wellcome Trust Sir Henry Wellcome Fellowship (201374/Z/16/Z and /B), UKRI FLF (MR/T018119/1), DFG Heisenberg funding [502024488], EPSRC (EP/V034537/1), the NIHR Clinical Research Facility (CRF) at Guy's and St Thomas' and by core funding from the Wellcome/EPSRC Centre for Medical Engineering [WT203148/Z/16/Z] and by the National Institute for Health Research (NIHR) Clinical Research Facility based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London. The views expressed are those of the authors and not necessarily those of the NHS or the NIHR or the Department of Health and Social Care.
References
1. Collaborators, G. B. D. C. H. D. Global, regional, and national burden of congenital heart disease, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Child Adolesc Health 4, 185-200 (2020). https://doi.org:10.1016/S2352-4642(19)30402-X
2. Hunter, L. E. & Simpson, J. M. Prenatal screening for structural congenital heart disease. Nat Rev Cardiol 11, 323-334 (2014). https://doi.org:10.1038/nrcardio.2014.34
3. Roy, C. W., van Amerom, J. F. P., Marini, D., Seed, M. & Macgowan, C. K. Fetal Cardiac MRI: A Review of Technical Advancements. Top Magn Reson Imaging 28, 235-244 (2019). https://doi.org:10.1097/RMR.0000000000000218
4. Marini, D., van Amerom, J., Saini, B. S., Sun, L. & Seed, M. MR imaging of the fetal heart. J Magn Reson Imaging 51, 1030-1044 (2020). https://doi.org:10.1002/jmri.26815
5. Arnold, T. C., Freeman, C. W., Litt, B. & Stein, J. M. Low-field MRI: Clinical promise and challenges. J Magn Reson Imaging 57, 25-44 (2023). https://doi.org:10.1002/jmri.28408
6. Aviles Verdera, J. et al. Reliability and Feasibility of Low-Field-Strength Fetal MRI at 0.55 T during Pregnancy. Radiology 309, e223050 (2023). https://doi.org:10.1148/radiol.223050
7. Ponrartana, S. et al. Low-field 0.55 T MRI evaluation of the fetus. Pediatr Radiol 53, 1469-1475 (2023). https://doi.org:10.1007/s00247-023-05604-x
8. Ye Tian, J. D., Jay D. Pruetz, Anand A. Joshi, John Wood, Krishna S. Nayak. Real-time fetal cardiac MRI at 0.55T enables assessment of ventricular function and heart and great vessal anatomy. ISMRM (2023).
9. Joshua F P van Amerom, Y. T., Datta S Goolaub, John Wood, Jon Detterich, Krishna S Nayak, Christopher K Macgowan. Fetal cardiac 3D cine MRI at low field - whole heart slice-to-volume reconstruction from real-time spiral SSFP at 0.55T. ISMRM (2023).
10. Lloyd, D. F. et al. An exploration of the potential utility of fetal cardiovascular MRI as an adjunct to fetal echocardiography. Prenat Diagn 36, 916-925 (2016). https://doi.org:10.1002/pd.4912
11. Kathleen Elizabeth Colford, D. C., Zoe Hesketh, Tom Finck, Ayse Ceren-Tanritanir, Serena Counsell, Mary Rutherford. Exploring the effect of elevated maternal BMI on image quality in fetal MRI. ISMRM (2023).
12. Geiger, J. et al. Feasibility of Non-Gated Dynamic Fetal Cardiac MRI for Identification of Fetal Cardiovascular Anatomy. Fetal Diagn Ther 50, 8-16 (2023). https://doi.org:10.1159/000528966
Figures
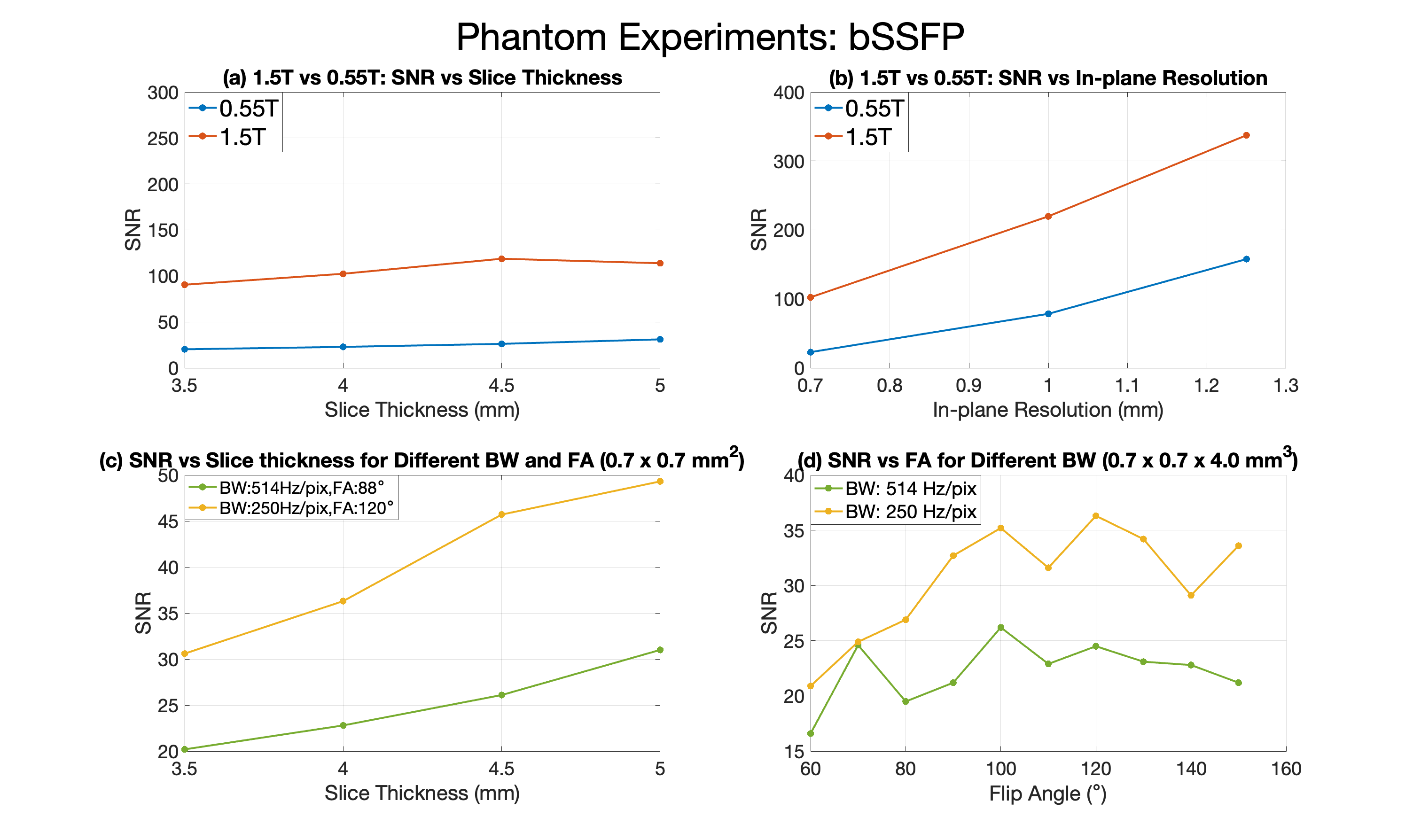
Figure 1: Phantom experiment: bSSFP SNR comparison between 1.5T and 0.55T, and SNR optimization at 0.55T. (a) SNR vs slice thickness and (b) SNR vs in-plane resolution. (c) SNR vs slice thickness for different bandwidth and flip angle, with in-plane resolution of 0.7 x 0.7 mm2. (d) SNR vs flip angle for different bandwidths with resolution of 0.7 x 0.7 x 4.0 mm3. Overall, lower bandwidth at 250 Hz/Px and higher flip angle at 120° resulted in a 1.6-fold SNR increase.
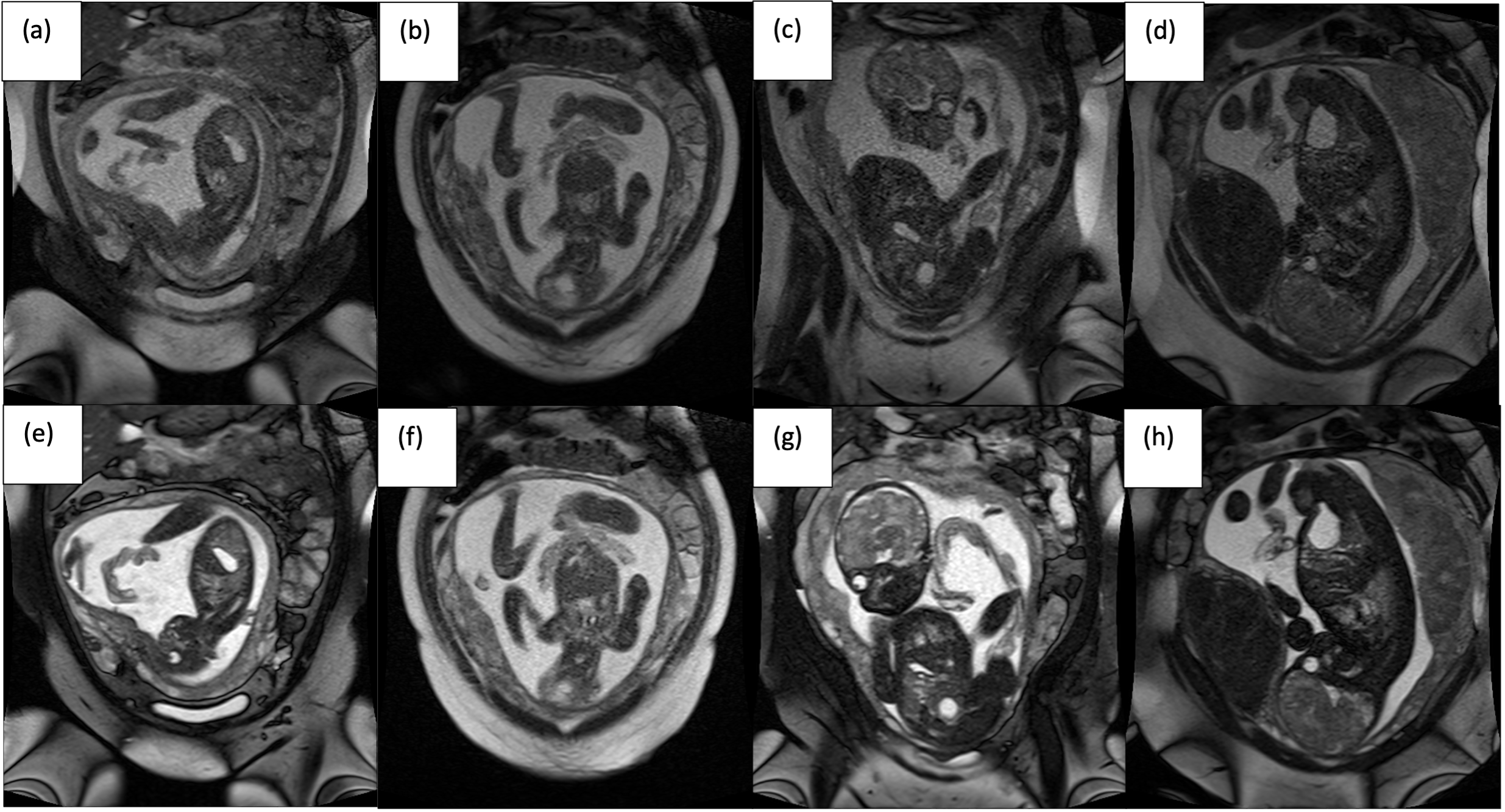
Figure 2: bSSFP fetal images acquired at 0.55T with original 1.5T parameters (top row) and optimized parameters at 0.55T (bottom row). Original parameters: bandwidth: 514 Hz/pix, flip angle: 88°. Optimized parameters: Bandwidth: 250 Hz/pix, flip angle: 120°. All images had in-plane resolution of 0.7 x 0.7 mm. (a,e) GA: 25, (b,f) GA: 25, (c,g) GA: 30, (d,h) GA: 36. Note the improved SNR, and improved contrast between amniotic fluid and fetal structures.
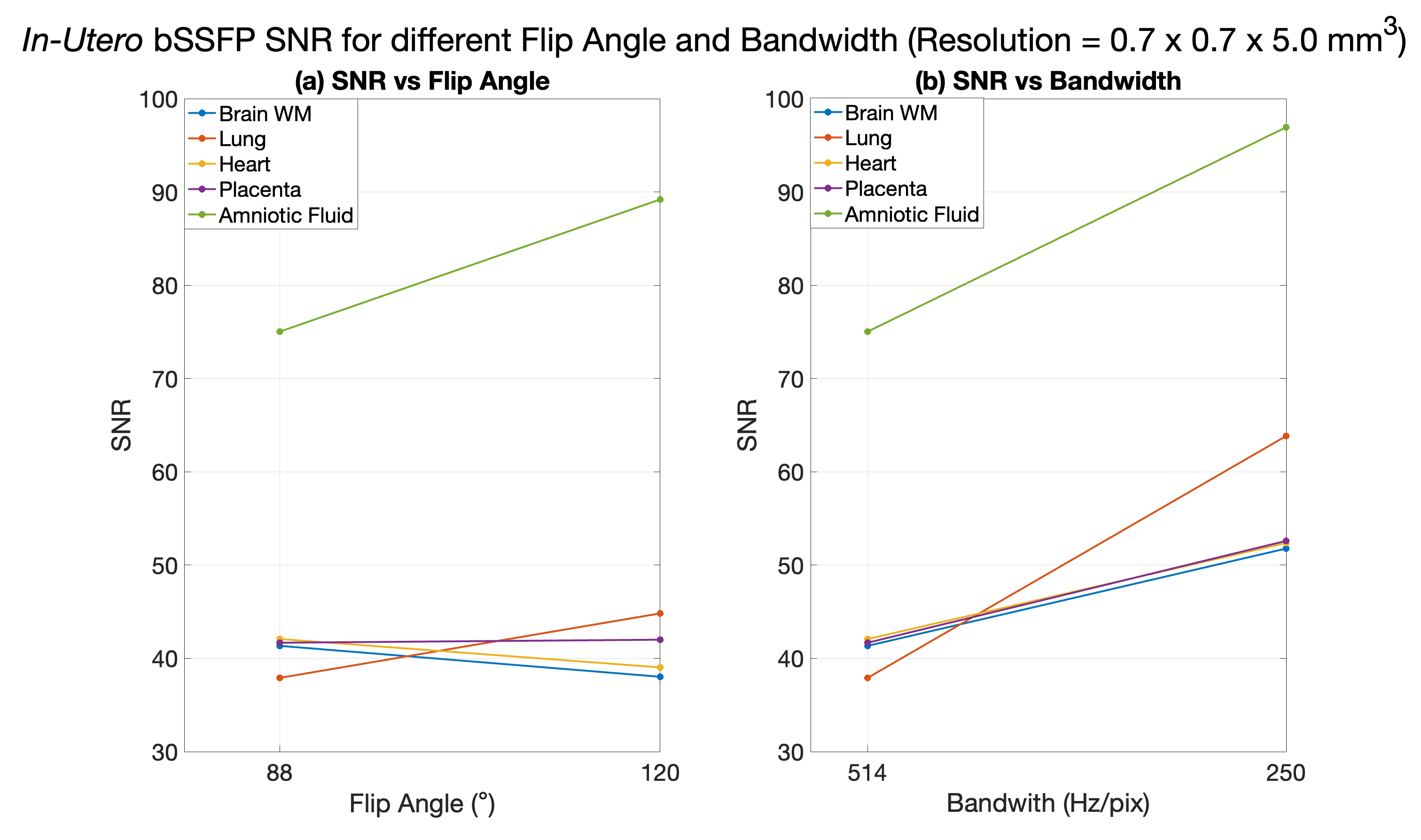
Figure 3: Example of in-utero SNR measurements: optimized parameters vs original parameters used on 1.5T. (a) SNR vs flip angle. (b) SNR vs bandwidth. The SNR of the lung and the amniotic fluid are most impacted by the flip angle.
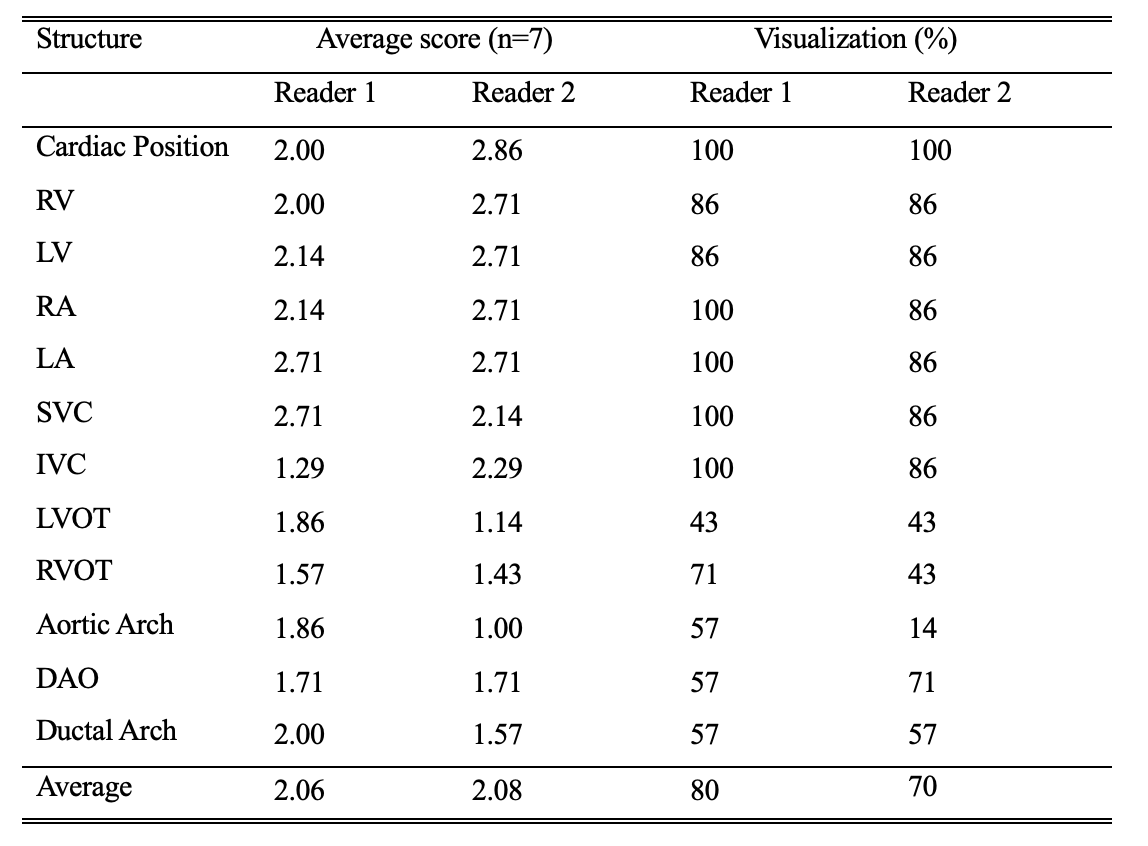
Table 1: Fetal cardiovascular structures and visualization assessment for seven cases with bSSFP sequences in three orientations with the optimized parameters (bandwidth = 250 Hz/Px, flip angle = 120°, resolution = 0.7 x 0.7 x 4.5 mm3). For each structure, a score of 0 (not visible) to 3 (excellent visibility) was assigned. A score of 0 and 1 were regarded as not visible, and scores of 2 and 3 were regarded as visible. Overall image quality was good with average scores of 2.06 and 2.08, visualization percentage was also comparable for the two readers.
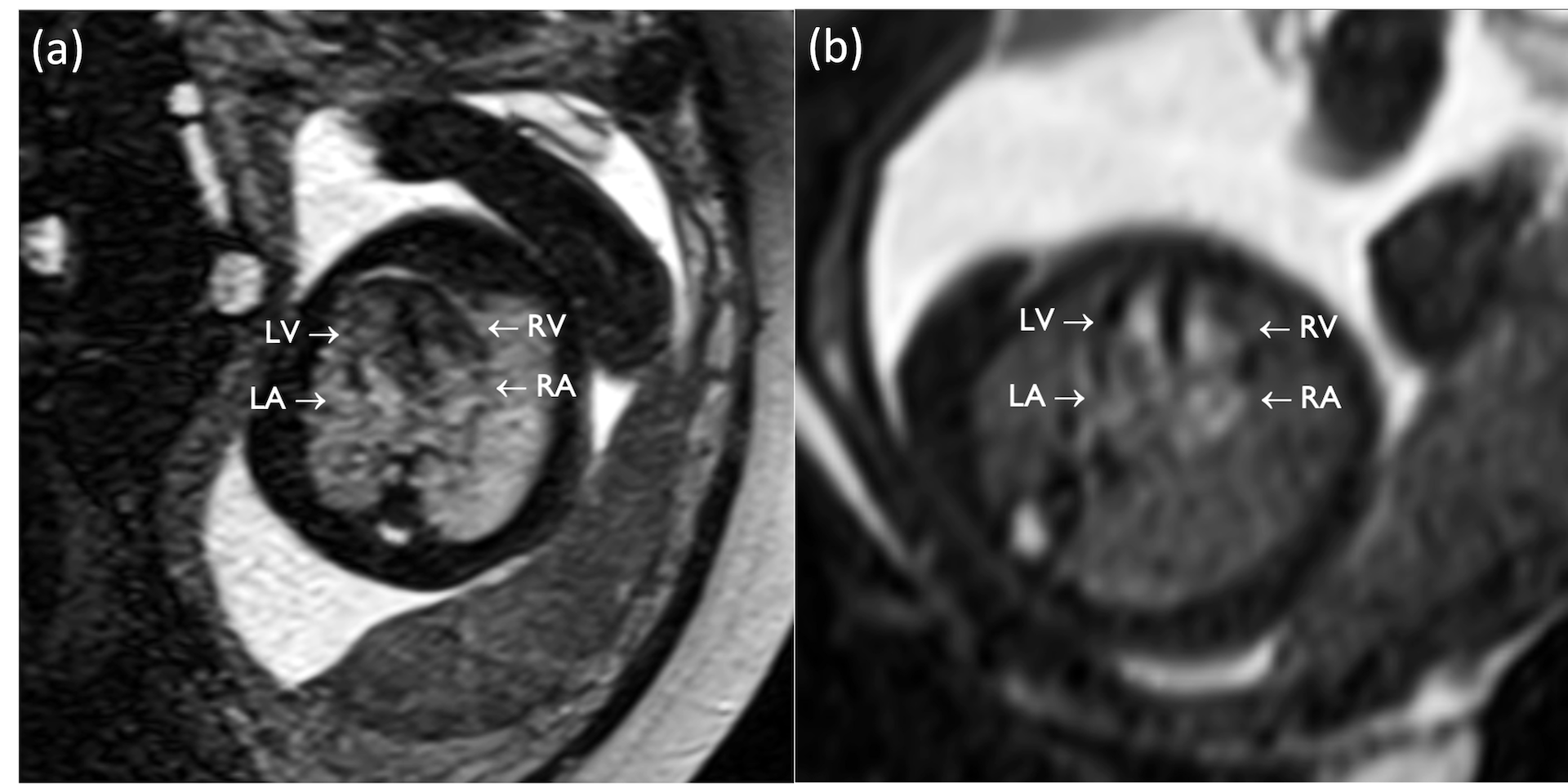
Figure 4: bSSFP images of the fetal heart showing equivalent to a four-chamber view (axial plane), with full visualization of the four chambers (LV, RV, LA, RA). (a). GA: 36 weeks. (b). GA: 24 weeks.