3402
Evaluation of Wideband Cardiac, Real-Time Pulse Sequences in Children with a Cardiac Implantable Electronic Device1Biomedical Engineering/Radiology Department, Northwestern University, Chicago, IL, United States, 2Division of Cardiology, Department of Pediatrics, Ann & Robert H. Lurie Children’s Hospital, Chicago, IL, United States, 3Department of Medical Imaging, Ann & Robert H. Lurie Children’s Hospital, Chicago, IL, United States
Synopsis
Keywords: Cardiovascular, Pediatric, Cardiac Implantable Electronic Devices, Real-Time Cine, Wideband, Pulse Sequence, Perfusion, LGE
Motivation: Cardiac MRI is rarely performed in children with cardiac implantable electronic devices (CIED) due to safety concerns and image artifacts.
Goal(s): To determine the clinical utility of wideband cardiac, real-time MRI methods in children with an implantable pulse generator (IPG).
Approach: We performed free-breathing real-time cine, wideband late gadolinium enhancement (LGE) and perfusion in 18 healthy children with IPG taped to below the left clavicle and abdomen to mimic endocardial and epicardial systems, respectively.
Results: Compared to the standard, wideband sequences effectively suppressed image artifacts, and produced relatively accurate quantification of bi-ventricular functional metrics.
Impact: Wideband cardiac, real-time pulse sequences are effective in reducing image artifacts induced by an IPG, thereby increasing the potential benefit of cardiac MRI in children with CIEDs.
Introduction
Children with serious conduction disease such as congenital complete atrioventricular block or symptomatic sinus node dysfunction require a cardiac implantable electronic device (CIED). Cardiac MRI in children with CIED are rarely performed due to safety concerns1 and significant image artifacts caused by an implantable pulse generator (IPG).2 In this study, we sought to determine the diagnostic utility of free-breathing real-time cine (FB-RT)3, wideband late gadolinium enhancement (LGE),4 and wideband perfusion5 pulse sequences in children with an IPG taped to anatomically correct locations to mimic endocardial and epicardial CIED systems, respectively, where standard cardiac pulse sequences with no IPG were used as reference.Methods
Healthy children > age 10, not requiring anesthesia, were recruited for a research MRI with no sedation or contrast agent. Imaging was performed with no IPG as reference, then repeated with a defibrillator IPG (Evera, Medtronic, USA) taped below the left clavicle and on the abdomen by a trained physician to mimic endocardial and epicardial CIED, respectively. Cardiac MRI was performed on a 1.5 T MRI scanner (Aera, Siemens). All pulse sequences used spoiled gradient-recalled echo (GRE) readout.Pulse Sequences: (Cine) We performed 32-fold, accelerated FB-RT cine image acquisition and reconstruction, as previously described,3 and standard breath-hold (BH) cine MRI. (Perfusion) We performed 5.8-fold accelerated wideband perfusion image acquisition and reconstruction, as previously described,5 and standard perfusion MRI. Proton density (PD) and T1-weighted (T1w) images were acquired to calculate the normalized signal that corrects for coil profiles and equilibrium magnetization.6 (LGE) We performed standard and wideband LGE with phase-sensitive inversion recovery (PSIR) reconstruction,7 which corrects for the surface coil effects. Table 1 summarizes the image acquisition parameters for cine, LGE and perfusion sequences.
Image Analysis:
(Cine) Cardiac contours were drawn in the left ventricle (LV) and right ventricle (RV) using the automatic AI tools followed by manual correction in Circle (cvi42, v5.14.2). We recorded the quantitative results of cardiac function: EDV, ESV, SV, and EF for the LV and RV, respectively. To quantify image artifacts in the FB-RT cine images, we selected three SAX planes (base, mid, apex) and manually segmented the LV myocardium at the end-diastolic phase with in-house tools written in MATLAB. We divided the myocardium into 16 AHA segments and obtained the coefficient of variation in the segments with FB-RT cine without IPG as reference. (Perfusion) We manually segmented the whole LV (since there is no contrast between blood and myocardium) in three SAX planes and calculated the normalized SI (i.e., T1w/PD). Standard perfusion with no IPG was used as reference. (LGE) In each of 16 segments, we calculated the mean signal intensity (SI) of the PSIR images. For reference LGE, we averaged SI from standard and wideband without IPG to account for the difference in inversion time (Table 1).
Statistical Analysis: One-way repeated measures ANOVA with Bonferroni correction was used to compare the cardiac functional metrics. For image artifact comparison, each myocardial segment SI was determined whether it is within mean ± 1.96 standard deviation of the reference.
Results
CMR studies were performed on N=18 children, median age 13 years (range 11-16) with 6 males and 12 females. (Cine) There were significant image artifacts in 8 out of 16 and 1 out of 16 LV segments with the IPG in clavicular and abdominal position, respectively (N=18, Figure 1). Despite image artifacts, there was no statistically significant difference (p > 0.68) in the cardiac functional parameters in cine with and without IPG for both the LV and RV (N=10, Table 2). (Perfusion) Only the standard sequence with IPG in the clavicle and abdomen (apex) were significantly different while the wideband sequence was not different from the reference (N=18, Figure 2). (LGE) Standard LGE produced significant image artifacts across 14 out of 16 segments with IPG in the clavicular position and 9 out of 16 segments with IPG in the abdominal position. Wideband LGE effectively suppressed image artifacts across all segments, except for one segment with IPG in the clavicular position (N=16, Figure 3).Conclusion
This study demonstrates that wideband LGE and perfusion pulse sequences are effective in suppressing image artifacts induced by an IPG in both clavicular and abdominal positions in children, whereas standard sequences produced significantly more image artifacts induced by the IPG. Also, while there were artifacts in the FB-RT cine images, the IPG did not significantly affect bi-ventricular functional measurements.Acknowledgements
The authors would like to thank funding support from the National Institutes of Health (R01HL116895, R01HL151079, R21EB030806A1, 1R01HL167148‐01A1), the American Heart Association (19IPLOI34760317, 949899), the Radiological Society of North America (EILTC2302), and the Brett Boyer Foundation.
References
1. Silka MJ, Shah MJ, Silva JNA, et al. 2021 PACES Expert Consensus Statement on the Indications and Management of Cardiovascular Implantable Electronic Devices in Pediatric Patients: Executive Summary. Heart Rhythm. Nov 2021;18(11):1925-1950. doi:10.1016/j.hrthm.2021.07.051
2. Sasaki T, Hansford R, Zviman MM, et al. Quantitative assessment of artifacts on cardiac magnetic resonance imaging of patients with pacemakers and implantable cardioverter-defibrillators. Circ Cardiovasc Imaging. Nov 2011;4(6):662-70. doi:10.1161/circimaging.111.965764
3. Hong. K, Fan. L, Collins. JD, Patel. AR, Lee. DC, Kim. D. Highly-accelerated Real-time Cine MRI with Radial k-space Sampling and View Sharing and KWIC Filtering in Patients with a Cardiac Implantable Electronic Device. Program Number 1353240. In Proceedings of SCMR 26th Annual Scientific Sessions 2023, San Diego, CA, USA.
4. Ranjan R, McGann CJ, Jeong EK, et al. Wideband late gadolinium enhanced magnetic resonance imaging for imaging myocardial scar without image artefacts induced by implantable cardioverter-defibrillator: a feasibility study at 3 T. Europace. Mar 2015;17(3):483-8. doi:10.1093/europace/euu263
5. Hong K, Collins JD, Freed BH, et al. Accelerated Wideband Myocardial Perfusion Pulse Sequence with Compressed Sensing Reconstruction for Myocardial Blood Flow Quantification in Patients with a Cardiac Implantable Electronic Device. Radiol Cardiothorac Imaging. Apr 16 2020;2(2):e190114. doi:10.1148/ryct.2020190114
6. Cernicanu A, Axel L. Theory-based signal calibration with single-point T1 measurements for first-pass quantitative perfusion MRI studies. Acad Radiol. Jun 2006;13(6):686-93. doi:10.1016/j.acra.2006.02.040
7. Kellman P, Arai AE, McVeigh ER, Aletras AH. Phase-sensitive inversion recovery for detecting myocardial infarction using gadolinium-delayed hyperenhancement. Magn Reson Med. Feb 2002;47(2):372-83. doi:10.1002/mrm.10051
Figures
Table 1: Summary of imaging parameters for standard BH cine, FB-RT cine, standard and wideband perfusion and LGE pulse sequences.
Figure 1: End diastolic phases of three SAX (base, mid, apex slices) of standard BH cine without IPG and FB-RT cine without and with IPG taped on the clavicle and abdomen. Arrows indicate signal loss due to IPG. The average coefficient of variation in the LV myocardial segments are shown in the bullseye plots. Segments with asterisk fall outside the mean ± 1.96 SD of the FB-RT cine without IPG (reference).
Table 2: Comparison of quantitative evaluation of ventricular function between clinical BH cine and FB-RT cine with and without taped IPG.
Figure 2: Three short axis slices of the unenhanced standard and wideband perfusion with and without IPG. Arrow indicates artifact. The normalized mean SI of the LV (myocardium + blood pool) are shown in the bullseye plots. Regions with asterisk fall outside the mean ± 1.96 SD of the standard without IPG.
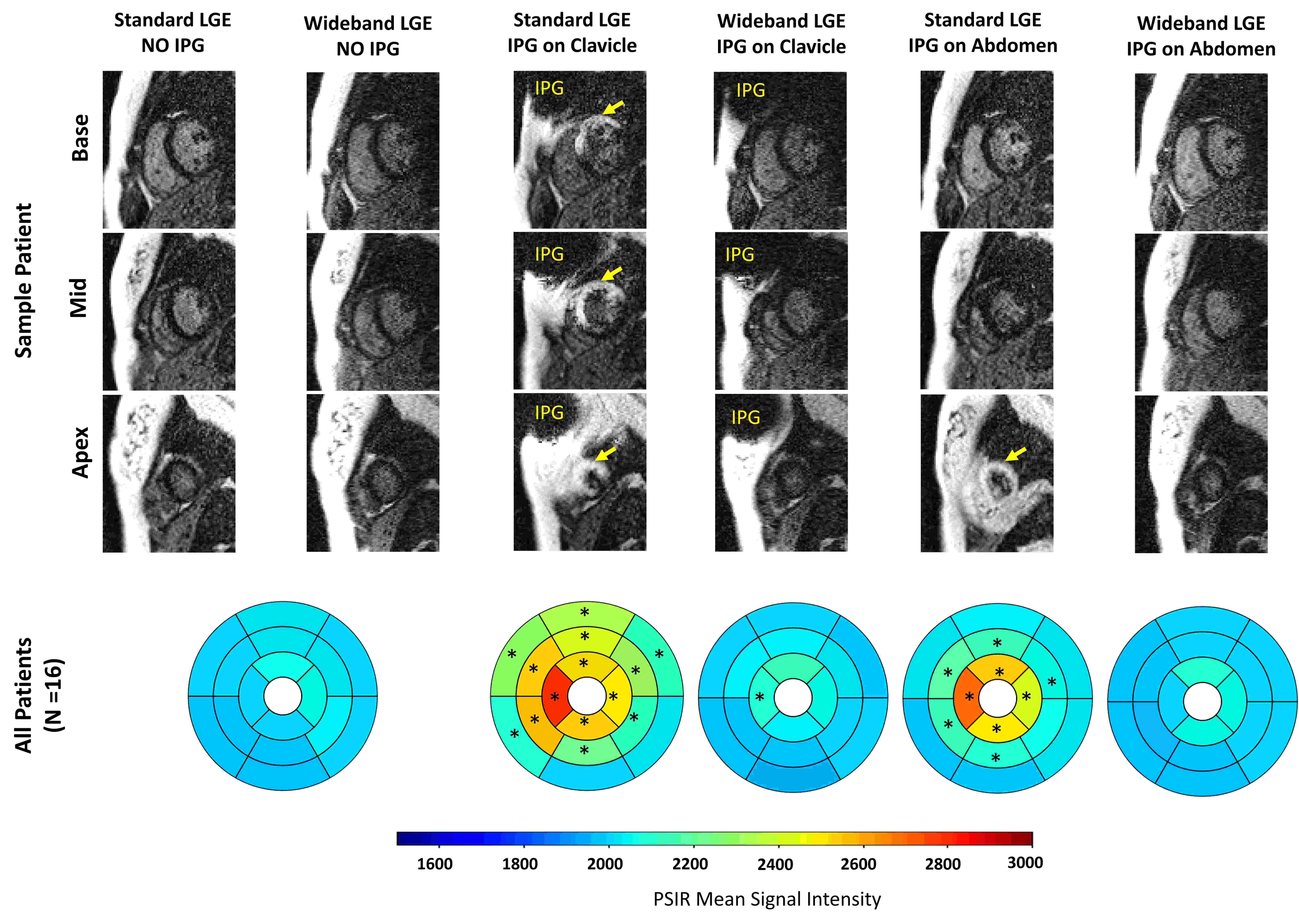
Figure 3: Magnitude images of the three short axis slices of unenhanced standard and wideband LGE with and without IPG. Arrow indicates artifact. The mean SI of the PSIR images is shown in the bullseye plots. Myocardial segments with asterisk fall outside the mean ± 1.96 SD of the average mean SI of the standard and wideband LGE without IPG.