3401
Cardiac MRI markers are associated with adverse clinical outcomes in neonates after congenital diaphragmatic hernia repair1Department of Diagnostic and Interventional Radiology, University Hospital Bonn, 53121, Germany, 2University Hospital Bonn, Bonn, Germany
Synopsis
Keywords: Heart Failure, Cardiovascular
Motivation: The triad of pulmonary hypoplasia, pulmonary hypertension, and early cardiac dysfunction has been postulated to be responsible for poor postnatal outcomes in congenital diaphragmatic hernia repair (CDH).
Goal(s): This study was aimed to investigate whether MRI markers of cardiac dysfunction are associated with clinical outcomes in neonates after CDH.
Approach: In this prospective study neonates after CDH repair underwent 3T cardiac MRI. Biventricular function/volumes, end-diastolic/end-systolic volumes, shunt fraction were assessed. The study cohort was binarized based on median RVEF (cutoff >54%) to compare clinical variables and outcome data between two groups.
Results: MRI-derived parameters of RV-dysfunction were associated with short-term clinical outcomes.
Impact: Cardiac MRI allows for objective and early assessment of cardiac dysfunction and, hence, might play an important role in risk stratification and clinical decision-making in neonates after CDH repair.
Body of the abstract
INTRODUCTIONCongenital diaphragmatic hernia (CDH) is a life-threatening anomaly characterized by diaphragmatic defect, intrathoracic herniation of abdominal viscera and pulmonary hypoplasia. The triad of pulmonary hypoplasia, pulmonary hypertension, and early cardiac dysfunction has been postulated to be responsible for poor postnatal outcomes in CDH1. Therefore, the aim of this observational study is to investigate whether cardiac MRI markers of cardiac dysfunction are associated with clinical outcomes in neonates after CDH repair.
METHODS
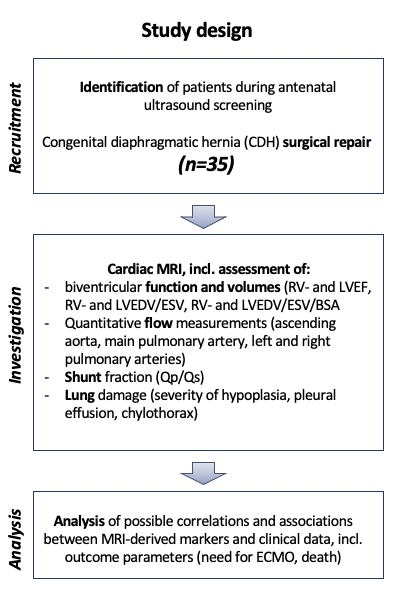
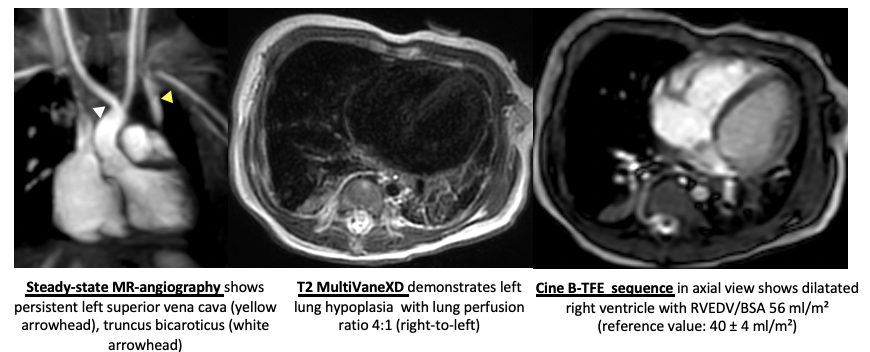
This prospective study was approved by the local institutional review board. In this ongoing prospective study (from June 2020) neonates after CDH repair underwent cardiac MRI in a neonatal ICU-sited and neonatal-sized 3 Tesla MRI scanner in deep sedation. Cardiac MRI protocol included assessment of biventricular function and volumes (left and right ventricular ejection fraction [LVEF, RVEF], end diastolic [EDV] and end systolic [ESV] volumes, shunt fraction [Qp/Qs], and lung perfusion). The study cohort was binarized based on median RVEF (cutoff value >54%) to compare clinical variables and outcome data (need for extracorporeal membrane oxygenation (ECMO) support and death) between the two groups. Measurements were performed separately and/or in consensus by two radiologists. Unpaired t test, Mann-Whitney U test, Spearman correlation coefficient, and a univariable ordinal regression model were used for statistical analysis.
RESULTS
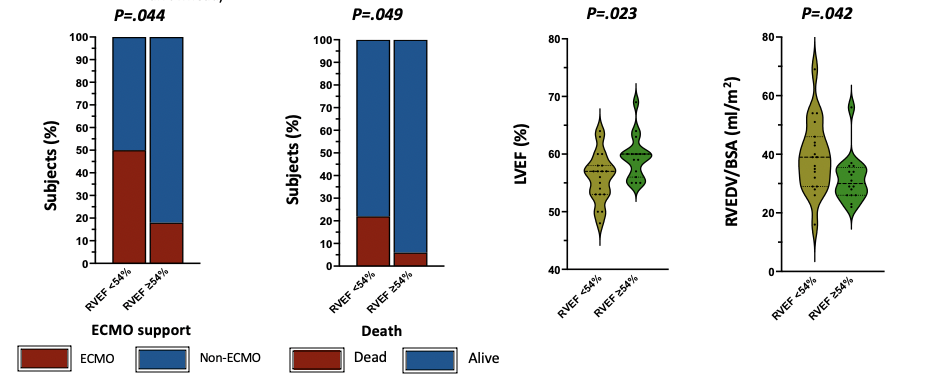
A total of 35 neonates (mean gestational age: 38±2 weeks, 16 female, 29 left-sided CDH, 17 “liver-up”) were evaluated. Baseline anthropometric and clinical characteristics (incl. age, sex, birth weight and height [percentile], time to repair, etc.) were similar in both groups (P>.05). Impaired RVEF correlated with the need for ECMO support after CDH repair (r=0.37, P=0.013). Neonates with lower RVEF (<54%) had worse clinical outcomes (22 vs. 6% mortality, P=0.049; 50 vs. 18% ECMO, P=0.044). Univariable ordinal regression analysis revealed an association between MRI-derived RVEF and the need for ECMO support (odds ratio: 0.87, 95% confidence interval: 0.75-0.98; P=0.019). LVEF was more impaired in the group with RVEF<54% (LVEF: 55±4 vs. 59±4%, P=.023).
DISCUSSION
Despite advances in medical care of neonates with CDH, mortality and morbidity continues to be high. Although many factors play role in the prognosis of CDH, the major determinant of survival is pulmonary hypoplasia and related pulmonary hypertension1,2. Progressive increase in pulmonary hypertension, right ventricular failure and concomitant left ventricular dysfunction are associated with higher mortality in CDH2. Therefore, comprehensive and reliable imaging techniques for the assessment and follow-up of pulmonary hypertension and cardiac dysfunction are crucial for timely therapies to prevent adverse outcomes. Cardiac MRI has experienced a fast evolution and has proven to be a reliable and accurate technique, not only for morphologic visualizations, but also for the assessment of ventricular function, the thoracic vasculature and hemodynamics3. Therefore, in this study, we assessed a cohort of neonates after CDH repair, with similar baseline characteristics including gestational age, sex, birth weight, and other clinical parameters to find out which MRI-derived parameters are associated with adverse clinical outcomes. The main finding of our study was there was a significant correlation between impaired RVEF and the requirement for ECMO support following CDH repair. In fact, neonates with lower RVEF (<54%) experienced more unfavorable clinical outcomes, with higher mortality (22% vs. 6%) and a greater need for ECMO support (50% vs. 18%). In addition, LVEF was also more compromised in the group with RVEF<54% (P=0.023). The results of our study support the clinical importance of comprehensive cardiac MRI in neonates undergoing CDH repair. Impaired RVEF in cardiac MRI appears to be a critical factor in predicting the need for ECMO support and ultimately influencing the clinical outcomes in this patient population.
CONCLUSION
Cardiac MRI allows for accurate and objective assessment of cardiac dysfunction in neonates after CDH repair. MRI-derived parameters of RV dysfunction were associated with short-term clinical outcomes.
Acknowledgements
noneReferences
1.
Boloker J, Bateman DA, Wung JT, Stolar
CJ. Congenital diaphragmatic hernia in 120 infants treated consecutively with
permissive hypercapnea/spontaneous respiration/elective repair. J. Pediatr.
Surg. 2002; 37: 357–66.
2. da-Costa-Santos J, Bennini JR Imaging Assessment of Prognostic Parameters in Cases of Isolated Congenital Diaphragmatic Hernia: Integrative Review Rev Bras Ginecol Obstet 2022;44(4):435–441.
3. Tkach JA, Higano NS, Taylor MD et al. Quantitative cardiopulmonary magnetic resonance imaging in neonatal congenital diaphragmatic hernia Pediatr Radiol. 2022 Nov;52(12):2306-2318
Figures