3397
Prognostic value of late gadolinium enhancement in children with dilated cardiomyopathy1Radiology, West China Second University Hospital, Chengdu, China
Synopsis
Keywords: Cardiovascular, Cardiomyopathy, Dilated cardiomyopathy; late gadolinium enhancement
Motivation: The prognostic value of late gadolinium enhancement (LGE) in adult dilated cardiomyopathy (DCM) has been confirmed, but its prognostic value in children with DCM remains unclear.
Goal(s): To evaluate the prognostic value of late LGE in children with DCM.
Approach: This retrospective single-center study analyzed 76 children with DCM. The composite endpoint was all-cause mortality, heart transplant, and rehospitalization for heart failure. The risk factors for the composite endpoint were identified with multivariable Cox analysis.
Results: Multivariable Cox analysis showed that LGE present was associated with the composite endpoints (hazard ratio [HR], 2.59 [95% CI: 1.05, 6.37], p=0.039).
Impact: Late gadolinium enhancement of CMR in children with DCM provides independently prognostic value of all-cause mortality, heart transplant, and rehospitalization for heart failure.
Introduction
The prognostic value of late gadolinium enhancement (LGE) in adult dilated cardiomyopathy (DCM) has been confirmed. However, the prognostic value of LGE in children with DCM remains to be investigated. This study aims to evaluate the prognostic value of late LGE in children with DCM.Methods
This retrospective single-center study analyzed 76 consecutive children with DCM who underwent cardiac magnetic resonance (CMR) to assess left ventricular dysfunction and myocardial fibrosis between July 2018 and December 2022. The composite endpoint was all-cause mortality, heart transplant, and rehospitalization for heart failure. The risk factors for the composite endpoint were identified with multivariable Cox analysis.Results
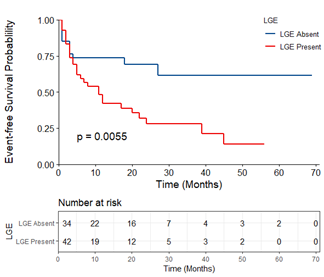
Among the 76 children (mean age, 6.1±4.9 years; 48 male [63.2%]), 42 patients (55.3%) were primary DCM, and 34 (44.7%) were secondary DCM. Forty-two patients (55.3%) had LGE, and 34 did not. During a mean follow-up period of 16.4±16.6 months (range, 1-69 months), a total of 40 patients reached the composite endpoint, in which 20 (50.0%) died of heart failure, 3 (7.5%) underwent a heart transplant, 17 (42.5%) rehospitalized for heart failure. Patients who reached the composite endpoint had a higher Lg-BNP (3.4 pg/mL [3.2, 3.7] vs. 2.6 pg/mL [1.5, 3.5], p=0.004). There is no significant difference among sex, age of diagnosis, body surface area, family history of DCM, and NYHA/Ross class between patients who reached the composite endpoint and those who did not. While, patients who reached the composite endpoint had a higher indexed left ventricular (LV) end-diastolic volume (LVEDVi) (130.8±47.5mL/m2 vs 103.1±33.4 mL/m2, p=0.004), indexed LV end-systolic volume (LVESVi) (110.8mL/m2 [59.4, 131.9] vs. 62.1mL/m2 [44.2, 92.7], p=0.003), indexed LV mass (LVMi) (59.7g/m2 [45.2, 70.1] vs. 49.6g/m2 [39.1, 59.3], p=0.03) and lower LVEF (19.8% [14.5, 29.7] vs. 33.1% [22.9, 47.1]), p=0.002). In univariable Cox regression analyses, Lg-BNP, systolic blood pressure, LVEDVi, LVESVi, LVMi, LVEF, and LGE present were all associated with the primary endpoint (all p<0.05). Multivariable stepwise analysis showed that only LGE present was associated with the composite endpoints (hazard ratio [HR], 2.59 [95% CI: 1.05, 6.37], p=0.039).Conclusions
Myocardial fibrosis assessment by LGE based on CMR can be used to identify children with DCM who are at high risk of all-cause death, heart transplant, and clinical deterioration.Acknowledgements
Not Applicable.References
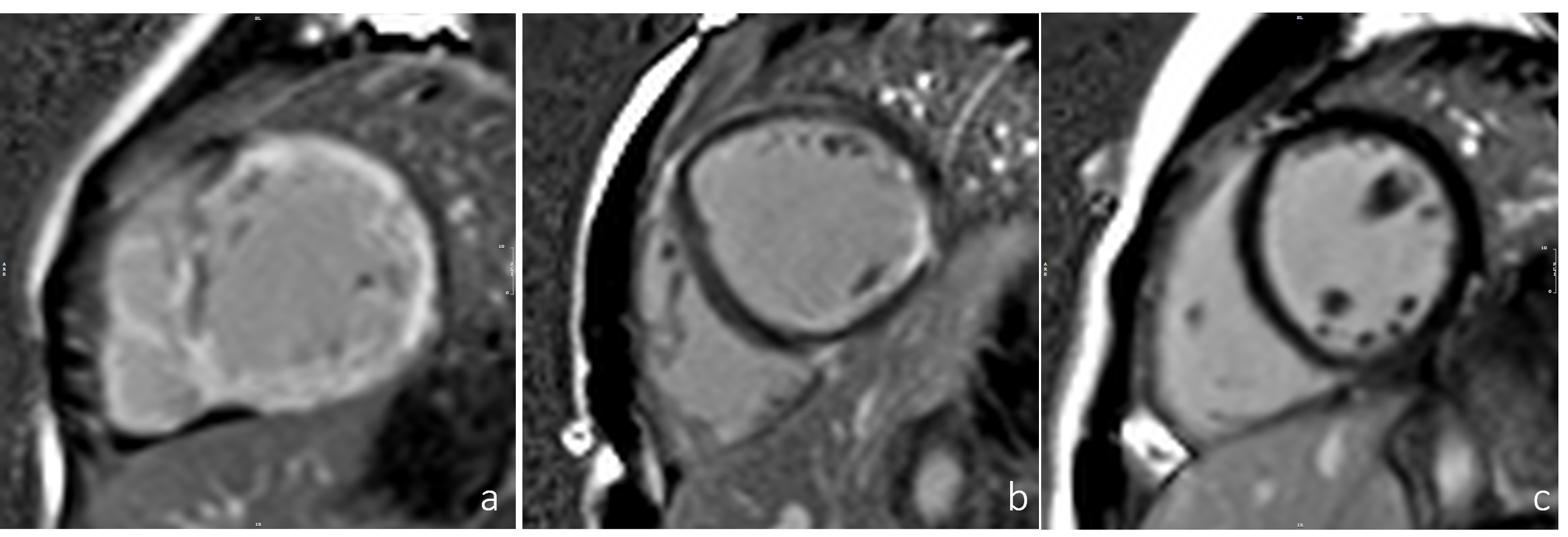
noneFigures