3393
4D Flow Assessment for Reconstruction Right Ventricular Outflow Tract in Congenital Heart Disease Patients: New Hemodynamic Insights1Shanghai Children's Medical Center, Shanghai, China, 2Siemens Healthineers Ltd, Shanghai, China
Synopsis
Keywords: Cardiovascular, Cardiovascular
Motivation: 4D Flow Assessment for Reconstruction Right Ventricular Outflow Tract in Congenital Heart Disease Patients: New Hemodynamic Insights for Handmade Three-Valve Goretex Conduit
Goal(s): 1) evaluate pulmonary valve regurgitation and the patency of the Goretex conduit using 4D flow CMR compare with controls. 2) assess the variation of advanced hemodynamic parameters of 2D axial WSS, 2D circumference WSS and EL in Gortex conduit.
Approach: The CMR data was acquired from 12 healthy participants and 17 patients who were performed cine sequence in routine chamber view and 4D flow.
Results: Hemodynamic changes were detected in patients with right ventricular outflow tract reconstruction.
Impact: Further long-term evaluation is necessary for the changes in segmental WSS in MPA.
Background
Reconstruction of the right ventricular outflow tract is one of the most common surgical strategies for management of congenital heart disease (CHD), accounting for about 50% of complex heart disease surgeries [1]. The handmade three-valve Goretex conduit enables unobstructed connection between the right ventricular outflow tract and the pulmonary artery, and reduces reflux from main the pulmonary artery [2]. However, the non-stretchability material of Goretex conduit needs long-term follow-up. 4D flow cardiovascular magnetic resonance (CMR) provides 3-directional velocity encoding and full volumetric coverage of the great arteries and may thus improve the hemodynamic evaluation in patients with CHD [3]. Some investigators had exploited these advantages of multi-dimensional flow imaging to derive new physiological and pathophysiological hemodynamic parameters, such as wall shear stress (WSS), or energy loss (EL) [4]. These advanced hemodynamic measurements can provide quantitative information on the impact of vascular disease on pulmonary blood flow patterns.Purpose
The aim of study is to 1) evaluate pulmonary valve regurgitation and the patency of the Goretex conduit using 4D flow CMR compare with controls. 2) assess the variation of advanced hemodynamic parameters of 2D axial WSS, 2D circumference WSS and EL in Gortex conduit.Methods
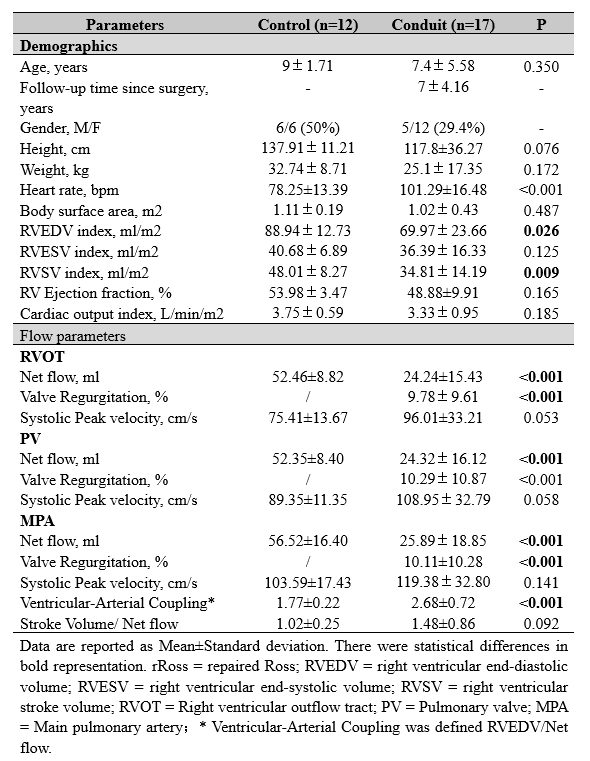
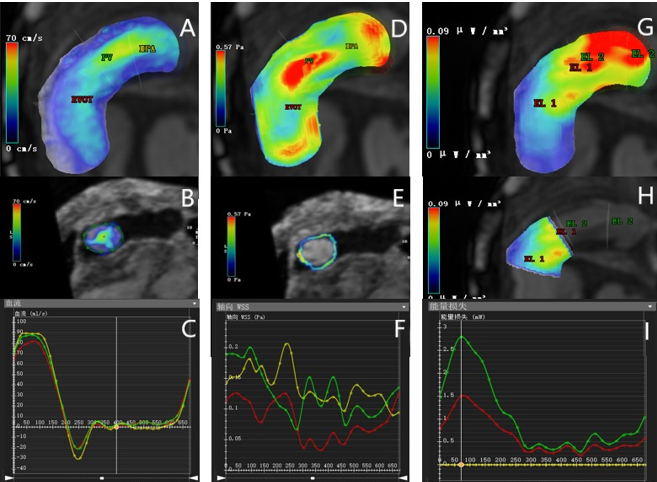
The CMR data was acquired from 12 healthy participants and 17 patients who were performed cine sequence in routine chamber view and 4D flow. CMR imaging was conducted on a 3.0 Tesla whole-body scanner (Prisma, Siemens, Germany) using a 32-channel phased-array cardiac coil. Whole heart 4D flow CMR was performed with spatial resolution=2.0-2.4×.2.0-2.4×2.0-2.4mm3, FOV=340×340mm, slab thickness=60-76 mm, temporal resolution=32-45ms, TE=2.2ms, TR=37.8ms, flip angle=15°, view per segment 2-3, velocity sensitivity(VENC)=200cm/s and with axial position coverage of the ventricle and arteries. Diaphragm navigation was used with efficiency value higher than 50% The average true scan time was 12-15 min. CMR image data obtained from CMR examination into the image analysis software CVi42 5.9 (CVI, Circle, Canada). Standard volumetric measurements were made from short-axis cine projections for CMR. 4D flow data was postprocessed by noise filtering, eddy current correction, and Maxwell equation correction. The image segmentation method using centerline extraction is used to extract the RVOT and aorta contour in the amplitude map (with more than 8 equally spaced sampling points), and complete the three-dimensional reconstruction of RVOT and the total pulmonary artery trunk. Blood flow, WSS and mechanical EL in 3 different planes of RVOT and the total pulmonary artery trunk ( PV was defined 2 mm above the handmade three-valve Goretex Conduit )were assessed. The mean ± standard deviation is used for continuous variables. The comparison between continuous variables was conducted using the student t-test, while skewness variables were tested using the Mann Whitney U-test.Results
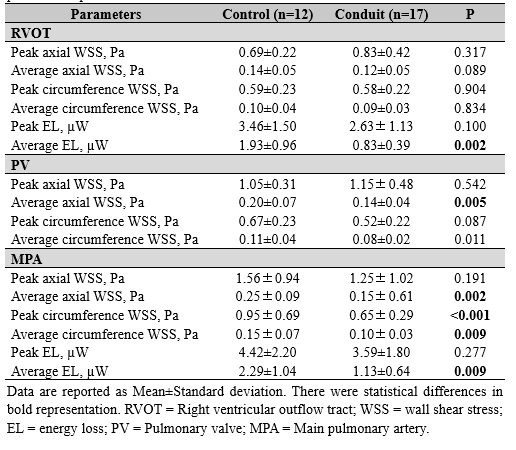
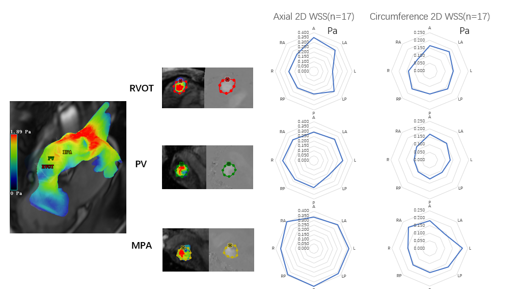
Mean age at surgery was 7±4.16 years. Median RVOT conduit size was 20 mm (range, 16–26 mm). RVEDV and RVSV in patients’ group were significantly lower than these in controls ((p=0.026 for RVEDV, p=0.009 for RVSV). Net flow of Conduit group was significantly lower than that of control group in RVOT plane PV plane, and MPA plane (all, p<0.001) Average EL of Conduit group was significantly lower than that of control group in RVOT plane and MPA plane (all, p<0.01). The significant difference of average axial WSS in PV plane and MPA plane (all, p<0.01) was existed between Conduit and control group. The significant difference of Peak and average circumference WSS in MPA plane (all, p<0.01) was also existed too. Highest axial segmental WSS was observed in the posterior, right posterior, and right anterior segments of the MPA as well as highest circumference segmental WSS in the left and right anterior segments of the MPA.Conclusions
Hemodynamic changes were detected in patients with right ventricular outflow tract reconstruction. Further long-term evaluation is necessary for the changes in segmental WSS in MPA.Acknowledgements
No acknowledgement found.References
1. Yamagishi M. Right ventricular outflow reconstruction using apolytetrafluoroethylene conduit with bulging sinuses and tricuspid fanshaped polytetrafluoroethylene valve. Oper Tech Thorac Cardiovasc Surg.2016, 21:211–229.
2. Delaney Marc,Cleveland Vincent,Mass Paige et al. Right ventricular afterload in repaired D-TGA is associated with inefficient flow patterns, rather than stenosis alone.[J] .Int J Cardiovasc Imaging, 2022, 38: 653-662.
3. van Ooij P, Markl M, Collins JD, et al. Aortic valve stenosis alters expression of regional aortic wall shear stress: New insights from a 4-dimensional flow magnetic resonance imaging study of 571 subjects. J Am Heart Assoc 2017;6(9).
4. Markl M, Schnell S, Wu C, et al. Advanced flow MRI: emerging techniques and applications.[J]. Clinical Radiology, 2016, 71(8):779-795.
Figures