3392
Real-time, multi-shot imaging improves image quality in an iCMR simulation study1Bioengineering, University of California San Diego, La Jolla, CA, United States, 2Department of Radiology, University of California San Diego, La Jolla, CA, United States, 3Department of Computer Science, University of California San Diego, La Jolla, CA, United States, 4Rady Children's Hospital-San Diego, San Diego, CA, United States, 5Department of Pediatrics, Division of Cardiology, University of California San Diego, La Jolla, CA, United States
Synopsis
Keywords: Cardiovascular, Heart
Motivation: Interventional cardiac MRI (iCMR) can be used to guide catheterizations, but image quality is limited by real-time imaging constraints (acquisition/reconstruction times).
Goal(s): To evaluate the extent to which real-time multi-shot imaging (via adaptive radial k-space sampling, ARKS) improves iCMR image quality relative to single-shot imaging.
Approach: Both ARKS and golden angle radial sampling were simulated using pediatric ECG recordings. Image quality was evaluated via mean squared error (MSE) and structural similarity index metric (SSIM).
Results: ARKS increases the number of samples available for reconstruction, relative to single shot imaging with the same temporal footprint. This led to lower MSE and higher SSIM.
Impact: Multi-shot real-time imaging has the potential to significantly improve interventional imaging by increasing the amount of data available for image reconstruction. In this study, we demonstrate that combining multi-shot data can improve image quality.
Introduction
Current iCMR relies on single-shot imaging in which the most recently acquired MRI samples are used to reconstruct images. To avoid cardiac blurring, the number of samples is limited, thus reducing the quality of iCMR images. Adaptive radial k-space sampling (ARKS) is an approach which enables real-time, multi-shot imaging by quickly finding MRI samples that were obtained at a similar point in the cardiac cycle1. Not only does ARKS increase the amount of data available, but it can also improve the angular distribution of samples.However, the ability of ARKS to improve image quality in a real-time iCMR setting has not been quantified. Therefore, we have conducted a simulation study to compare ARKS to single shot methods. We use physiologic recordings of pediatric patients who underwent clinical MRIs and simulate k-space sampling using fully sampled short-axis ECG-gated cine images from the open-source Automated Cardiac Diagnosis Challenge (ACDC) dataset2.
Methods
Twenty ECGs recorded during 4D flow imaging in non-sedated pediatric patients were analyzed with IRB approval. The median age was 12.9 years old, (IQR: 11.5-14.7), the median heart rate was 75.7 bpm, (IQR: 67.7-95.0), and gender ratio was 50% female. We simulated iCMR imaging as a 2D radial bSSFP acquisition sequence with TR = 2.6ms. The duration of the iCMR simulation was 110 seconds.One cardiac cycle was automatically selected for analysis of image quality (at 80% of the simulation). For single-shot imaging, golden angle radial k-space sampling was used. We defined three different single shot methods (short, medium, long) which used different number of MRI samples: 10, 45, and 65, respectively. The “short” method matched the temporal footprint used by ARKS (26msec or 10 radial spokes) whereas “long” matched the median number of samples available for ARKS reconstruction (169mse or 65 spokes). We hypothesize that ARKS will have improved image quality compared to single-shot methods, specifically the short single-shot which should suffer from extreme undersampling. The trajectories of both simulations were computer in MATLAB (Version, Mathworks) and data reconstruction were performed in PyTorch.
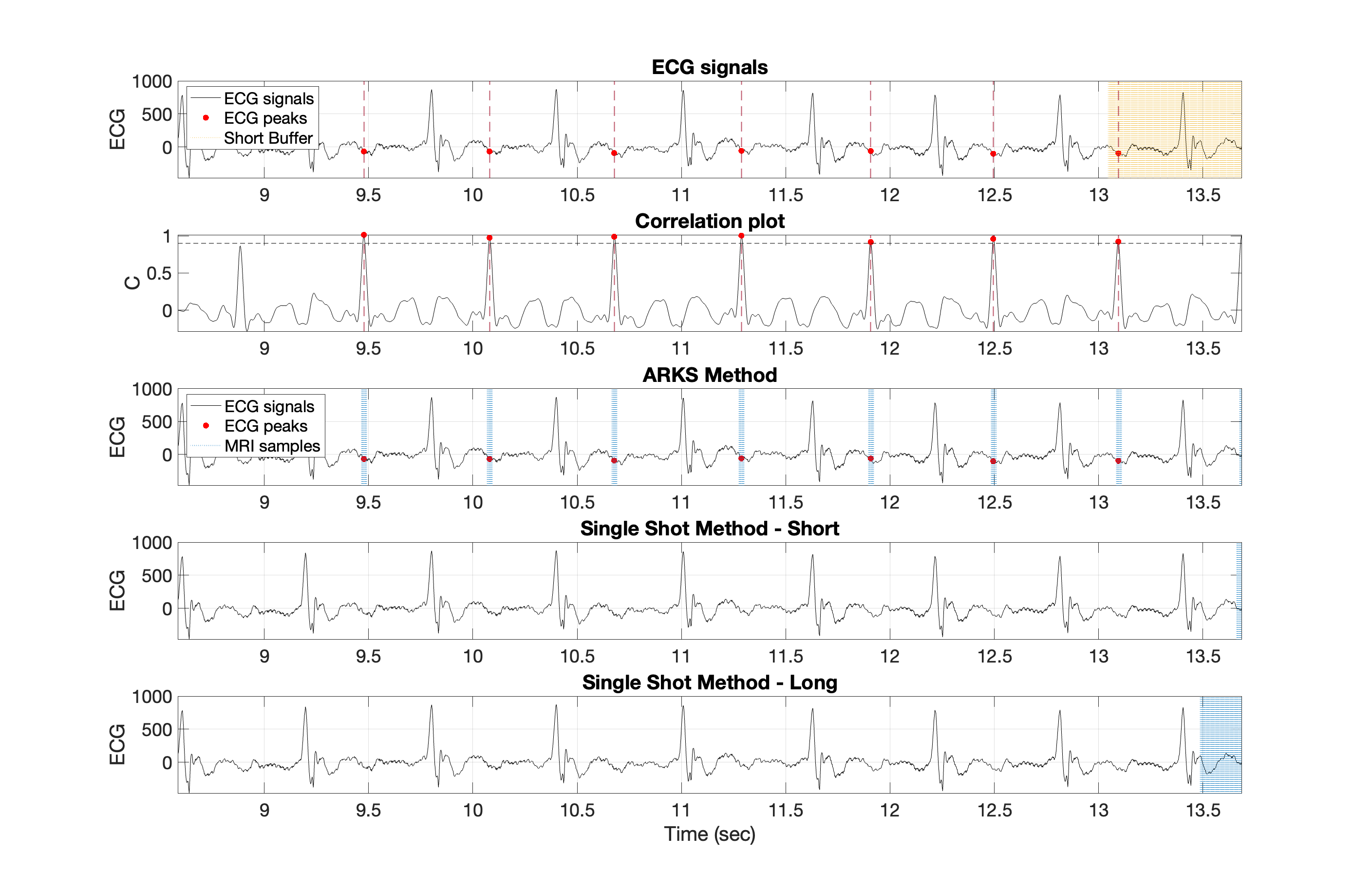
ARKS selects MRI data previously acquired at the current cardiac position using the ECG cross correlation plot shown in Figure 1. Based on each patient’s median RR interval, each MRI sample was assigned a % cardiac cycle value. This was used to sample the correct image from the ECG-gated cine movie obtained from the open-source ACDC dataset2.
Single receiver coil reconstruction was performed using nonuniform fast Fourier transform3,4. Mean Square Error (MSE) and Structural Similarity Index (SSIM) were utilized to quantify image quality differences in multi-shot imaging versus single-shot imaging. Friedman's test and Wilcoxon-Signed Rank tests were used to analyze differences in median image quality metrics across simulation methods.
Result
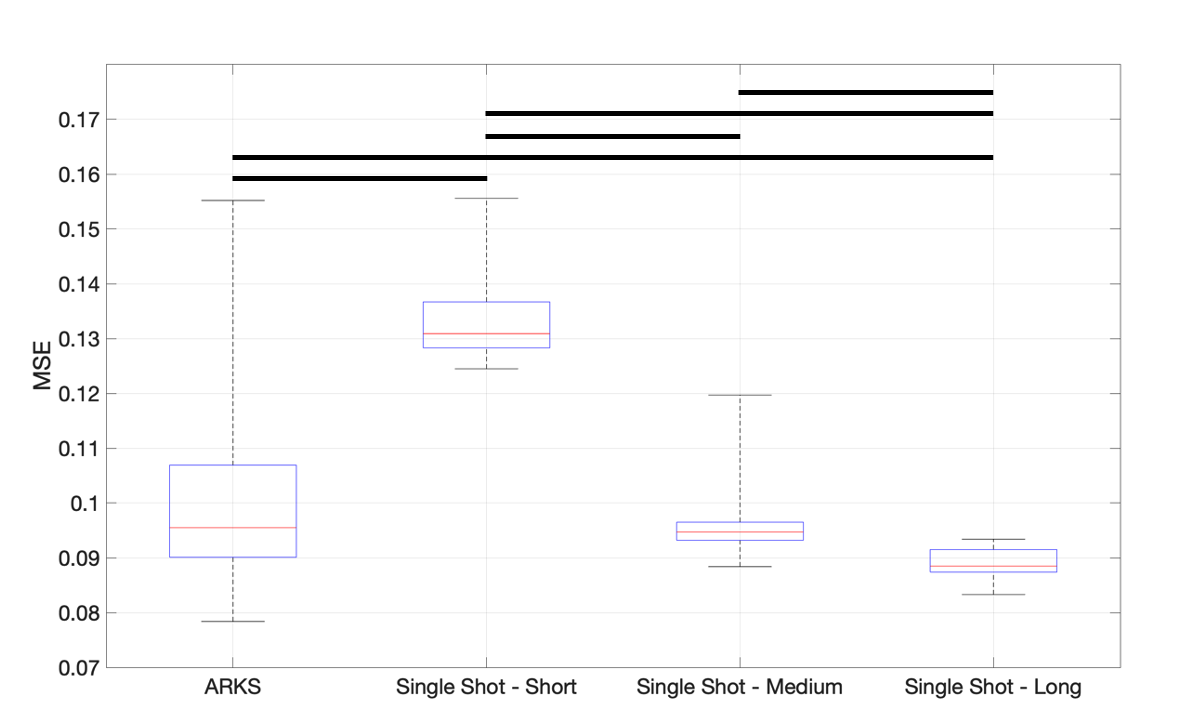
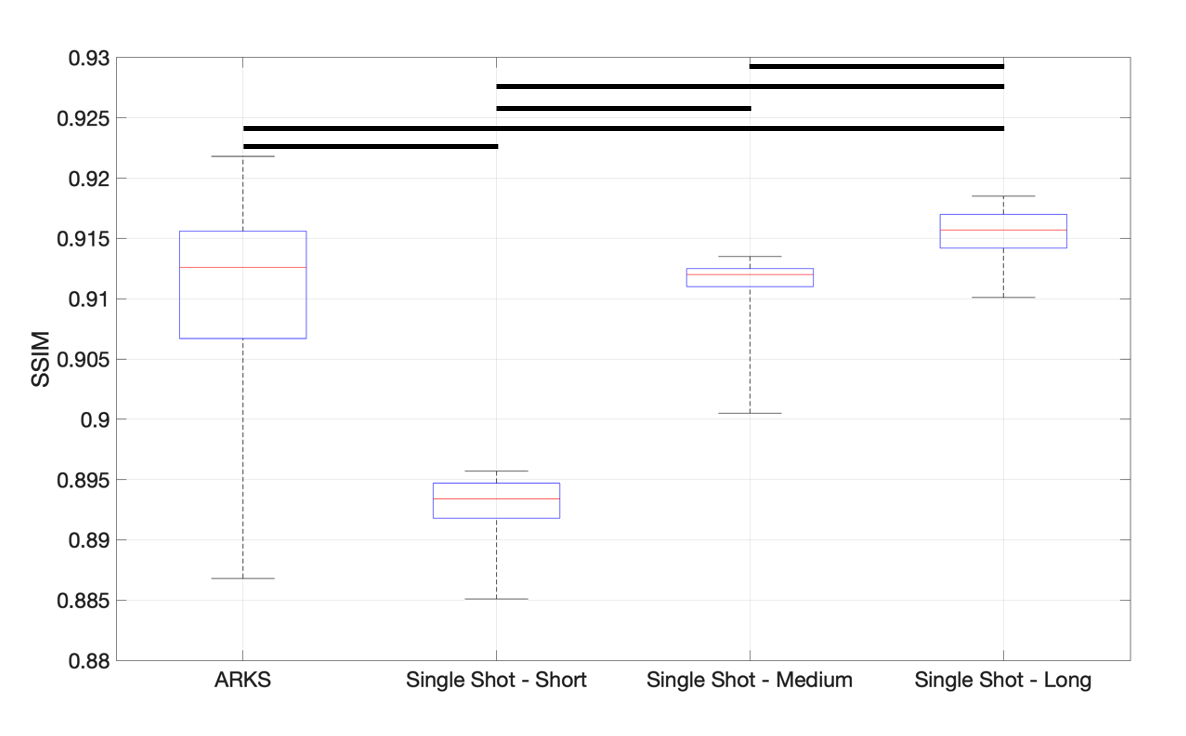
Each pediatric ECG data had a different number of frames created with respect to their cardiac cycle. MSE of images acquired with ARKS was lower (p<0.05) than those generated with short single-shot and higher (p>0.05) compared to long single-shot. The improvement over short single shot is likely due to a reduction in radial streaks. The lack of improvement compared to long singe shot is attributed to MSE not penalizing blurring of myocardial boundaries. No difference (p>0.05) was observed between ARKS and medium single-shot.In terms of SSIM, ARKS exhibited an SSIM value higher (p<0.05) than short single-shot, but lower than long single-shot. Similar to MSE, the SSIM of medium single-shot was not different (p>0.05) from ARKS.
Discussion & Conclusions
We have shown that ARKS method has better image quality than short single-shot reconstructions in simulations. Therefore, further study would be required to test its robustness in vivo and in an iCMR setting.Contrary to our initial hypothesis, the image quality of the long single-shot method was better than ARKS. A potential explanation may be that when we calculated SSIM and MSE across the entire image. Therefore, reduction of streak artifacts outside of the heart area could outweigh any potential cardiac blurring. In addition, ARKS adapts dynamically to the physiologic signal so the number of spokes available for reconstruction varies throughout the reconstruction. This could also lead to a relative increase in imaging metrics in a single shot since it can have a higher number of views. Finally, one limitation of this study is that although we used 20 different patients’ ECG data, the same cardiac cine MRI data was used for image simulations.
Acknowledgements
NIH R01 HL162671: Improved MRI Guidance of Pediatric Catheterization via Autonomous Multi-Beat Data SynthesisReferences
(1) Contijoch F, Han Y, Kamesh Iyer S, et al. Closed-loop control of k-space sampling via physiologic feedback for cine MRI. PLoS One. 2020;15(12):e0244286. Published 2020 Dec 29. doi:10.1371/journal.pone.0244286
(2) O. Bernard, A. Lalande, C. Zotti, F. Cervenansky, et al. "Deep Learning Techniques for Automatic MRI Cardiac Multi-structures Segmentation and Diagnosis: Is the Problem Solved ?" in IEEE Transactions on Medical Imaging, vol. 37, no. 11, pp. 2514-2525, Nov. 2018 doi: 10.1109/TMI.2018.2837502
(3) Lin, Jyh-Miin. “Python Non-Uniform Fast Fourier Transform (PyNUFFT): An Accelerated Non-Cartesian MRI Package on a Heterogeneous Platform (CPU/GPU).” Journal of Imaging 4.3 (2018): 51. (
4) J.-M. Lin and H.-W. Chung, Pynufft: python non-uniform fast Fourier transform for MRI Building Bridges in Medical Sciences 2017, St John’s College, CB2 1TP Cambridge, UK
Figures