3390
Signal intensity and volume of carotid intraplaque hemorrhage on MRI and ipsilateral cerebrovascular events: the Plaque At RISK (PARISK) study1Department of Radiology and Nuclear Medicine, Maastricht University Medical Centre, Maastricht, Netherlands, 2Cardiovascular Research Institute Maastricht (CARIM), Maastricht University, Maastricht, Netherlands, 3Department of Radiology and Nuclear Medicine, Erasmus University Medical Center, Rotterdam, Netherlands, 4Department of Neurology, Erasmus University Medical Center, Rotterdam, Netherlands, 5Department of Neurology, Amsterdam University Medical Center, Amsterdam, Netherlands, 6Department of Neurology, Zuyderland Medical Center, Heerlen, Netherlands, 7Department of Neurology, Zuyderland Medical Center, Sittard, Netherlands, 8School for Mental Health and Neuroscience (MHeNs), Maastricht University, Maastricht, Netherlands, 9Department of Epidemiology, Erasmus University Medical Center, Rotterdam, Netherlands, 10Department of Radiology and Nuclear Medicine, University Medical Center Utrecht, Utrecht, Netherlands, 11Department of Radiology, Leiden University Medical Center, Leiden, Netherlands, 12Department of Neurology, Maastricht University Medical Centre, Maastricht, Netherlands, 13Department of Clinical Neurophysiology, Maastricht University Medical Centre, Maastricht, Netherlands
Synopsis
Keywords: Atherosclerosis, Stroke
Motivation: The presence of intraplaque hemorrhage (IPH) is a strong independent stroke predictor. Higher IPH signal intensity ratios (SIR) and volumes were found in symptomatic versus asymptomatic carotid arteries.
Goal(s): To determine if IPH SIR and volume are associated with the risk for ipsilateral ischemic neurovascular events in symptomatic patients with <70% carotid stenosis.
Approach: Cox proportional hazards and logistic regression were used to explore the association of IPH SIR and volume to ipsilateral ischemic neurovascular events in 87 IPH-positive patients.
Results: IPH SIR and IPH volume were not associated with risk for ipsilateral ischemic events during 5.1(IQR:3.1-5.6) years.
Impact: No association was found between IPH SIR or volume and the risk for ipsilateral ischemic neurovascular events or new infarcts on brain MRI. Therefore, identifying the presence of IPH is sufficient for risk stratification.
Introduction
The Plaque at RISK study (PARISK) study demonstrated that patients with a carotid plaque positive for intraplaque hemorrhage (IPH) have an increased risk of recurrent ipsilateral ischemic cerebrovascular events1. It was previously reported that symptomatic carotid plaques with IPH showed higher IPH signal intensity ratios (SIR) and larger IPH volumes than asymptomatic plaques2,3. Hence, we explored whether IPH SIR and IPH volume are associated with the risk for ipsilateral ischemic cerebrovascular events beyond the presence of IPH.Methods
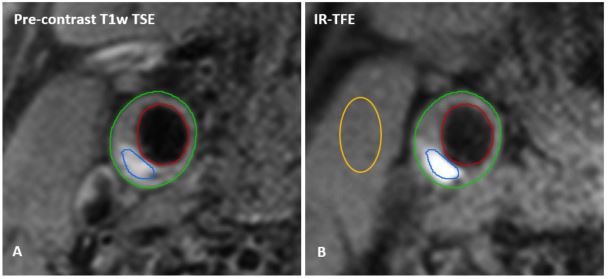
TIA and ischemic stroke patients with mild-to-moderate carotid stenosis and an ipsilateral IPH-positive carotid plaque (n=87) from the PARISK study were included. Patients were clinically followed-up for 5 years and brain MRI (n=69) was acquired after 2 years to identify new ipsilateral brain infarcts. Trained observers delineated the IPH, defined as a hyperintense region compared to surrounding muscle tissue on hyper T1-weighted MRI images (3D Fast Spoiled Gradient Echo (FSPGR) or 3D-T1w Inversion Recovery (IR) Turbo Field Echo (TFE)) acquired on a 3.0 Tesla MRI system with dedicated carotid coils (Figure 1). Fifteen transverse adjoining slices of 2 mm of the extracranial carotid artery, centered on the carotid plaque, were acquired. The IPH SIR was defined as the highest signal intensity in the IPH region divided by the mean signal intensity of the adjacent muscle tissue4. Kaplan-Meijer plots including log rank (Mantel-Cox) tests were used to illustrate the cerebrovascular event-free survival probability related to a high versus low IPH SIR or high versus low IPH volume. The associations between IPH SIR or volume and recurrent ipsilateral ischemic cerebrovascular events or new infarcts on brain MRI were investigated using Cox-proportional hazard models and logistic regression.Results
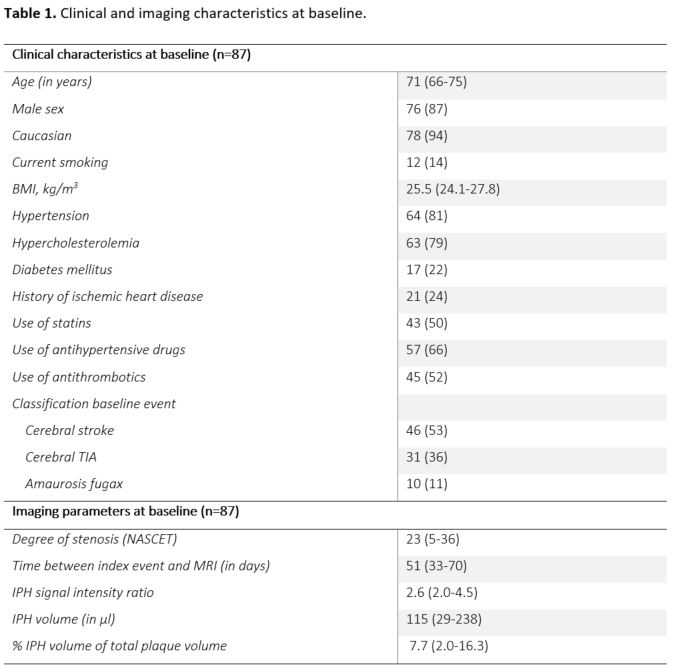
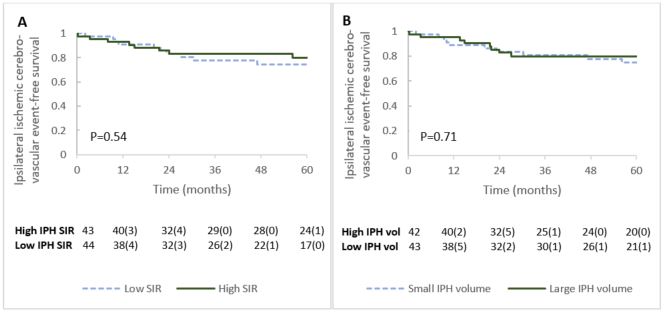
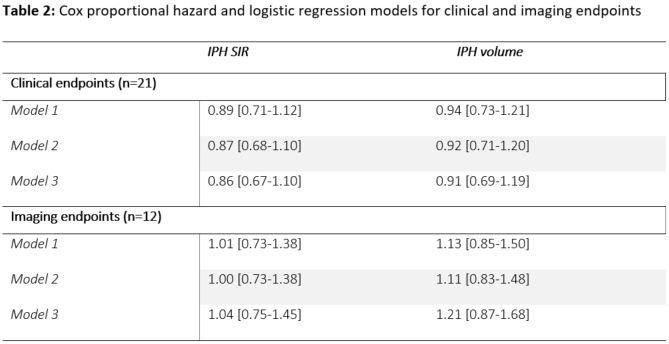
During a median clinical follow-up of 5.1 (IQR: 3.1-5.6) years, out of 87 patients (Table 1) 21 patients experienced a total of 22 clinical ipsilateral ischemic events (i.e., 9 ischemic strokes, 11 TIAs, and 2 amaurosis fugax events) and 12 new ipsilateral brain infarcts on MRI were identified. The median IPH SIR was 2.6 (IQR: 2.0-4.5) and the median IPH volume was 115 µl (IQR: 29-238). The cerebrovascular event-free survival probability of patients with a high versus low IPH SIR and high versus low IPH volume (Figure 2) was not significantly different (p= 0.54 and p=0.71, respectively). Cox proportional hazard models also found no association for IPH SIR (HR: 0.89 [95% CI: 0.67-1.10] or IPH volume (HR: 0.91 [0.69-1.19] with ipsilateral ischemic cerebrovascular events (Table 2). Logistic regression of IPH SIR (OR: 1.04 [0.75-1.45]) and IPH volume (OR: 1.21 [0.87-1.68] per 100 µl increase) did not detect an association with new ipsilateral infarcts on brain MRI.Discussion
We demonstrated that IPH SIR and IPH volume were not associated with the risk for ipsilateral ischemic cerebrovascular event recurrence or new infarcts identified on brain MRI. While several cross-sectional studies have reported a higher IPH SIR or larger IPH volume in symptomatic carotid plaques versus asymptomatic plaques, the potential association between these parameters and future ischemic cerebrovascular events had, to our knowledge, not yet been explored. The major limitation of our study is that the sample size is limited, since we could only include patients from the PARISK study with an IPH-positive plaque. Regardless, the hazard ratios for IPH SIR and volume reported in this study, even at the upper bound of the 95% CI, are small and therefore not clinically relevant. Sample size improvement could indicate a weak association with new ipsilateral ischemic events at best. In contrast to IPH SIR and volume, IPH presence itself showed a strong and independent association with cerebrovascular event recurrence as previously reported by the PARISK study and a large meta-analysis1,5. While quantification of IPH SIR and volume does not offer improved prognostic value for the risk of recurrent ipsilateral cerebrovascular events, the finding is valuable for clinical implementation. The identification of IPH presence on MRI as a predictor is much easier in daily clinical practice compared to the additional time-consuming quantification of IPH signal intensity and volume.Acknowledgements
The authors want to thank all researchers, clinicians, and participants involved for their contribution to the Plaque at RISK study (PARISK) study. Participating centers: Academic Medical Center, Amsterdam (P.J. Nederkoorn); Erasmus MC, University Medical Center Rotterdam, Rotterdam (A. van der Lugt and P.J. Koudstaal); Flevoziekenhuis, Almere (M. Limburg); Kennemer Gasthuis, Haarlem (M. Weisfelt); Laurentius Ziekenhuis, Roermond (A.G. Korten); Maasstad Ziekenhuis, Rotterdam (R. Saxena); Maastricht University Medical Center (M.E. Kooi, R.J. van Oostenbrugge, W.H. Mess); Orbis Medisch Centrum, Sittard and Heerlen (N.P. van Orshoven, A.H.C.M.L. Schreuder); Sint Antonius Ziekenhuis, Nieuwegein (S.C. Tromp); Sint Franciscus Gasthuis, Rotterdam (S.L.M. Bakker); Slotervaartziekenhuis, Amsterdam (N.D. Kruyt); Tergooi Ziekenhuizen Hilversum/Blaricum (J.R. de Kruijk); University Medical Center Utrecht (J. Hendrikse, G.J. de Borst); Viecuri Medisch Centrum, Venlo (B.J. Meems); Vlietland Ziekenhuis, Schiedam (J.C.B. Verhey); IJsselland Ziekenhuis, Capelle aan den IJsel (A.D. Wijnhoud).References
1. Dam-Nolen DHKv, et al. Carotid Plaque Characteristics Predict Recurrent Ischemic Stroke and TIA. JACC: Cardiovascular Imaging. 2022;15(10):1715-26.
2. Wang X, Sun J, Zhao X, Hippe DS, Hatsukami TS, Liu J, et al. Ipsilateral plaques display higher T1 signals than contralateral plaques in recently symptomatic patients with bilateral carotid intraplaque hemorrhage. Atherosclerosis. 2017;257:78-85.
3. Benson JC, Savastano L, Nardi V, Lanzino G, Lerman A, Brinjikji W. Intraplaque CTA characteristics as predictors of symptomatology: a semiautomated volumetric analysis. Emerg Radiol. 2022;29(1):75-80.
4. Larson AS, Brinjikji W, Kroll NJ, Savastano L, Huston J, 3rd, Benson JC. Normalized intraplaque hemorrhage signal on MP-RAGE as a marker for acute ischemic neurological events. Neuroradiol J. 2022;35(1):112-8.
5. Schindler A, Schinner R, Altaf N, Hosseini AA, Simpson RJ, Esposito-Bauer L, et al. Prediction of Stroke Risk by Detection of Hemorrhage in Carotid Plaques: Meta-Analysis of Individual Patient Data. JACC Cardiovasc Imaging. 2020;13(2 Pt 1):395-406.
Figures