3389
PCASL with a clinically practical ischemia-hyperemia protocol for use in critical limb threatening ischemia1Imaging, University College London, London, United Kingdom, 2Centre for Medical Imaging, University College London, London, United Kingdom, 3Imaging, University College London Hospital, London, United Kingdom, 4Vascular Surgery, University College London, London, United Kingdom, 5Medical Physics and biomedical engineering, University College London Hospital, London, United Kingdom
Synopsis
Keywords: Vascular, Arterial spin labelling
Motivation: Lower-limb vascular imaging used in advanced peripheral arterial disease PAD) is limited to luminography with no functional tissue perfusion data.
Goal(s): MRI ASL perfusion quantification is a contrast agent free technique that promises to be a novel imaging biomarker for tissue viability. However, current implementations have several limitations, including low signal-to-noise and the need for a substantial period of hyperemia to induce measurable perfusion in the muscle.
Approach: We aimed to develop an abbreviated, clinically-practical ischemia-hyperemia paradigm to measure perfusion, and to evaluate this in volunteers.
Results: A 2-minute period of ischemia produced hyperemia a doubling of baseline perfusion, sustained for 30 seconds.
Impact: Quantitative perfusion imaging with pseudocontinuous arterial spin labelling can be achieved in the lower limb with an ischemia-hyperemia paradigm with 2 minutes of ischemia. This clinically applicable technique can be used in the assessment of peripheral arterial disease.
Introduction
Chronic limb threatening ischemia (CLTI) represents the most severe end of the spectrum of peripheral arterial disease (PAD) [1]. The prevalence of symptomatic PAD is approximately 2.5% [2] and limb amputation is required in 4% of patients with PAD [3]. Investigations in the assessment of CLTI include cross-sectional angiography, ultrasound and arterial brachial pressure indices (ABPI); these tests are limited to luminography, whilst ABPI is often inconclusive in CLTI due to incompressible arteries and pain. No gold standard imaging technique can quantify the deficits in muscle perfusion. A clinically practical non-invasive quantitative imaging perfusion test would allow earlier detection of tissue ischemia and provide a benchmark for assessing disease progression.Quantitative perfusion imaging with MRI using arterial spin labelling (ASL) is an attractive modality to assess this cohort of patients; it is free of nephrotoxic contrast agents and can be performed as part of standard of care MR angiography [4]. However, this technique is challenging owing to inherent low baseline muscle blood flow and low signal to noise ratio [5–7]. Perfusion measurements are performed after induced hyperemia in order to plot a time resolved curve of signal, which has been shown by other groups to unmask perfusion deficits in PAD and correlate with severity of PAD [6,8–10]. Hyperemia however is reportedly short lived for around 20 seconds [11,12]. The majority of prior studies have used employed periods of ischemia up to 5minutes which is impractical when applied to CLTI.
The purpose of this research was to test whether muscle perfusion can be measured with ASL using an IHP and exercise protocol.
Methods
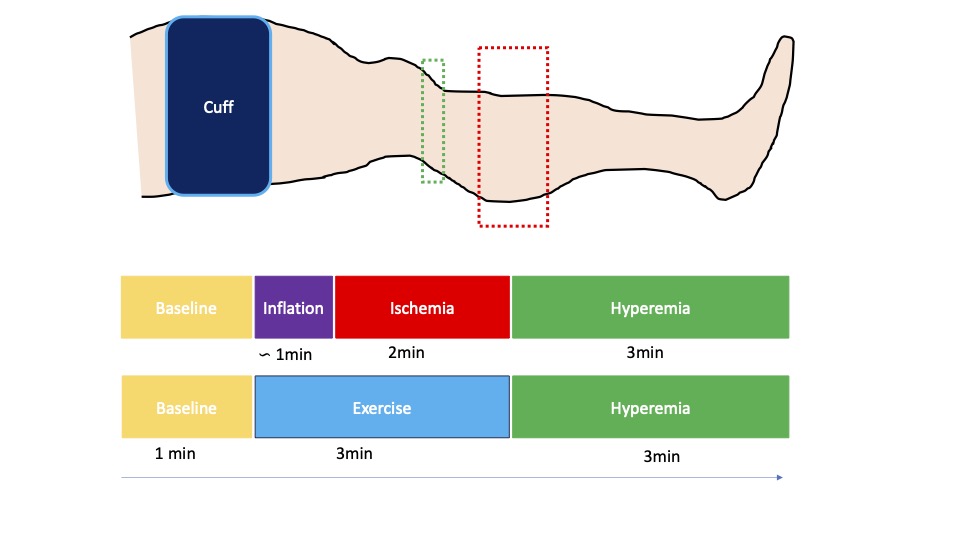
Induction of muscle hyperaemia:Two in-bore techniques were compared: ischemia hyperemia paradigm (IHP) and a period of 3 minutes of resistance exercise with a 5kg weight on a pulley. IHP was achieved with a tourniquet placed around the thigh of one leg and inflated to 200mmHg for up to 2 minutes and then rapidly deflated( the contralateral limb was a control).
Arterial spin labelling acquisition:
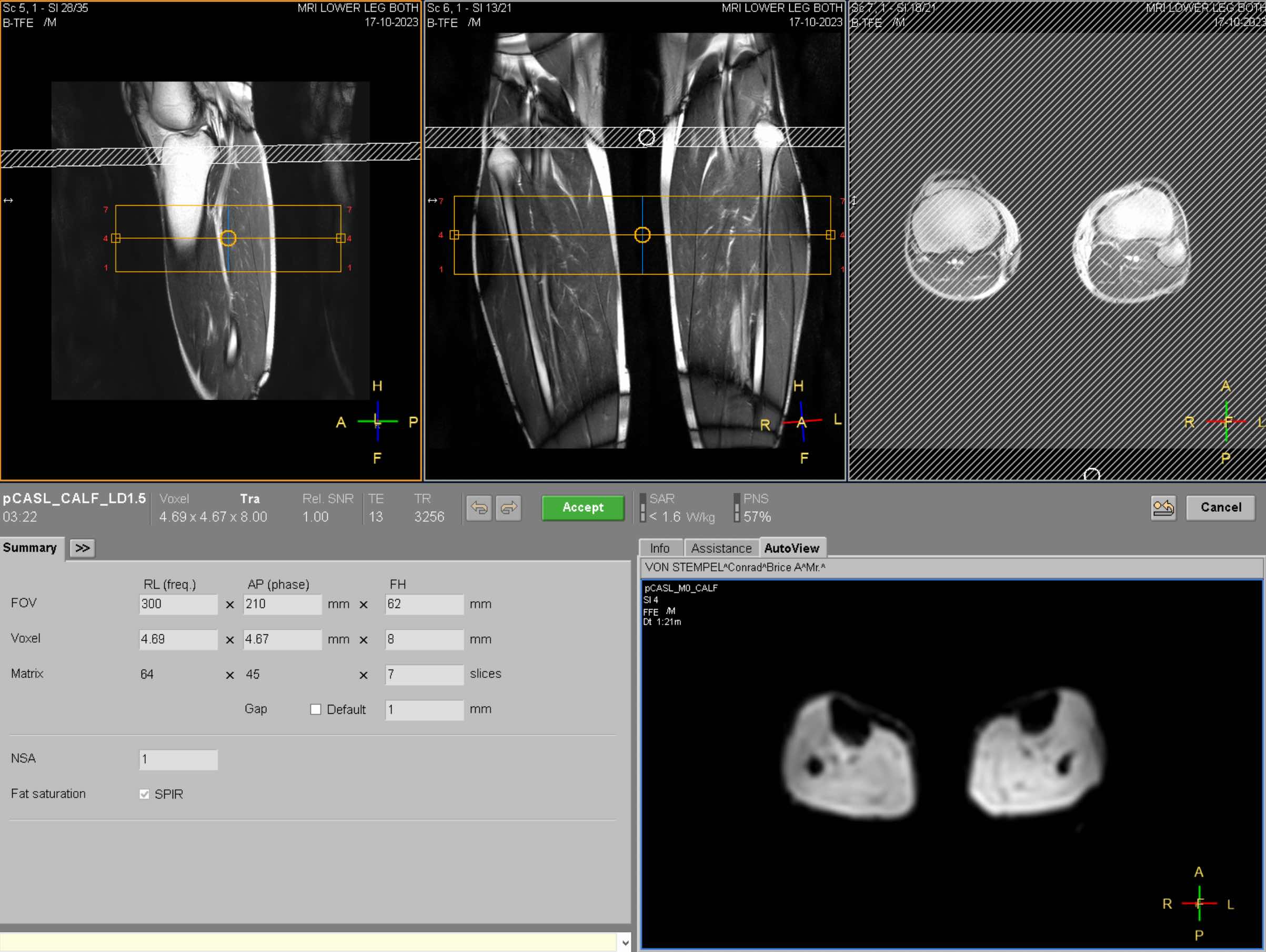
ASL was performed continuously at rest (1 minute) during both ischemia (2minutes) and hyperemia (3minutes) in the IHP experiments and for 5 minutes during and after exercise. An 8 channel surface coil was placed over the lower legs elevated with a foam support structure. Pseudocontinuous ASL (PCASL) was perfomed at 3T with a 1.5second labelling duration and 1.5second post labelling delay. The labelling plane positioned perpendicularly in the popliteal artery and measurements were performed in a 6cm region of interest in calf muscle. Anatomical sequences were performed through the lower limb to facilitate segmentation of muscle groups and correct for motion.
Blood flow measurements:
ASL data from the soleus muscles of both legs was segmented manually (ITK-SNAP). Perfusion weighted image maps and limb blood flow (LBF) was calculated using the mathematical model derived from the general solution to the Bloch equation for longitudinal magnetisation of tissue as described by Detre et al [13] with the assumptions of a blood-muscle coefficient of 0.9ml/g and T1 relaxation of blood at 3T of 1650ms.
Results
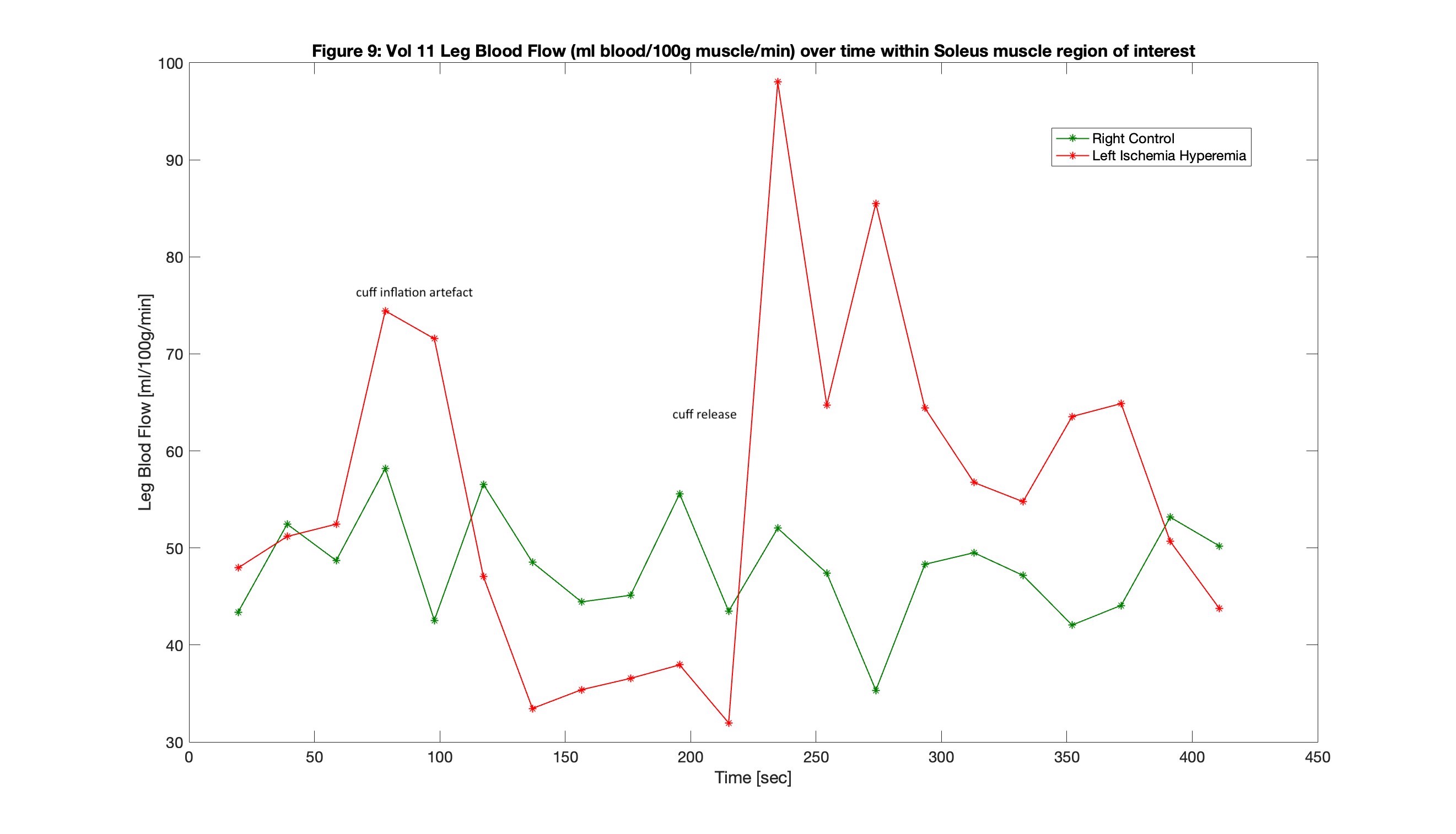
A measurable hyperemia was detected with IHP protocol in 8 studies using 2 minutes of ischemia: There was significant increase in muscle perfusion in the soleus during hyperemia compared to the control limb (60.5 vs 45.3 ml/100g/min p=0.023) and compared to preceding ischemia (median 34.3ml/100g/min) with a median peak perfusion during hyperemia of 70.5ml/100g/min. Median length of hyperemia was 39 seconds (IQR 12.25-56.75).Post exercise measurements were performed in 5 participants. No significant increase in LBF after exercise compared to baseline resting LBF was detected in the soleus muscle (31 vs 36.5 ml/100g/min; p = 0.49).
Discussion
These results suggest that a short period of cuff induced ischemia (2 minutes) can reliably induce a measurable hyperemic stimulus that persists for around half a minute with a muscle perfusion approximately double that of baseline. This is a clinically applicable protocol that can be readily applied to patients with even severe PAD. The degree and magnitude of hyperemia measured using this abbreviated protocol is consistent with the previous studies using ASL in lower limb muscle that have employed longer periods of ischemia of up to 5 minutes [6].Conclusion
A clinically practical IHP protocol with 2 minutes of ischemia provided a measurable sustained hyperemic stimulus double that of baseline. This promises to lower the existing barriers to the use of ASL in clinical practice, particularly for patients with critical limb-threatening ischemia.Acknowledgements
This work was supported by the UK Royal College of Radiologists. Timothy J.P. Bray is supported by the UCLH National Institute for Health Research (NIHR) Biomedical Research Centre (BRC). This work was undertaken at UCLH/UCL, which receives funding from the UK Department of Health’s NIHR BRC funding scheme. The views expressed in this publication are those of the authors and not necessarily those of the UK Department of Health.References
- Vos T, Abajobir AA, Abbafati C, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. The Lancet. Published online 2017. doi:10.1016/S0140-6736(17)32154-22.
- Cea-Soriano L, Fowkes FGR, Johansson S, Allum AM, García Rodriguez LA. Time trends in peripheral artery disease incidence, prevalence and secondary preventive therapy: A cohort study in the Health Improvement Network in the UK. BMJ Open. 2018;8(1). doi:10.1136/bmjopen-2017-0181843.
- Ahmad N, Thomas GN, Gill P, Torella F. The prevalence of major lower limb amputation in the diabetic and non-diabetic population of England 2003-2013. Diab Vasc Dis Res. 2016;13(5):348-353. doi:10.1177/14791641166513904.
- NICE. Peripheral Arterial Disease: Diagnosis and Management Clinical Guideline.; 2012. www.nice.org.uk/guidance/cg1475.
- Boushel R, Langberg H, Olesen J, et al. Regional blood flow during exercise in humans measured by near-infrared spectroscopy and indocyanine green. J Appl Physiol. 2000;89(5). doi:10.1152/jappl.2000.89.5.18686.
- Englund EK, Rodgers ZB, Langham MC, Mohler ER, Floyd TF, Wehrli FW. Measurement of skeletal muscle perfusion dynamics with pseudo-continuous arterial spin labeling (pCASL): Assessment of relative labeling efficiency at rest and during hyperemia, and comparison to pulsed arterial spin labeling (PASL). Journal of Magnetic Resonance Imaging. 2016;44(4):929-939. doi:10.1002/jmri.252477.
- Raynaud JS, Duteil S, Vaughan JT, et al. Determination of Skeletal Muscle Perfusion Using Arterial Spin Labeling NMRI: Validation by Comparison With Venous Occlusion Plethysmography.; 2001.8.
- Wu WC, Mohler E, Ratcliffe SJ, Wehrli FW, Detre JA, Floyd TF. Skeletal Muscle Microvascular Flow in Progressive Peripheral Artery Disease. Assessment With Continuous Arterial Spin-Labeling Perfusion Magnetic Resonance Imaging. J Am Coll Cardiol. 2009;53(25):2372-2377. doi:10.1016/j.jacc.2009.03.0339.
- Chen HJ, Roy TL, Wright GA. Perfusion measures for symptom severity and differential outcome of revascularization in limb ischemia: Preliminary results with arterial spin labeling reactive hyperemia. Journal of Magnetic Resonance Imaging. 2018;47(6):1578-1588. doi:10.1002/jmri.2591010.
- Suo S, Zhang L, Tang H, et al. Evaluation of skeletal muscle microvascular perfusion of lower extremities by cardiovascular magnetic resonance arterial spin labeling, blood oxygenation level-dependent, and intravoxel incoherent motion techniques. Journal of Cardiovascular Magnetic Resonance. 2018;20(1). doi:10.1186/s12968-018-0441-311.
- Nishiyama SK, Wray DW, Richardson RS. Aging affects vascular structure and function in a limb-specific manner. J Appl Physiol. 2008;105(5). doi:10.1152/japplphysiol.90612.200812.
- Langham MC, Jain V, Magland JF, Wehrli FW. Time-resolved absolute velocity quantification with projections. Magn Reson Med. 2010;64(6). doi:10.1002/mrm.2255913.
- Detre JA, Leigh JS, Williams DS, Koretsky AP. Perfusion imaging. Magn Reson Med. 1992;23(1):37-45. doi:10.1002/mrm.191023010614.
- Lopez D, Pollak AW, Meyer CH, et al. Arterial spin labeling perfusion cardiovascular magnetic resonance of the calf in peripheral arterial disease: Cuff occlusion hyperemia vs exercise. Journal of Cardiovascular Magnetic Resonance. 2015;17(1). doi:10.1186/s12968-015-0128-y
Figures