3385
Fibrous cap status, plaque surface morphology, and intraplaque hemorrhage volume over two years in patients with carotid plaques: PARISK study1Cardiovascular Research Institute Maastricht (CARIM), MAASTRICHT, Netherlands, 2Department of Radiology and Nuclear Medicine, Maastricht University Medical Center, MAASTRICHT, Netherlands, 3Department of Radiology and Nuclear Medicine, Erasmus MC, University Medical Center Rotterdam, Rotterdam, Netherlands, 4Department of Neurology, Amsterdam UMC, location AMC, Amsterdam, Netherlands, 5Department of Radiology, University Medical Center Utrecht, Utrecht, Netherlands, 6Department of Clinical Neurophysiology, Maastricht University Medical Center, maastricht, Netherlands, 7Department of Epidemiology, Erasmus MC, University Medical Center Rotterdam, Rotterdam, Netherlands, 8Department of Epidemiology, Maastricht University, maastricht, Netherlands, 9Department of Neurology, Maastricht University Medical Center, MAASTRICHT, Netherlands
Synopsis
Keywords: Atherosclerosis, Atherosclerosis, Carotid, Stroke
Motivation: We explored the relationship between intraplaque hemorrhage (IPH) and thin/ruptured fibrous cap (TRFC) or disrupted plaque surface.
Goal(s): We investigated the relationship between a TRFC/disrupted plaque surface and the change in carotid IPH volume
Approach: Longitudinal carotid MR study in 110 symptomatic patients with mild-to-moderate carotid stenosis.
Results: Baseline MR images revealed a larger IPH volume in patients with a TRFC/disrupted plaque surface and the IPH volume (tended to) decrease during follow-up. However, part of patients with a TRFC/disrupted plaque surface at baseline had a higher risk of IPH progression.
Impact: Identifying patients at higher risk of IPH progression allows for timely monitoring and intervention, potentially reducing the incidence of stroke. This research contributes to improved quality of life for individuals at risk of carotid IPH-related complications
Introduction
Carotid intraplaque hemorrhage (IPH) is a strong predictor of stroke (1, 2), but factors contributing to IPH development are incompletely understood. Cross-sectional studies have demonstrated an association between IPH and a thin/ruptured fibrous cap (TRFC)/disrupted plaque surface (3). We aim to investigate the relationship between a TRFC/disrupted plaque surface and the change in IPH volume in a longitudinal study in symptomatic patients with mild-to-moderate carotid stenosis.Methods
Recent TIA and stroke patients with ipsilateral carotid plaques were derived from the Plaque At Risk (PARISK) study (4). Multisequence carotid MRI was performed using dedicated coils on 3.0 T whole-body MRI scanners and CTA of the carotid artery was performed if no contraindications for CTA were present as described before (5). We analyzed IPH and fibrous cap status (thick versus TRFC) on the baseline and 2-year follow-up MRI in 110 patients (Figure 1). Plaque surface (smooth versus disrupted (fissure/ulceration)) on CTA was assessed in 93 patients at baseline and 70 patients at follow-up. The median change in IPH volume over the two-year period was computed. To evaluate the variation in IPH quantification between different observers, we calculated the mean coefficient of variation (100% * standard deviation (SD)/ mean) (6). This analysis was conducted by comparing IPH volumes determined independently by five trained readers, blinded to other readers' results in a group of 17 patients. The mean coefficient of variation for IPH volume was 11%. A threshold for IPH progression or regression was defined as twice the mean coefficient of variation, equivalent to 2 standard deviations (2SDs), thus a positive or negative change in volume of more than 22% was defined as progression or regression, while smaller changes were considered as no change. The risk of IPH progression was compared between patients with a thick versus TRFC and smooth versus disrupted plaque surface. Multivariate logistic regression was used to evaluate the association between TRFC/disrupted plaque surface at baseline and the risk of IPH being present at follow-up after adjustment for baseline IPH volume and potential confounders.Results
Patients with a TRFC at baseline had a higher median baseline IPH volume than patients with a thick fibrous cap (97.3 mm3, IQR [3.2-193.3 mm3] vs. 0.0 mm3, p<0.05). In line, patients with disrupted plaque surface on CTA at baseline had a larger median baseline IPH volume than patients with smooth plaque surface (25.1 mm3, IQR: [0.0-166.2 mm3] vs. 0.0 mm3; p<0.05). In the TRFC and disrupted plaque surface groups, the median IPH volume tended to decrease during follow-up (baseline: 97.3 mm3 versus follow-up: 29.7 mm3, p=0.09, and baseline: 25.1 mm3 versus follow-up: 11.2 mm3, p=0.04, respectively) (Figure 2). On the other hand, in the group with a thick fibrous cap and the group with a smooth plaque surface, the median IPH volumes were zero at baseline and remained zero at follow-up (Figure 2). The risk of IPH progression was higher in the TRFC/disrupted plaque groups (risk ratio (RR): 2.9, 95% CI: 1.5-5.5 and 2.0, CI: 0.9-4.5, respectively) than in patients with a thick fibrous cap/smooth plaque surface (Table 1). An example of IPH progression is shown in Figure 3. Additionally, patients with a TRFC were at increased risk of having IPH at follow-up (OR=6.3, 95% CI: 2.4-16.9; p<0.05), while patients with disrupted plaque surface did not show this increased risk (OR=1.8, 95% CI: 0.6-4.8; p=0.3). An explorative analysis showed that in most patients, fibrous cap status and plaque surface morphology did not change from baseline to follow-up (Figure 4). Patients with a TRFC or disrupted plaque surface at both time points had the largest median IPH volume at baseline and follow-up. During follow-up, a net nonsignificant decrease in IPH volume was observed in these patients. Patients with a thick FC or smooth plaque surface at both time points had the lowest IPH volume at both time points. In patients with a thick fibrous cap changing to TRFC or a smooth plaque surface changing to disrupted, there was an increase in IPH volume (Figure 4). The opposite trend, i.e. a decrease in IPH volume, was observed in patients where TRFC changed to thick or the disrupted plaque surface changed to smooth.Discussion
For stroke patients with a TRFC/disrupted plaque, with a larger median baseline IPH volume, the net decrease in IPH volume may indicate plaque healing over time. Nevertheless, patients with a TRFC/disrupted plaque are still at increased risk for IPH progression.Conclusion
Symptomatic patients with TRFC/disrupted plaque surface are at increased risk of IPH progression and may benefit from regular monitoring.Acknowledgements
All members of the PARISK study group: S.L.M. Bakker, H. Boersma, D. Bos, G.A.J.C. Crombag, M.J.A.P. Daemen, G.J. de Borst, M.P.M. de Maat, A.A.J. de Rotte, K. Dilba, J. Hendrikse, A.P. Hoeks, P.A.M. Hofman, B. Hussain, L.J. Kapelle, M. Kassem, M.E. Kooi, A.G. Korten, P.J. Koudstaal, J.R. de Kruijk, N.D. Kruyt, M.I. Liem, M. Limburg, C. Lucci, B.J. Meems, W.H. Mess, M.T. Mulder, P.J. Nederkoorn, A.J. Nederveen, K.P.H. Nies, R. Saxena, F.H.B.M. Schreuder, A.H.C.M.L. Schreuder, J.P.L. Slenders, H.M. Spronk, J. Steinbuch, H. ten Cate, S.C. Tromp, M.T.B. Truijman, H.M.M. van Beusekom, D.H.K. van Dam‐Nolen, A.G. van der Kolk, A. van der Lugt, A.C. van Dijk, A.F.W. van der Steen, A.M. van Hattem, R.H.M. van Hoof, R.J. van Oostenbrugge, N.P. van Orshoven, T.J. van Velzen, J.C.B. Verhey, W. Weisfelt, J.E. Wildberger, A.D. Wijnhoud, T. Zadi.References
1. Gupta A, Baradaran H, Schweitzer AD, Kamel H, Pandya A, Delgado D, et al. Carotid Plaque Mri and Stroke Risk: A Systematic Review and Meta-Analysis. Stroke (2013) 44(11):3071-7. Epub 2013/08/31. doi: 10.1161/strokeaha.113.002551.
2. Schindler A, Schinner R, Altaf N, Hosseini AA, Simpson RJ, Esposito-Bauer L, et al. Prediction of Stroke Risk by Detection of Hemorrhage in Carotid Plaques: Meta-Analysis of Individual Patient Data. JACC Cardiovasc Imaging (2020) 13(2 Pt 1):395-406. doi: 10.1016/j.jcmg.2019.03.028.
3. Ota H, Yu W, Underhill HR, Oikawa M, Dong L, Zhao X, et al. Hemorrhage and Large Lipid-Rich Necrotic Cores Are Independently Associated with Thin or Ruptured Fibrous Caps: An in Vivo 3t Mri Study. Arteriosclerosis, thrombosis, and vascular biology (2009) 29(10):1696-701. Epub 07/16. doi: 10.1161/ATVBAHA.109.192179.
4. Dam-Nolen DHKv, Truijman MTB, Kolk AGvd, Liem MI, Schreuder FHBM, Boersma E, et al. Carotid Plaque Characteristics Predict Recurrent Ischemic Stroke and Tia. JACC: Cardiovascular Imaging 0(0). doi: doi:10.1016/j.jcmg.2022.04.003.
5. Truijman MT, Kooi ME, van Dijk AC, de Rotte AA, van der Kolk AG, Liem MI, et al. Plaque at Risk (Parisk): Prospective Multicenter Study to Improve Diagnosis of High-Risk Carotid Plaques. International journal of stroke : official journal of the International Stroke Society (2014) 9(6):747-54. Epub 2013/10/22. doi: 10.1111/ijs.12167.
6. Bland JM, Altman DG. Measuring Agreement in Method Comparison Studies. Statistical Methods in Medical Research (1999) 8(2):135-60. doi: 10.1177/096228029900800204.
Figures
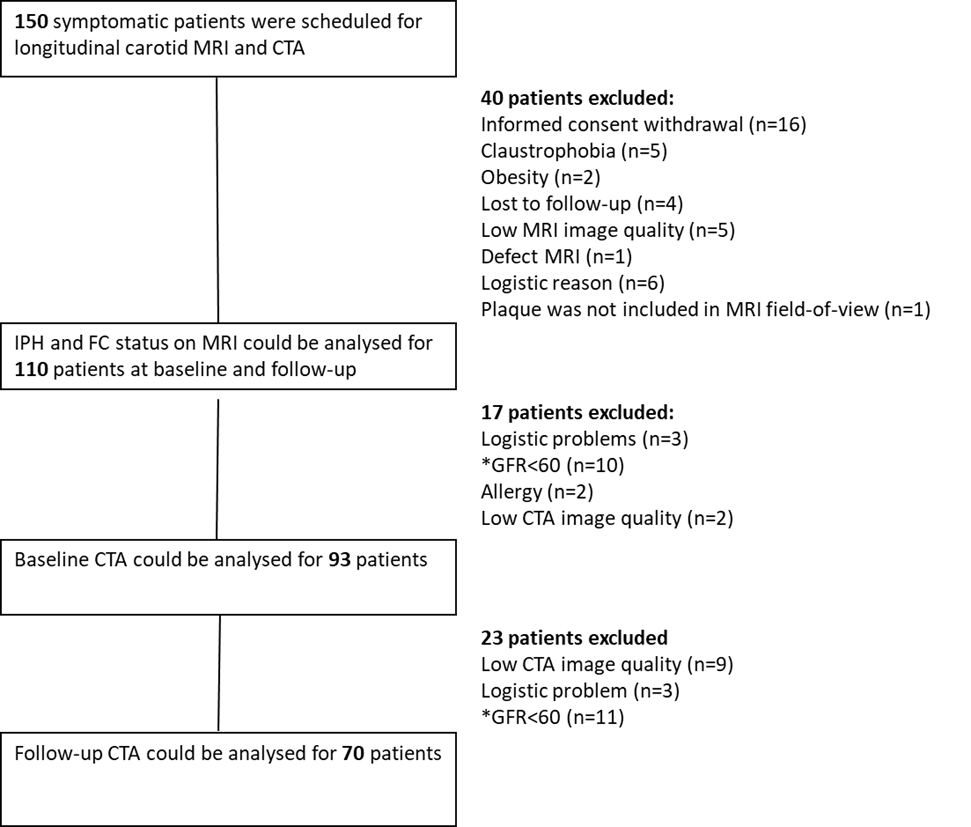
Figure 1. Flow chart of the study
MRI= magnetic resonance imaging, CTA= computed tomographic angiography, GFR= glomerular filtration rate, IPH= intraplaque hemorrhage, FC = fibrous cap, *= based on exclusion criteria in the ethical protocol.
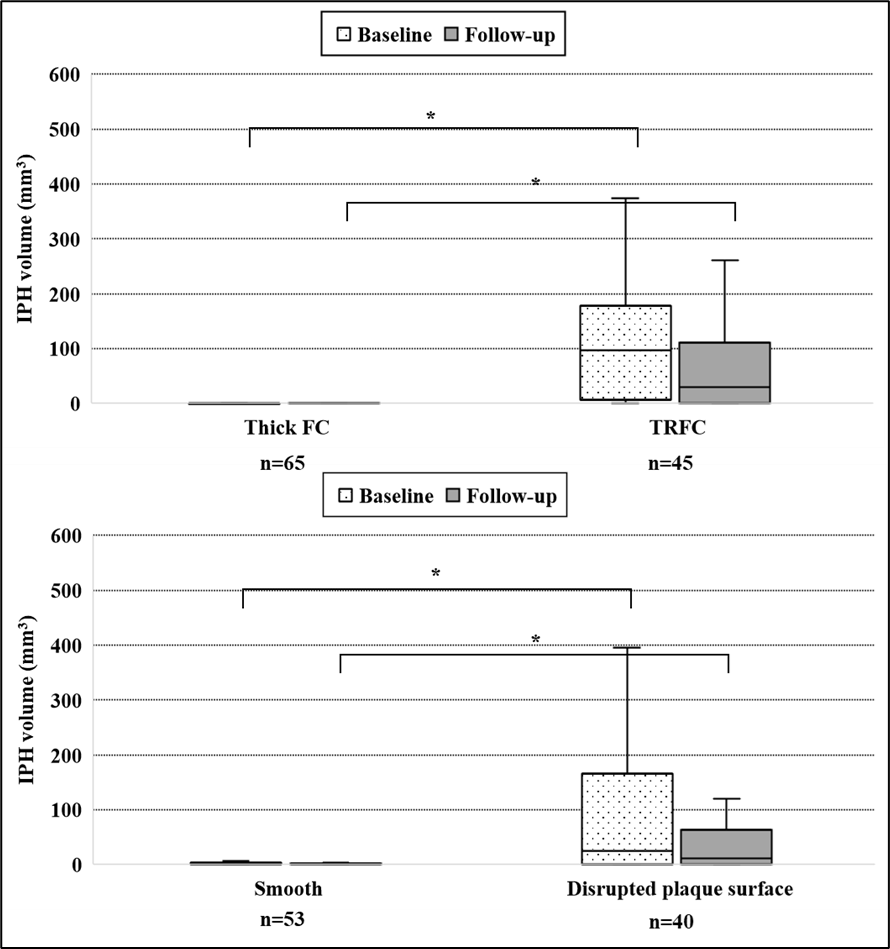
Figure 2. Median intraplaque volume at baseline and at two-year follow-up
IPH indicates intraplaque hemorrhage; FC indicates fibrous cap; TRFC indicates thin or ruptured fibrous cap.
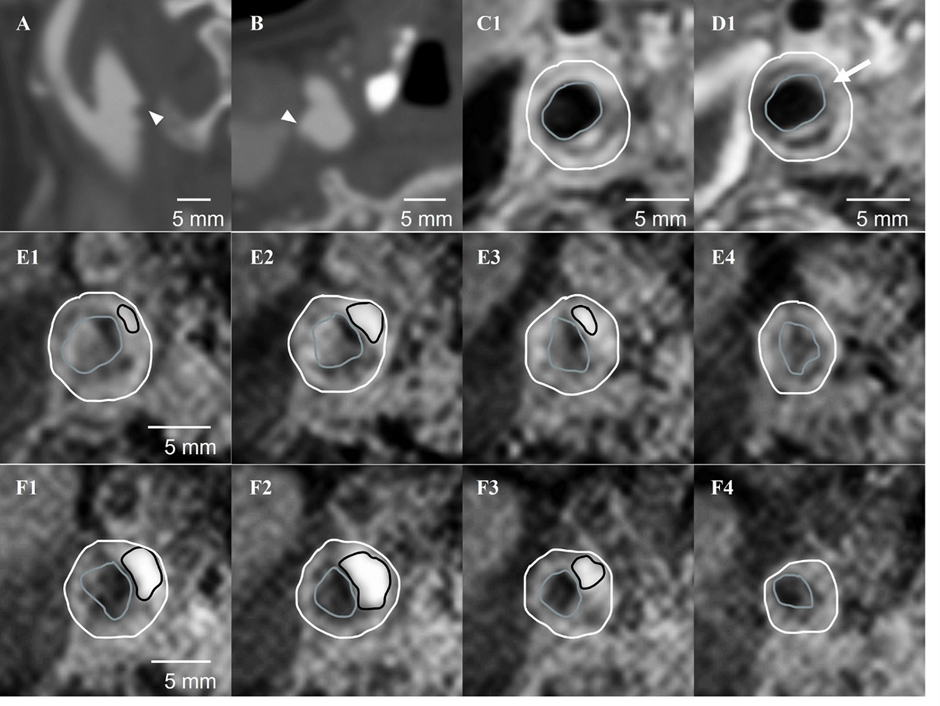
Figure 3. The arrowhead indicates a disrupted plaque surface on baseline CTA images (A, B). The arrow indicates a thin or ruptured fibrous cap (TRFC) on baseline pre and post-contrast T1w MRI. The gray and white contours indicate the lumen and outer vessel wall delineation. E1-4) and F1-4) show consecutive 3D T1-weighted inversion recovery turbo field echo (IR-TFE) images of a patient with IPH at baseline and follow-up, respectively. The black contours indicate the delineations of intraplaque hemorrhage (IPH)). The total IPH volume increased by 62% after two years of follow-up.
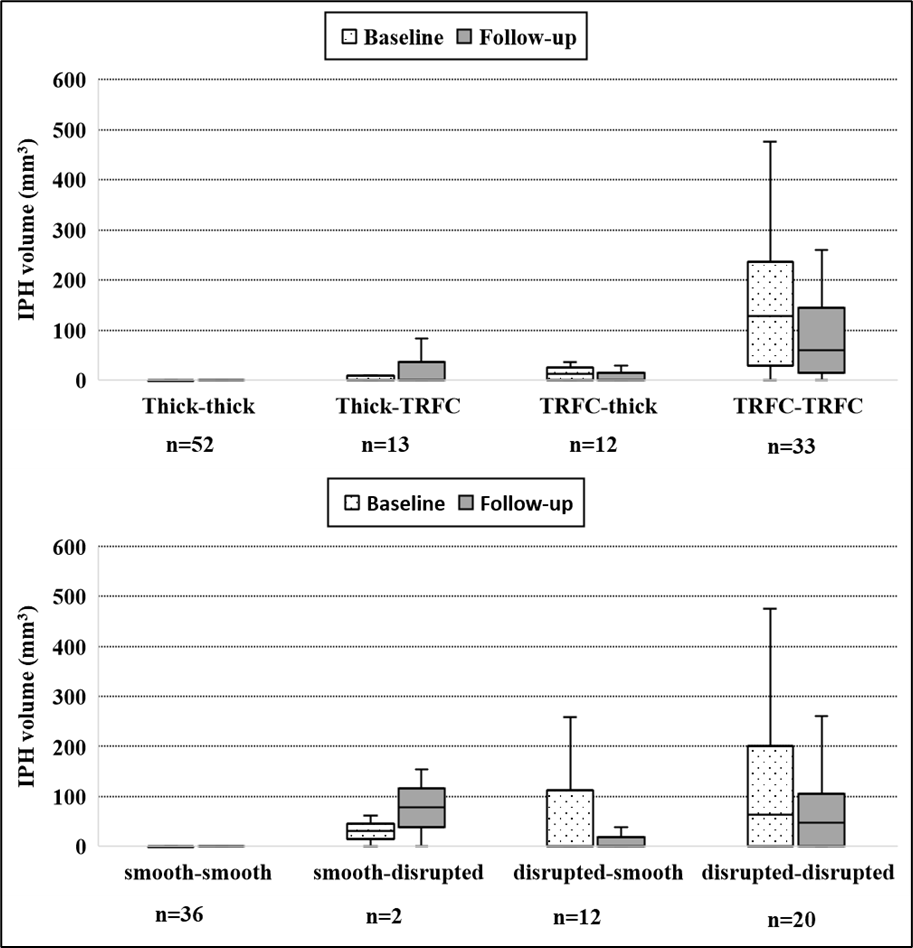
Figure 4. Explorative analysis on the median IPH volumes stratified by fibrous cap status (thick versus TRFC) or plaque surface morphology (smooth versus disrupted) at baseline and follow-up.
For instance, thick-TRFC indicates a thick fibrous cap at baseline and a TRFC at follow-up. TRFC indicates thin or ruptured fibrous cap; IPH indicates intraplaque hemorrhage.
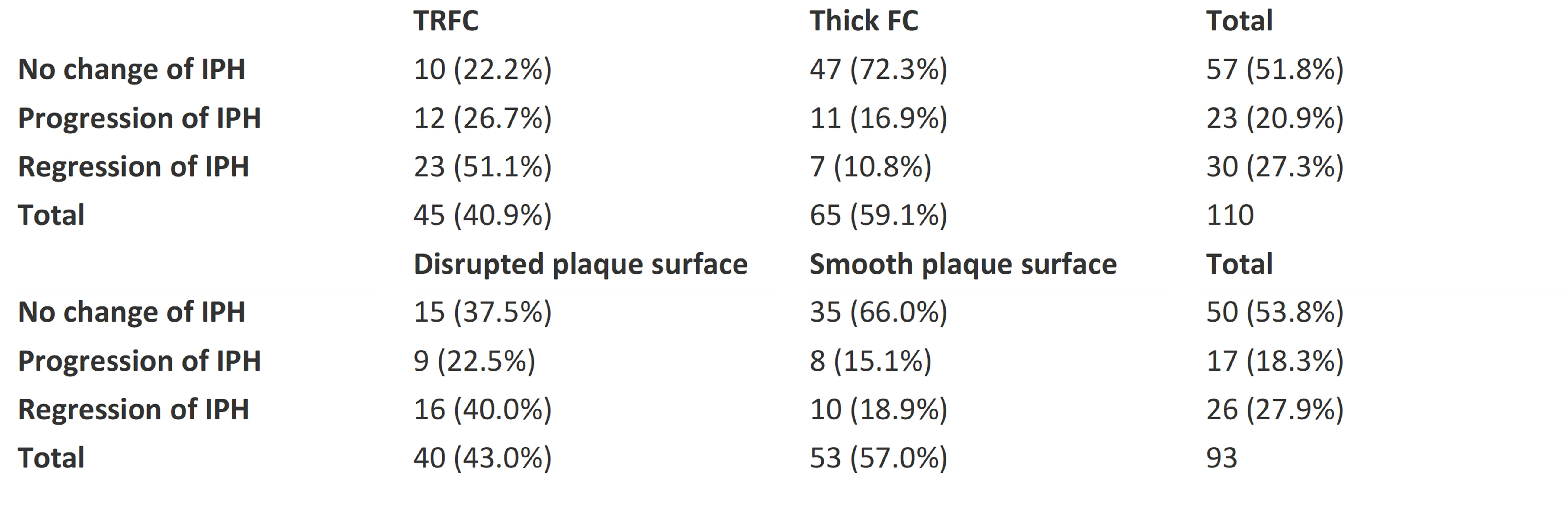
Table 1. IPH volume change during two years of follow-up
Progression of IPH= volumetric increase compared to the baseline value larger than 22% or new IPH. Regression= volume decrease of more than 22% or disappearance of IPH. A change between -22% and +22% was classified as no change in IPH volume.