3384
The Value of Multimodal Atherosclerotic Plaque Imaging Coordinated Analysis in the Assessment of Cardiovascular and Cerebrovascular Events1Radiology department, Fujian Provincial Hospital, Fuzhou, China, 2Shengli Clinical Medical College of Fujian Medical University, Fuzhou, China, 3Department of Geriatric Medicine, Fujian Provincial Hospital, Fuzhou, China, 4MR Research Collaboration Team, Siemens Healthineers Ltd., Shanghai, China
Synopsis
Keywords: Vessel Wall, Atherosclerosis, intracranial artery, stroke, coronary artery
Motivation: The coexistence of atherosclerosis in coronary, and intracranial arteries has not been comprehensively assessed.
Goal(s): This study was designed to investigate the co-existence of atherosclerosis in the intracranial and coronary arteries of patients with and without ASCVD using high-resolution magnetic resonance imaging and computed tomography angiography.
Approach: The ASCVD group exhibited greater artery stenosis, as well as significant differences in lipid, calcium volumes, and lipid volume ratio compared to the non-event group. Additionally, different plaque types displayed significant variations in morphology and composition.
Results: There is a consistent pattern of change in plaque characteristics between intracranial and coronary arteries.
Impact: High-resolution magnetitic resonance imaging (hrMRI) and coronary computed tomography angiography (CCTA) to investigate the co-existence of high-risk atherosclerotic plaques in the intracranial and coronary arteries of patients with cardiovascular events. Results showed that such plaques were present in both locations.
Introduction
Despite significant improvements in prevention, diagnosis, and treatment in recent decades, atherosclerotic cardiovascular disease (ASCVD), mainly stroke and heart attack, remains the leading cause of death and disability worldwide1-2. Currently, angiography-defined luminal stenosis is the only validated criterion for risk assessment, including digital subtraction angiography (DSA), magnetic resonance angiography (MRA), and computed tomography angiography (CTA)3. However, serious limitations exist4. Increasing evidence has shown that detailed lesion morphological and compositional features are more relevant to patient clinical presentations and subsequent events5-7. Advanced high-resolution multi-contrast MRI (hrMRI) has enabled characterization of detailed architectures in atherosclerosis noninvasively. This study was designed to explore the coexistence and differences of lesion architecture in the atherosclerosis in the intracranial and coronary territories in patients with and without ASCVD using hrMRI and CTA.Method
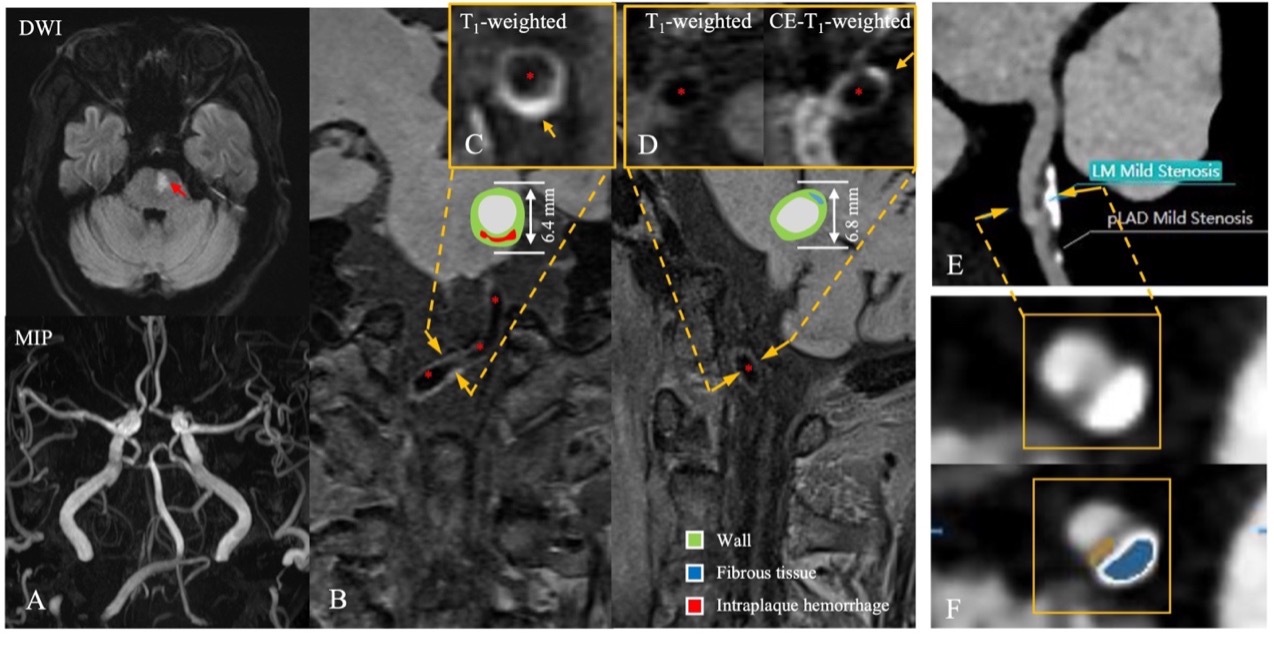
Forty-four patients (age 66 ± 9 years, 28 men) underwent both hrMRI and CCTA were included. The ASCVD group was defined as patients who had a cardiac or/and cerebral ischemic event. The non-event group included patients with atherosclerotic plaques in the head and neck arteries and coronary arteries, but without any ischemic cardiovascular event. In hrMRI, if there was only one lesion on the ipsilateral side of ischemia, it was considered as the culprit, and if multiple plaques were present on the ipsilateral side, the most stenotic one was considered as the culprit8. In CCTA, culprit lesions associated with cardiac ischemic events were identified based on findings on electrocardiography, wall motion abnormalities on echocardiography, or angiographic appearance during invasive coronary angiography9-10. Other lesions, if present, were treated as non-culprits. All MR images were obtained in a 3T scanner (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany) with a 64-channel head-and-neck coil. The brain imaging protocol included diffusion-weighted imaging (DWI), T1-weighted and T2-weighted imaging, and T2 fluid-attenuated inversion recovery (FLAIR). The hrMRI protocol included 3D time-of-flight magnetic resonance angiography (MRA) (TR 900 ms, TE 16 ms, FOV 238 mm × 169 mm, Matrix 317 × 384, slice thickness 5 mm, slice interval 1.5 mm, layer number 336, turbo factor 52, acquisition factor 2, scanning time 8 min 42 s), 3D black blood T1-weighted Sampling Perfection with Application optimized Contrast using different flip angle Evolution (SPACE) sequence (3D T1) (TR 900 ms, TE 16 ms, FOV 238 mm × 169 mm, Matrix 318 × 448, slice thickness 0.53 mm, layer number 240, turbo factor 52, acquisition factor 2, scanning time 8 min 06 s), 3D black blood T2-weighted SPACE sequence (3D T2) (TR 1200 ms, TE 122 ms, FOV 180 mm × 180 mm, Matrix 248 × 256, slice thickness 0.7 mm, layer number 72, turbo factor 56, acquisition factor 2, scanning time 5 min 07 s) and postcontrast 3D black blood T1-weighted SPACE sequence (3D CE-T1) (parameters were same as 3D T1). CCTA was performed using a third-generation dual-source CT (SOMATOM Force, Siemens Healthcare, Erlangen, Germany). All hrMRI images were independently analyzed by two neuroradiologists using MR-VascularView to quantify plaque morphological and compositional features (Fig. 1). CCTA images were analyzed independently by another two independent radiologists using coronary-specific analysis software (CoronaryDoc) (Fig. 1). Student's t-test or Wilcoxon rank-sum test was used where appropriate to compare continuous parameters between two groups and χ2 test for categorical data.Results
In intracranial plaques, compared to the non-event group, the ASCVD group had more severe stenosis grades and statistically significant differences in lipid plaque volume (LPV), lipid plaque volume ratio (LPR), and calcified plaque volume (CPV). Similarly, in coronary plaques, the ASCVD group had plaques with greater stenosis, more severe stenosis grades, larger volumes, longer length, larger fibro-lipid plaque volume (FLPV), larger fibrotic plaque volume (FPV), and higher fibrotic plaque volume ratio (FPR) compared to the non-event group. Furthermore, there were statistically significant differences in stenosis, stenosis grades, plaque length, and plaque volume between non-event plaque, non-culprit plaque, and culprit plaque. Finally, in image analysis of hrMRI, there were differences between intraplaque hemorrhage volume ratio (IPHR), LPR, FPV, and CPV among the three groups of plaques, and FLPV and FPV were significantly different among the three different plaque types from coronary artery.Discussion & Conclusions
This study conducted an initial exploration into the similarity of characteristics of intracranial and coronary plaques obtained through different imaging within the same patient. Our results indicate that, for the same patient, there is a consistent pattern of change in plaque characteristics between intracranial and coronary arteries.Acknowledgements
Thanks to technician Shengmei Lin, Jiawei Su and nurse Fang Huang who helped in the MR examination; thanks to Fayang Lian who works in the scientific research department of the hospital to provide scientific consultation. Thanks very much to Professor Zhongzhao Teng and his team members for their technical support.References
1 Arnett D K, Blumenthal R S, Albert M A, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines[J]. Circulation, 2019, 140(11): e596-e646.2 Mach F, Baigent C, Catapano A L, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk: the Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)[J]. European heart journal, 2020, 41(1): 111-188.
3 Battistella V, Elkind M. Intracranial atherosclerotic disease[J]. European journal of neurology, 2014, 21(7): 956-962.
4 Rothwell P M, Warlow C P. Prediction of benefit from carotid endar terectomy in individual patients: a risk-modelling study[J]. The Lancet, 1999, 353(9170): 2105-2110.
5 Teng Z, Brown A J, Gillard J H. From ultrasonography to high resolution magnetic resonance imaging: Towards an optimal management strategy for vulnerable carotid atherosclerotic plaques[J]. EBioMedicine, 2016, 3: 2-3.
6 Underhill H R, Hatsukami T S, Fayad Z A, et al. MRI of carotid atherosclerosis: clinical implications and future directions[J]. Nature Reviews Cardiology, 2010, 7(3): 165-173.
7 Stone G W, Maehara A, Lansky A J, et al. A prospective natural-history study of coronary atherosclerosis[J]. New England Journal of Medicine, 2011, 364(3): 226-235.
8 Qiao Y, Zeiler S R, Mirbagheri S, et al. Intracranial plaque enhancement in patients with cerebrovascular events on high-spatial-resolution MR images[J]. Radiology, 2014, 271(2): 534-542.
9 Pflederer T, Marwan M, Schepis T, et al. Characterization of culprit lesions in acute coronary syndromes using coronary dual-source CT angiography[J]. Atherosclerosis, 2010, 211(2): 437-444.
10 Tesche C, Caruso D, De Cecco C N, et al. Coronary computed tomography angiography–derived plaque quantification in patients with acute coronary syndrome[J]. The American journal of cardiology, 2017, 119(5): 712-718.
Figures