3383
Monitoring relative diameter change of the carotid artery using non-contrast-enhanced 4D dynamic angiography: preliminary results1Department of Radiology, Department of Radiology, Lausanne University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 2CIBM Center for BioMedical Imaging, Lausanne, Switzerland, 3IHU LIRYC, Electrophysiology and Heart Modeling Institute, INSERM U1045, Centre de recherche Cardio-Thoracique de Bordeaux, Université de Bordeaux, Bordeaux, France, 4Department of Cardiovascular Imaging, Hôpital Cardiologique du Haut-Lévêque, CHU de Bordeaux, Bordeaux, France, 5Stroke Center, Neurology Service, Department of Clinical Neurosciences, Lausanne University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland
Synopsis
Keywords: Vascular, Blood vessels, Carotid Diameter, Pulsatile Motion, Angiography
Motivation: The carotid artery anatomy is routinely studied with MRI, whilst its relative diameter change is evaluated using ultrasound. An MRI technique to measure the carotid diameter change throughout the cardiac cycle could therefore be complementary to the existing toolset.
Goal(s): To combine carotid MR angiography and diameter change quantification in one scan without contrast agent injection.
Approach: A 4D (3D+time) free-running sequence was extended with slab-selective RF pulses to increase the inflow blood-to-muscle contrast. Carotid diameter changes and contrast ratios were quantified.
Results: The contrast ratio significantly improved with the use of slab-selective pulses and the carotid relative diameter change was precisely measured.
Impact: 4D free-running MR angiography with slab-selective RF pulses allows for the dynamic visualization of the carotid lumen and the quantification of the relative carotid diameter change throughout the cardiac cycle without contrast agent injection.
Introduction
Stroke is one of the leading causes of disability worldwide, and is often related to arteriosclerosis and plaque rupture in the neck.1 Besides clinical symptoms, current carotid plaque treatment decisions are mostly based on the degree of stenosis. Nevertheless, changes in vessel wall stiffness and arterial diameter also appear to be prevalent in the development of cardiovascular disease.2,3 To quantify the degree of atheromatous stenosis in the carotid artery, MR angiography (MRA) is commonly used.4 However, echo tracking ultrasound is routinely employed to track vessel diameter changes during the systolic and diastolic cardiac phases (i.e., the relative diameter change); such a biomarker would be a useful complement to the MRA toolset.5 The objective of this study was therefore to assess the feasibility of 4D dynamic MRA for the quantification of carotid diameter changes throughout the cardiac cycle without the need for contrast agents.In MRA at 3T, GRE sequences are commonly used due to their low susceptibility to magnetic field inhomogeneities. However, GRE images lack contrast between the blood and the surrounding structures. As alternatives, contrast agents or sequences such as time-of-flight (TOF) are frequently used. In this study, we therefore combined a 4D free-running6 sequence with slab-selective RF excitation to generate inflow contrast.
Methods
Ten healthy volunteers (2F, 33±9y) were scanned on a 3T clinical scanner (MAGNETOM PrismaFit, Siemens Healthineers, Erlangen, Germany) with 4 sequences. 1) A free-running GRE sequence (isotropic pixel size=0.6mm3, field of view=160mm3, RF excitation angle α=8º, scan time=8min) using a 3D radial phyllotaxis trajectory7 (Figure 1A). For contrast generation, slab-selective sinc RF pulses8 were used in the axial orientation to excite 60% of the field of view. 2) Same as the first, but with non-selective RF pulses (scan time=9min). 3) A 2D breath-hold cine sequence (temporal resolution=40ms, pixel size=1.17x1.17x6mm3, 4 slices). 4) A routine (non-dynamic) TOF sequence (pixel size=0.4x0.4x0.45mm3, 295 slices, scan time=4min, α=20º) in a 6-volunteer subset.Pulse oximetry was used to retrospectively sort the free-running k-space data into cardiac-motion-resolved bins of 80ms duration (Figure 1A). 4D (3D+cardiac cycle) datasets were reconstructed using compressed sensing9 and denoised with HD-PROST.10
The effect of the slab-selective RF pulses (Figure 1B) was assessed by calculating the blood-to-muscle contrast ratio (CR) between the carotid lumen and sternocleidomastoid muscle signals S for non-selective (NS) and slab-selective (SS) acquisitions: CR=[Sblood-Smuscle]/Smuscle. The CR of the slab-selective sequence and TOF were also compared.
The left and right common carotid diameter was measured on four transversal 2D cine slices and on matching reformatted slab-selective images to compute the changes from the diastolic (DD) to the systolic (SD) phases (Figure 1C), as well as the relative diameter change (RDC=[SD-DD]/DD). Differences were assessed with two-sided paired t-tests and p<0.05 was considered statistically significant.
Results
The average CR improved significantly when applying slab-selective (CRSS=1.74±0.41) instead of non-selective RF pulses (CRNS=0.41±0.16, p<0.0001, Figure 2A). In its subgroup, the CR for the TOF (CRTOF=4.24±0.94) was still higher though (CRSS=1.70±0.52, p=0.0009, Figure 2B).The average DD was lower in the slab-selective (DDSS=5.87±0.70mm) than in the 2D cine images (DDCINE=6.16±0.35mm, p=0.0001, Figures 3A, Figure 5). No significant differences were observed for the SD. The relative diameter change (RDC) was significantly higher in the slab-selective (RDCSS=18.25±2.23%) than in the cine images (RDCCINE=8.24±4.66%, p<0.0001, Figure 3B).
Discussion
The dynamic free-running carotid MRA with slab-selective RF pulses was successfully acquired in all participants, and could be used to assess the diameter differences between the diastolic and systolic phases.The underestimation of the slab-selective DD caused a significant increase in the RDC compared to cine images, which better agree with literature.3,11 This might be explained by flow artifacts or variable inflow velocity. The lower contrast in the SS compared to the TOF images is likely related to the thinner slab and higher RF excitation angle of the latter.
Besides carotid pulsation, swallowing and respiration are also confounders in carotid MRA.12 These motion sources might affect the estimation of the diameters due to unaccounted vessel displacements. Future work will therefore focus on accounting for respiratory motion using a motion-resolved approach, 13 validating the findings versus the reference standard echo tracking ultrasound, and correlating the sequence in patients with different degrees of carotid arteriosclerotic plaque.
Conclusion
We demonstrated the feasibility of characterizing the carotid anatomy and its pulsatile diameter change using free-running 4D dynamic MRA with slab-selective RF pulses.Acknowledgements
This study was funded by grants from the Swiss Heart Foundation and the Swiss National Science Foundation (grant number 32003B_182615).References
1. Donkor, E. S. Stroke in the 21st Century: A Snapshot of the Burden, Epidemiology, and Quality of Life. Stroke Res Treat, (2018). doi:10.1155/2018/3238165
2. Sedaghat S. et al. Common Carotid Artery Diameter and Risk of Cardiovascular Events and Mortality Pooled Analyses of Four Cohort Studies. Hypertension 72, 85–92 (2018). doi:10.1161/HYPERTENSIONAHA.118.11253
3. Cuadrado Godia, E. et al. Carotid Artery Distensibility: A Reliability Study. J Ultrasound Med. 9, 1157–1165 (2007). doi:10.7863/jum.2007.26.9.1157
4. Nederkoorn, P. J. et al. Time-of-Flight MR Angiography of Carotid Artery Stenosis: Does a Flow Void Represent Severe Stenosis? American Journal of Neuroradiology 23, 1779–1784 (2002).
5. Kojo, M. et al. Normal Developmental Changes in Carotid Artery Diameter Measured by Echo-Tracking. Pediatr Neurol 18, 221–226 (1998). doi: 10.1016/s0887-8994(97)00195-1
6. Coppo, S. et al. Free-running 4D whole-heart self-navigated golden angle MRI: Initial results. Magn Reson Med 74, 1306–1316 (2015). doi:10.1002/mrm.25523
7. Piccini, D. et al. Spiral phyllotaxis: The natural way to construct a 3D radial trajectory in MRI. Magn Reson Med 66, 1049–1056 (2011). doi:10.1002/mrm.22898
8. Ferincz, R. et al. Slab-selection in free-running cardiac and respiratory motion-resolved bSSFP 5D whole-heart MRI. ISMRM 3095 (2023).
9. Lustig, M. et al. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magn Reson Med 58, 1182–1195 (2007). doi:10.1002/mrm.21391
10. Bustin, A. et al. High-dimensionality undersampled patch-based reconstruction (HD-PROST) for accelerated multi-contrast MRI. Magn Reson Med 81, 3705–3719 (2019). doi:10.1002/mrm.27694
11. Hansen, F. et al. Diameter and compliance in the human common carotid artery-variations with age and sex. Pergamon Ultrasound in Med. & Biol 21, 1-9 (1995). doi:10.1016/0301-5629(94)00090-5
12. Boussel, L. et al. Swallowing, arterial pulsation, and breathing induce motion artifacts in carotid artery MRI. Journal of Magnetic Resonance Imaging 23, 413–415 (2006). doi:10.1002/jmri.20525
13. Feng, L. et al. 5D whole-heart sparse MRI. Magn Reson Med 79, 826–838 (2018). doi:10.1002/mrm.26745
Figures
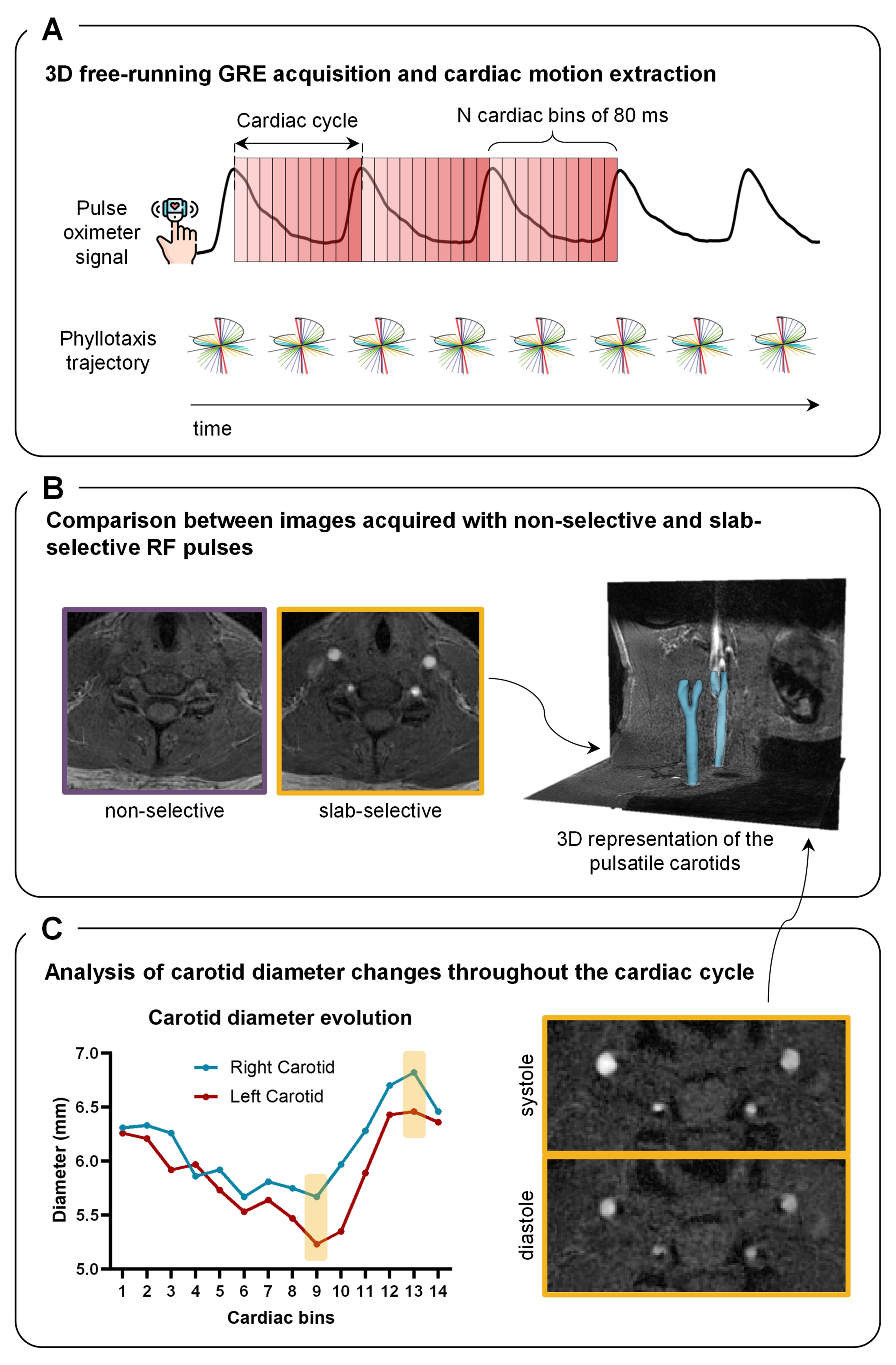
Figure 1. Overview of the free-running framework. (A) Continuous acquisition of data using a segmented 3D radial trajectory and k-space cardiac binning into N bins of 80 ms using the pulse oximeter signal. (B) Comparison of blood-to-muscle contrast between images obtained with non-selective and slab-selective RF pulses. (C) Example measurement of the carotid diameter in a healthy volunteer to quantify the relative diameter change throughout the cardiac cycle.
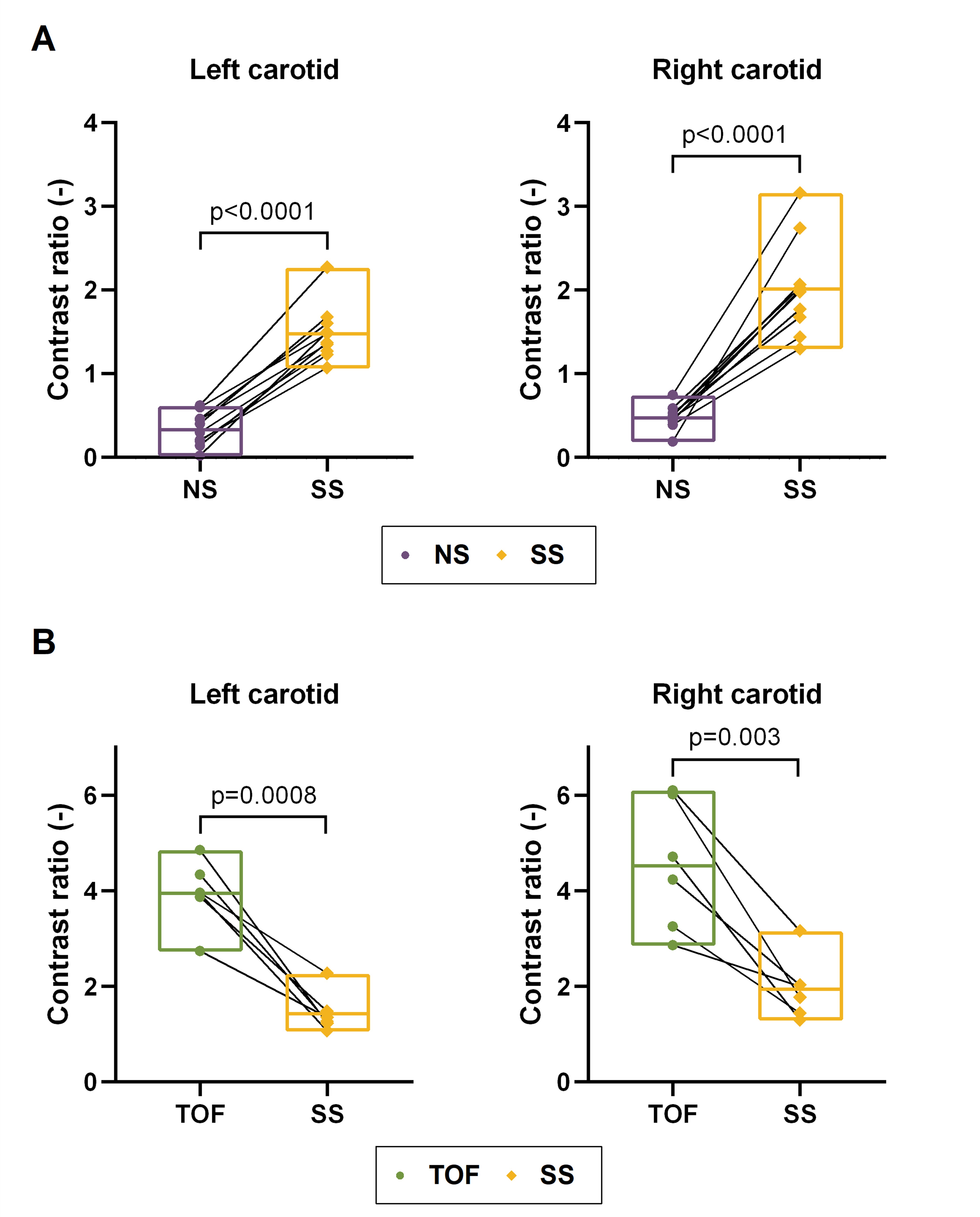
Figure 2. Blood-to-muscle contrast ratio for both carotids. (A) Contrast ratio between non-selective (NS) and slab-selective (SS) acquisition. The contrast ratio significantly increased for the slab-selective case (pleft<0.0001 and pright<0.0001). (B) Contrast ratio between the clinical TOF acquisition and the SS images in a subset of 6 volunteers. The thin TOF slices resulted in higher contrast ratios (pleft=0.0008 and pright=0.003).
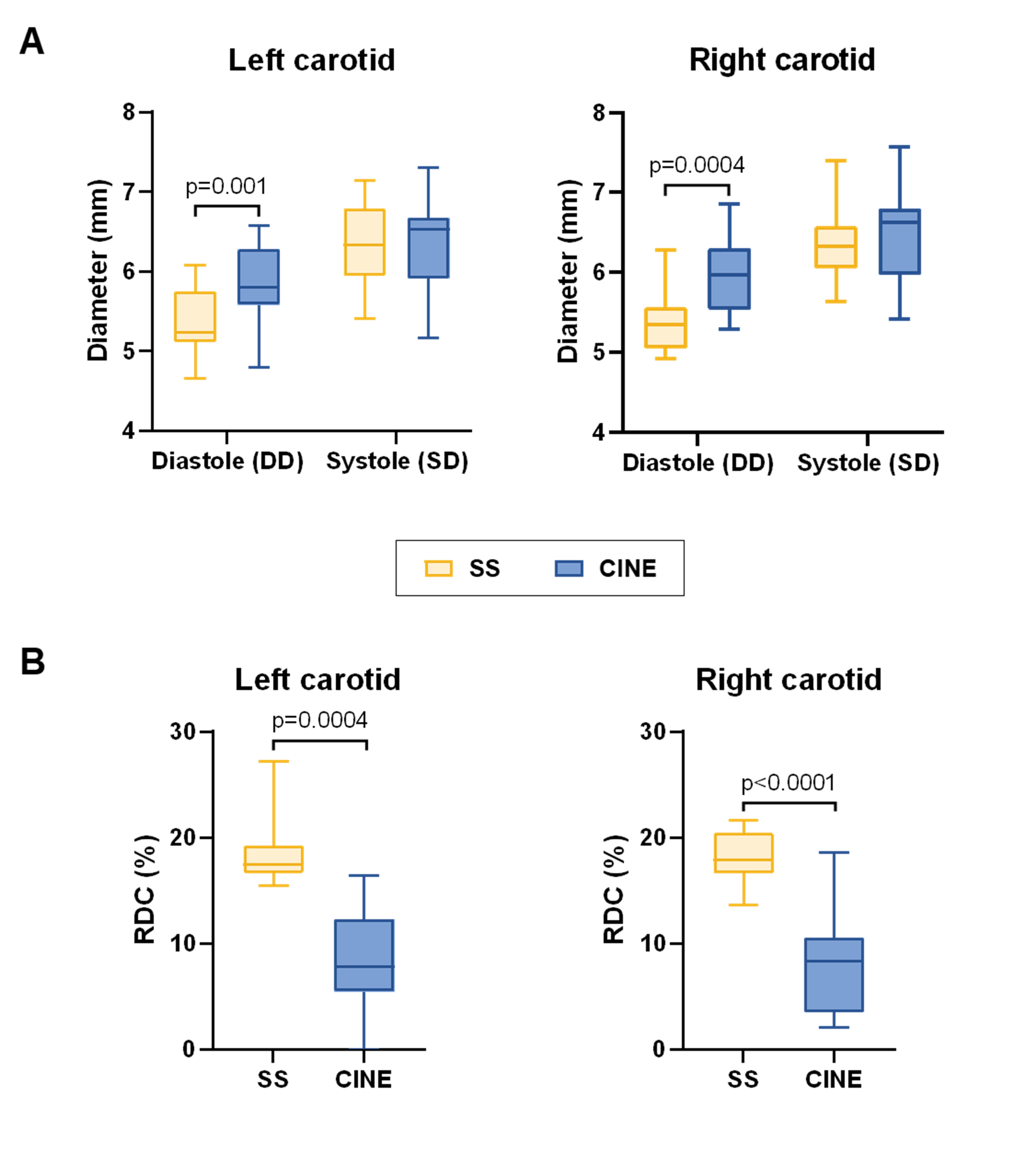
Figure 3. Diastolic and systolic diameter measurements for both carotids. (A) Diameter measurements in the slab-selective (SS) and cine acquisitions. There is a slight but consistent underestimation of the diameter in both phases in the SS images, which is statistically significant in the diastolic phase (pleft=0.001 and pright=0.0004). (B) Relative diameter change (RDC) in the SS and cine acquisitions. A significant overestimation can be observed in the SS case (pleft=0.0004 and pright<0.0001).
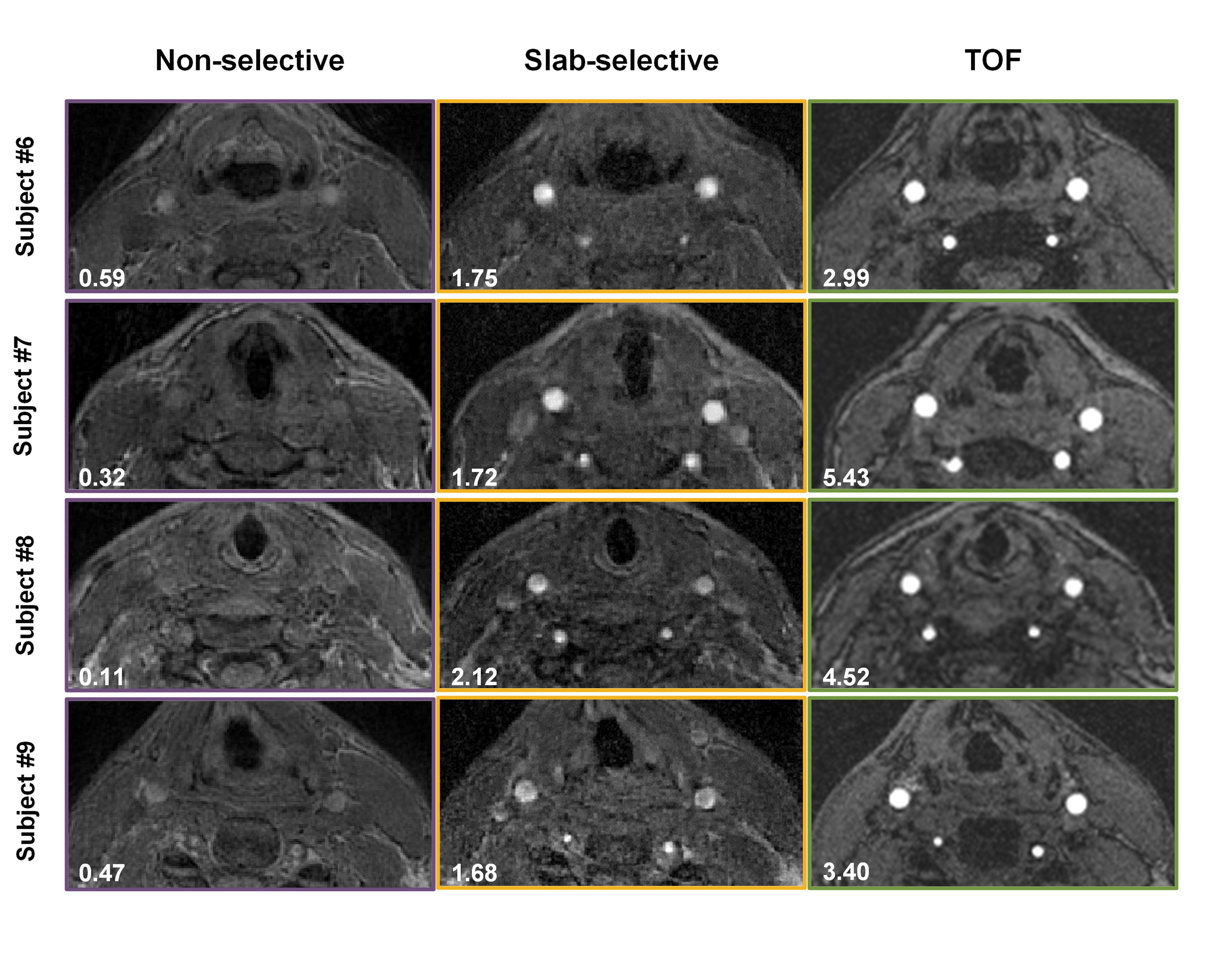
Figure 4. Axial comparison of the carotid arteries. In the lower-left corners, the average contrast ratio of both arteries is displayed. A difference in contrast between TOF and slab-selective images in the systolic phase can be observed but not as pronounced as between the non-selective and slab-selective acquisitions.
Figure 5. Animated 3D representation of the pulsating carotid in subject #1.