3380
Analysis of postural effect on cardiac function using multiposture MRI1Kanazawa University, Kanazawa, Japan, 2Ogaki Municipal Hospital, Ogaki, Japan, 3Ishikawa Prefectural Central Hospital, Kanazawa, Japan
Synopsis
Keywords: Myocardium, Heart, Cardiac function, Cine MRI, Multiposture MRI
Motivation: Cardiac function is affected by body posture. However, MRI measurements have been limited to the supine posture.
Goal(s): Our goal was to evaluate the effect of body posture on cardiac function using multiposture MRI.
Approach: We assessed cardiac function in supine and standing postures in seven healthy males using a 0.4T multiposture MRI.
Results: Significant reductions in left ventricular end-diastolic volume, end-systolic volume, and stroke volume were observed in the standing posture, with increased heart rate, while cardiac output and ejection fraction remained consistent across postures.
Impact: Multiposture MRI enables the assessment of the postural effect on cardiac function and potentially provides new diagnostic insights into regulatory response to postural change.
INTRODUCTION
Cardiac cine MRI and ultrasound (US) are used to evaluate cardiac function and diagnose heart diseases. Some studies using US have shown that body posture affects cardiac function measurements.1,2 However, US has limitations in analytical accuracy. Although cine MRI can assess cardiac function with higher accuracy than US,3 measurements in different body postures, such as standing or sitting, have been limited by the architecture of conventional MRI systems. In this study, we evaluated the effect of body posture on cardiac function using a multiposture MRI, which enables acquisition in various body postures.4METHODS
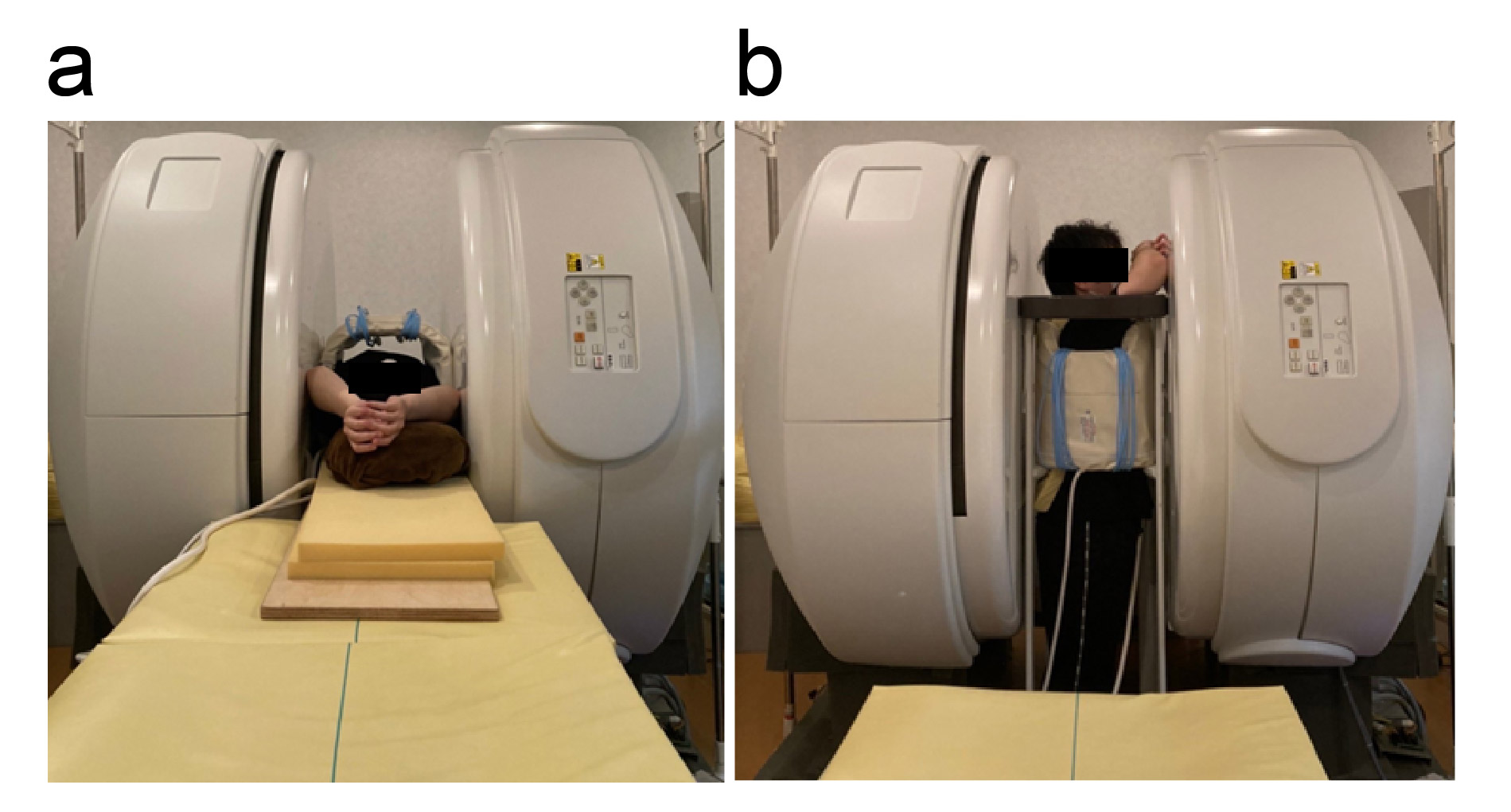
Cardiac function was assessed in seven healthy male subjects (mean age, 22.6 ± 0.5 years) in the supine and standing postures using a 0.4T multiposture MRI (FUJIFILM Healthcare, Tokyo, Japan) (Figure 1). Electrocardiogram-synchronized cardiac cine MRI in the short axis of the left ventricle was performed using a balanced steady-state free precession sequence. The left ventricular cavity in each image was automatically delineated using QIR-MR software (CASIS, Quetigny, France).5 Then, left ventricular end-diastolic volume (EDV), end-systolic volume (ESV), stroke volume (SV), heart rate (HR), cardiac output (CO), and ejection fraction (EF) were determined. We compared the cardiac functional parameters between the two postures using the Wilcoxon signed-rank test. Statistical significance was set at P < 0.05.RESULTS AND DISCUSSION
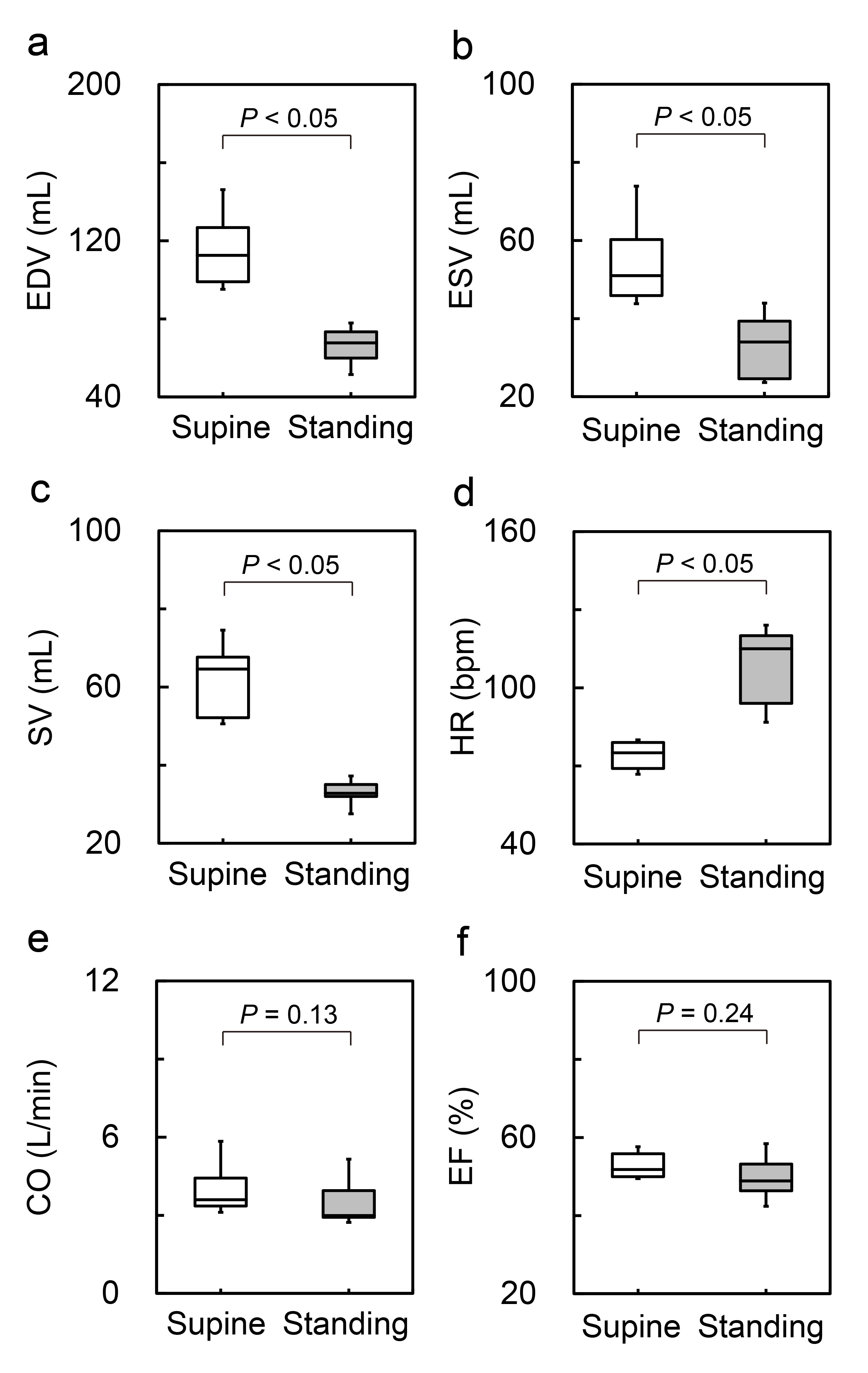
The cardiac functional parameters in the supine and standing postures were 118.4 ± 24.8 mL vs. 65.7 ± 11.8 mL for EDV, 55.9 ± 14.6 mL vs. 33.4 ± 9.4 mL for ESV, 62.5 ± 11.3 mL vs. 32.4 ± 5.1 mL for SV, 73.7 ± 5.6 bpm vs. 108.3 ± 16.1 bpm for HR, 4.1 ± 1.3 L/min vs. 3.6 ± 1.2 L/min for CO, and 53.1 ± 3.7% vs 49.8 ± 6.6% for EF (Figure 2). The EDV, ESV, and SV were significantly smaller in the standing posture than in the supine posture (Figs. 2a–c). These results can be attributed to the fluid shift to the lower part of the body when standing, reducing the venous return of blood to the heart.6 The HR significantly increased in the standing posture compared with the supine posture (Fig. 2d), while the CO showed no significant difference between the postures (Fig. 2e). These findings suggest that increased sympathetic nervous activity in the standing posture leads to elevated HR,7 which maintains a steady CO. No significant difference was observed in the EF between the postures (Fig. 2f), indicating that EF is less affected by posture.CONCLUSION
Standing posture decreases EDV, ESV, and SV and increases HR compared with supine posture. Multiposture MRI enables the assessment of postural effect on cardiac function.Acknowledgements
No acknowledgement found.References
- Baldi JC, et al. Postural differences in hemodynamics and diastolic function in healthy older men. Eur J Appl Physiol. 2007; 99: 651-657.
- Nelson MD, et al. Left ventricular systolic and diastolic function during tilt-table positioning and passive heat stress in humans. Am J Physiol Heart Circ Physiol. 2011; 301: H599-608.
- Walsh TF, et al. Assessment of ventricular function with cardiovascular magnetic resonance. Cardiol Clin. 2007; 25: 15-33, v.
- Kadoya Y, et al. Effect of gravity on portal venous flow: Evaluation using multiposture MRI. J Magn Reson Imaging. 2019; 50: 83-87.
- Painchaud N, et al. Cardiac Segmentation With Strong Anatomical Guarantees. IEEE Trans Med Imaging. 2020; 39: 3703-3713.
- Poliner LR, et al. Left ventricular performance in normal subjects: a comparison of the responses to exercise in the upright and supine positions. Circulation. 1980; 62: 528-534.
- Patel K, et al. Effect of postural changes on cardiovascular parameters across gender. Medicine. 2016; 95: e4149.
Figures