3379
An Open-source, Flexible, Plug-and-Play Inline CMR Image Segmentation Platform1Cardiology, Beth Israel Deaconess Medical Center, Boston, MA, United States, 2Cardiovascular MR R&D, Siemens Healthcare Ltd, Calgary, AB, Canada, 3Siemens Medical Solutions, Boston, MA, United States, 4Medis Medical Imaging Systems, Leiden, Netherlands, 5Radiology, Beth Israel Deaconess Medical Center, Boston, MA, United States
Synopsis
Keywords: Heart Failure, Segmentation, Open-Source
Motivation: Cardiac magnetic resonance (CMR) image segmentation remains a time-consuming task. Deep learning (DL) segmentation models have advanced considerably in recent years, but they lack flexibility for manual adjustments.
Goal(s): We sought to develop an open-source, flexible plug-and-play inline CMR image segmentation platform.
Approach: We implemented in-house algorithms in a clinical scanner as separate Python modules, allowing new and existing DL models to be integrated into clinical workflow.
Results: We assessed the feasibility of the automated plug-and-play platform for inline cine segmentation in 308 patients referred for clinical CMR.
Impact: This platform facilitates the rapid development and evaluation of any segmentation algorithm in a transparent and reproducible fashion. An open-source, flexible, plug-and-play inline CMR segmentation platform will enable rapid testing and evaluation of new segmentation and analysis algorithms.
Introduction
In recent years, cardiac magnetic resonance (CMR) imaging has seen increasing clinical use, yet the time-consuming process of manual contour drawing remains a significant challenge in image analysis. Deep learning (DL) models have been proposed for automated contouring, however they lack flexibility for manual adjustments and quality control. Commercial CMR segmentation software increases accessibility, but is often slower to update algorithms and has limited flexibility for research, falling short of meeting the evolving demands for CMR imaging. There is a need for a flexible, integrated platform for CMR segmentation that is adaptable to new models and seamlessly embedded within existing scanning and analysis workflows. We sought to develop and evaluate a platform for a flexible plug-and-play, inline CMR segmentation with results readily available on the scanner and an option for subsequent adjustments in post-processing software.Methods
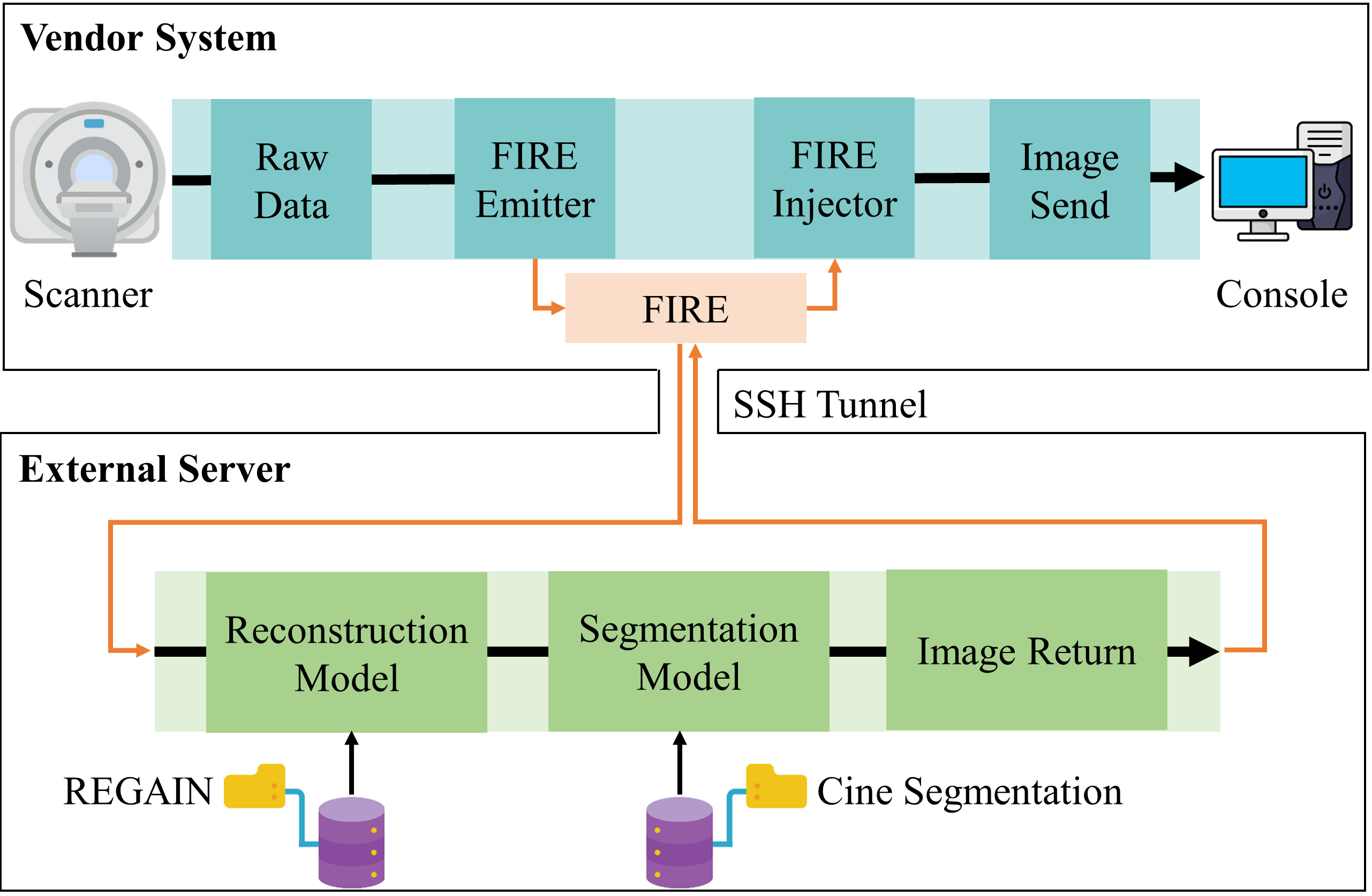
We implemented a fully automated inline CMR segmentation pipeline on a Siemens 3T scanner (MAGNETOM Vida, Siemens Healthineers AG, Erlangen, Germany) (Fig. 1). Initially, images were reconstructed using conventional vendor algorithms or an in-house resolution enhancement method. Data were transferred from the scanner to an external server using the Framework for Image Reconstruction prototype1. We implemented in-house reconstruction and segmentation algorithms in separate open-source Python modules, offering flexibility to deploy different DL-models. Docker containers in the external server encapsulate the Python code and dependencies.We assessed the feasibility of the automated plug-and-play platform for inline cine segmentation in 308 patients (176 males; 57±16 years) referred for clinical CMR. Cine images were acquired with an accelerated protocol with the following imaging parameters: TE/TR = 1.7/3.3 ms, flip angle = 30 degrees, slice thickness = 8 mm, temporal resolution = 53 ms, matrix size = 208 × 208, spatial resolution = 1.7 × 1.7 mm2, and phase-encoding truncation = 25% (i.e., 52 lines prescribed). With GRAPPA rate 2 and 46 ACS lines, total phase-encoding lines were 49, resulting in 4.2-fold acceleration. Images were reconstructed using resolution enhancement generative adversarial in-line neural network (REGAIN)2. Following reconstruction, the REGAIN-enhanced cine images were segmented using a segmentation network3. Both image reconstruction and segmentation models are freely available (https://github.com/HMS-CardiacMR/CineROI) and were chosen to demonstrate the feasibility of the platform.
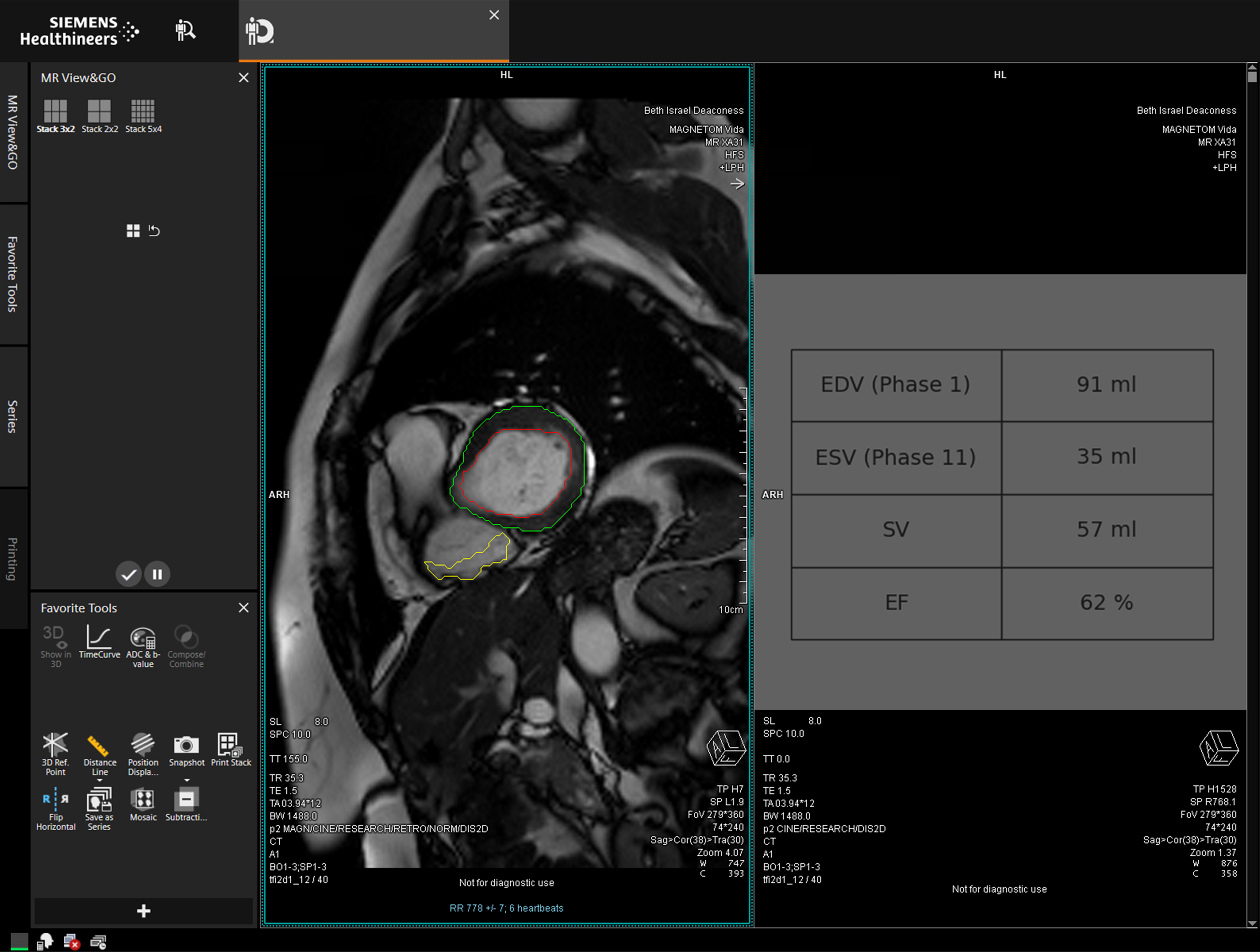
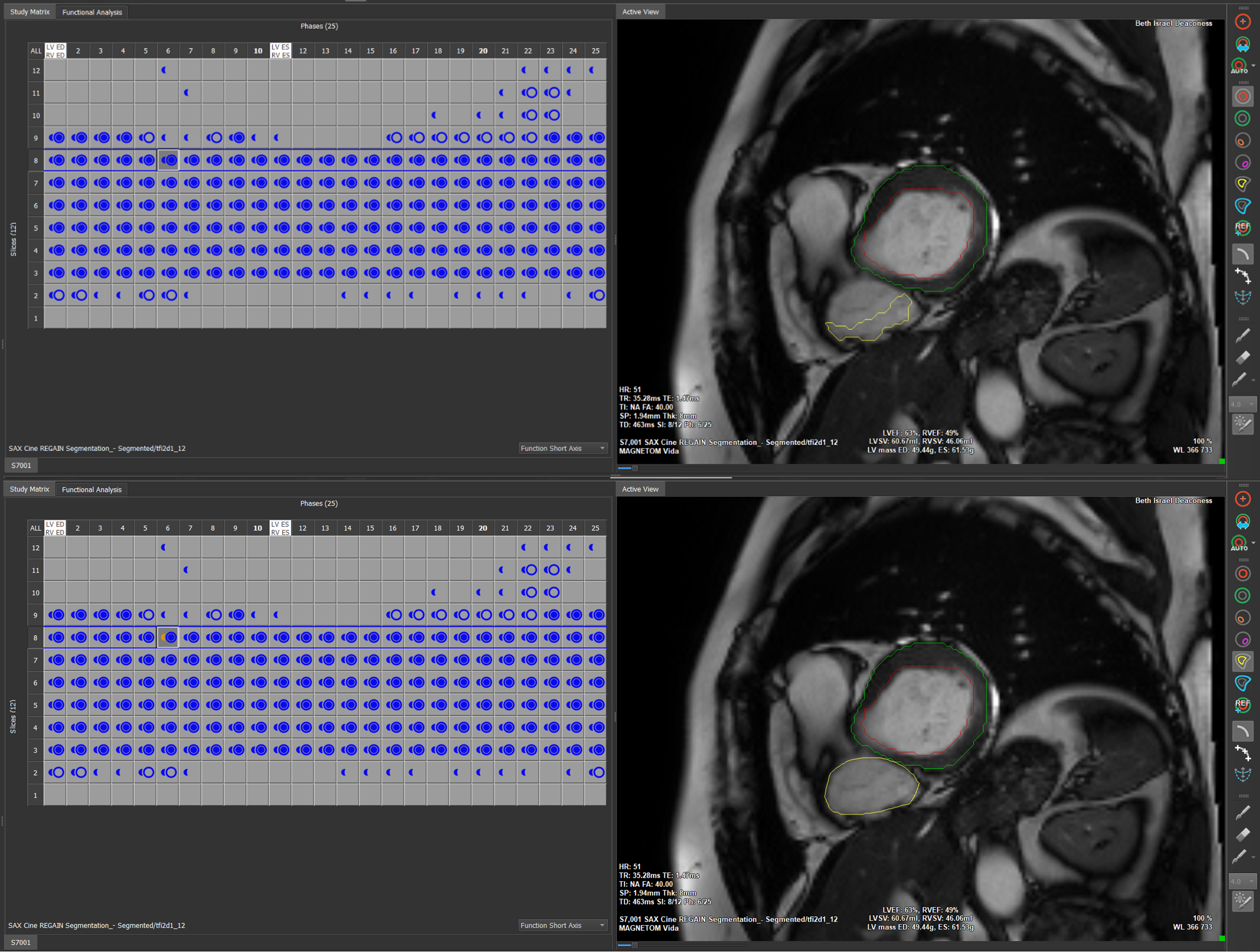
After scan completion, contoured images appeared on the scanner console, allowing immediate review and re-acquisition if necessary. Left-ventricular end-diastolic volume (EDV), end-systolic volume (ESV), stroke volume (SV), and ejection fraction (EF) were also calculated and displayed on the scanner console (Fig. 2). The DL-generated contours were stored as custom tags in the image DICOM header, which allows for offline adjustments using post-processing software. We demonstrated this by transferring the images from the scanner to Medis (Medis Medical Imaging Systems, Leiden, The Netherlands), where a custom add-on allowed us to extract the inline DL contours from the DICOM header to create a Medis-compatible contour that users can edit (Fig. 3).
Cine images were analyzed using cvi42 (Circle Cardiovascular Imaging Inc., Calgary, AB, Canada) software by a clinical fellow and reviewed by a clinical attendee. Analysis consisted of semi-automatic segmentation with manual contour correction.
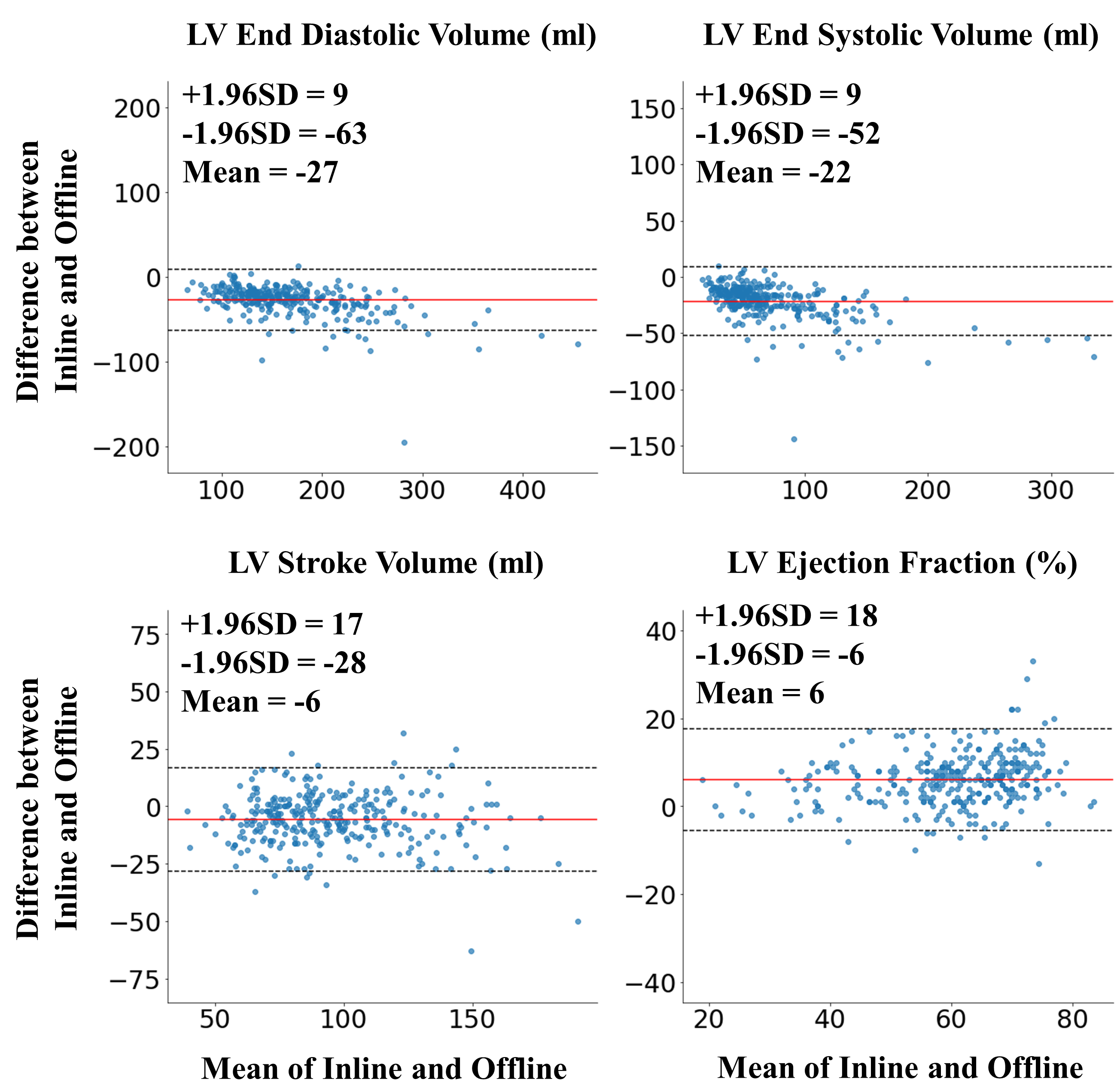
Linear regression and Bland-Altman analysis compared the inline (fully automated) and offline (semi-automated) methods for EDV, ESV, SV, and EF. All data analysis was performed using Scipy (v1.8.0). Contours were inspected to identify segmentation failures of the inline model.
Results
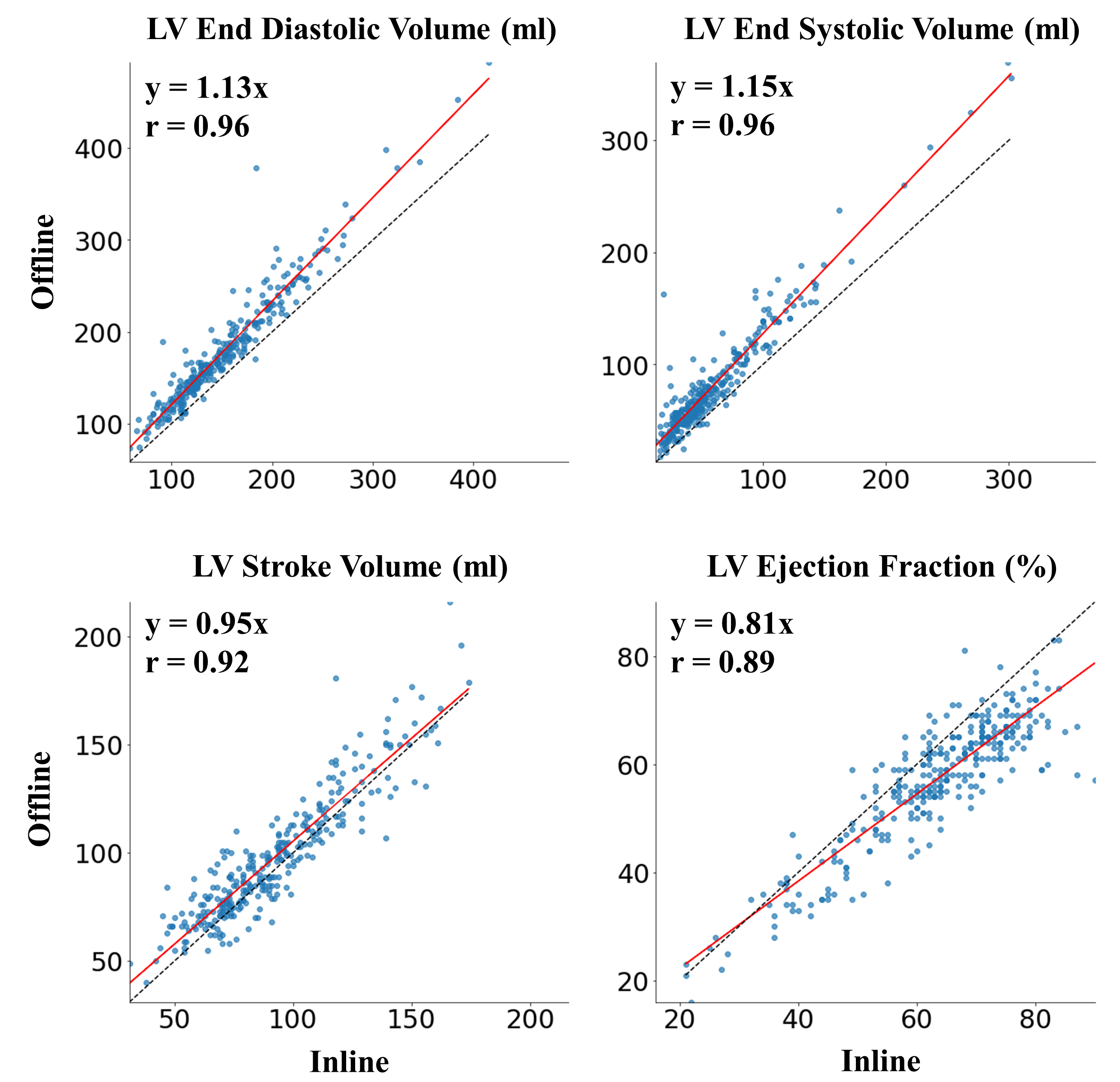
The plug-and-play inline CMR cine segmentation platform was successfully deployed and evaluated in all patients of this pilot study. There was strong agreement between inline and offline assessments (EDV: r = 0.96; ESV: r = 0.96; SV: r = 0.92; EF: r = 0.89) (Fig. 4). There was good agreement between techniques, with the 95% confidence intervals ranging from 9 ml to -63 ml for EDV, 9 ml to -52 ml for ESV, 17 ml to -28 ml for SV, and 18% to -6% for EF (Fig. 5). The cine segmentation model performed well on mid-ventricular slices but encountered challenges delineating the blood pool and myocardium in slices closer to the base and apex. Nevertheless, no slices were excluded from the analysis.Conclusion
We successfully developed and performed an initial evaluation of an open-source flexible, plug-and-play inline CMR image segmentation platform. Further refinement of segmentation networks may improve agreement with clinical analysis, which can be easily integrated into the proposed platform. Due to the modular nature of the pipeline, additional analyses such as strain can also be readily evaluated. The platform allows for rapid deployment of CMR segmentation and analysis, enabling researchers to test the feasibility and performance of any new or established DL segmentation algorithm in an open-source environment.Acknowledgements
Funding: This study is supported by the National Institutes of Health.References
1 Chow, K., Kellman, P. & Xue, H. in SCMR 24th annual scientific sessions. Virtual Meeting.2 Yoon, S. et al. Accelerated Cardiac MRI Cine with Use of Resolution Enhancement Generative Adversarial Inline Neural Network. Radiology 307, e222878, doi:10.1148/radiol.222878 (2023).
3 Morales, M. A. et al. DeepStrain: A Deep Learning Workflow for the Automated Characterization of Cardiac Mechanics. Front Cardiovasc Med 8, 730316, doi:10.3389/fcvm.2021.730316 (2021).
Figures