3378
Quantitative evaluation of carotid atherosclerotic characteristics using in vivo carotid MR imaging with MULTIPLEX1Department of Radiology, Peking University Third Hospital, Beijing, China, 2Tsinghua University, Beijing, China, 3United Imaging Research Institute of Intelligent Imaging, Beijing, China, 4Peking University Third Hospital, Beijing, China
Synopsis
Keywords: Atherosclerosis, Cardiovascular
Motivation: Conventional carotid artery wall MR imaging is time-consuming due to multiple MR acquisitions. MULTIPLEX, a fast single-scan MRI technique, provides T1W/PDW/T2* maps simultaneously. Its potential in evaluating arterial plaque remains unexplored.
Goal(s): Evaluating MULTIPLEX in characterising carotid plaque.
Approach: We compared T1/PD/T2* values of arterial morphology and plaque components (lipid-rich necrotic core/intraplaque haemorrhage/loose matrix) in 33 participants using ANOVA between conventional technique and MULTIPLEX.
Results: Significant T1/PD/T2* differences of plaque compositions mentioned above were found across all three groups with MULTIPLEX, similar to conventional technique. Varied plaque components displayed T1/PD/T2* differences.
Impact: MULTIPLEX shows promises in characterising arterial plaque beyond the brain.
Abstract
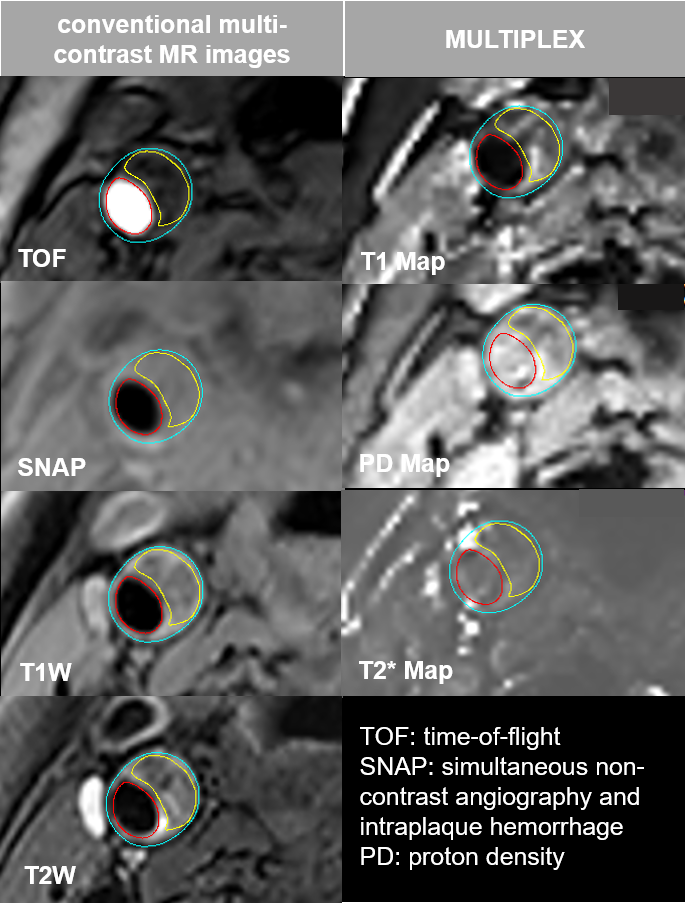
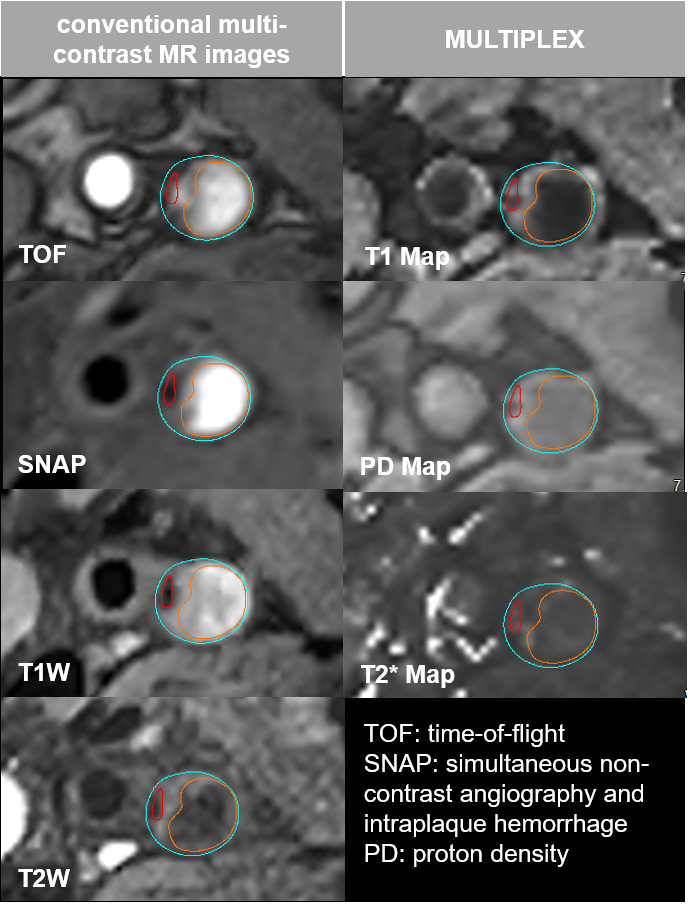
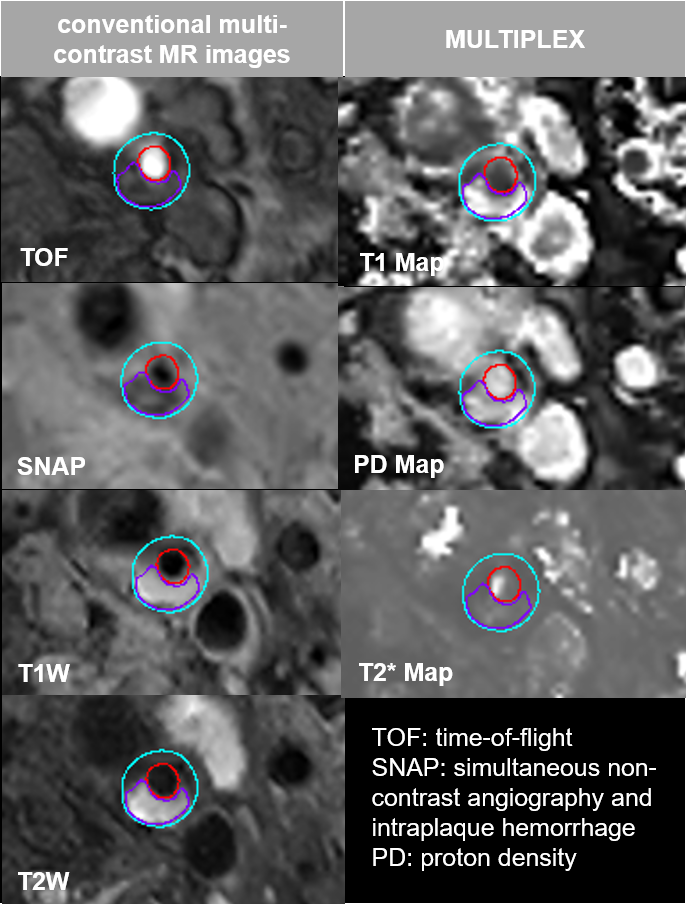
Introduction: The conventional multi-contrast carotid MR vessel wall imaging has been widly used to evaluate the carotid plaque compositional features based on signal intensity in various contrast images. The single-scan 3D multi-parametirc MR imaging, known as MULTI-parametric MR imaging with fLEXible design (MULTIPLEX) has shown great promise in evaluating the human brain [1,2]. However, its potential for evaluating carotid plaque features remains unexplored. In this study, we aimed to evaluate the value of in vivo MULTIPLEX in characterising carotid compositional features.Methods: Patients with carotid stenosis referred for carotid endarterectomy were enrolled from Jun 2022 to Aug 2022 in Peking University Third Hosptial. All participants underwent MR imaging for carotid arteries on a 3.0T MR scanner with 8-channel carotid coil to acquire following sequences: 1) conventional multi-contrast carotid MR vessel wall imaging sequences: 3D time-of-flight: TR/TE 17.6/6.7 ms, flip angle 8°, and slice thickness 2 mm; 2D T1-weighted: TR/TE 850/13.44 ms and slice thickness 2 mm; 2D T2-weighted: TR/TE 2000/96.6 ms and slice thickness 2 mm; and Simultaneous Non-contrast Angiography intraplaque hemorrhage (SNAP) imaging: TR/TE 9.6/4.0 ms, flip angle 12°, and slice thickness 1 mm; 2) MULTIPLEX sequence: TR/TE 29.8/3.55 ms, flip angle 4 °, and slice thickness 2 mm, 5 echoes, voxel size 0.60 x 0.60 x 2.00 mm3. The conventional multi-contrast carotid MR images of participants were independently evaluated by two radiologists with over 5 years’experience in neurovascular MRI. The contours of morphological features including lumen and wall as well as compositional features (Fig. 1-3) (including lipid rich necrotic core (LRNC), intraplaque hemorrhage (IPH) and loose matrix (LM) of plaque in the index carotid artery) were outlined on multi-contrast carotid MR images using VesselExplorer2 (Tsimaging Healthcare, Beijing, China) [3-5]. The quantitative carotid MR images were registered with multi-contrast carotid MR images in three steps. First, the resolution of quantitative carotid MR images was interpolated to be consistent with multi-contrast images. Second, the quantitative and multi-contrast images were automatically matched according to the location information of each slice. Third, the contours of lumen, wall and plaque components on multi-contrast images were mapped to the matched quantitative mages, and radiologists manually registered the quantitative and multi-contrast images based on those contours with Matlab2020a. The mean values of T1, PD and T2* of wall and the above plaque components on quantitative images were computed and compared using ANOVA.
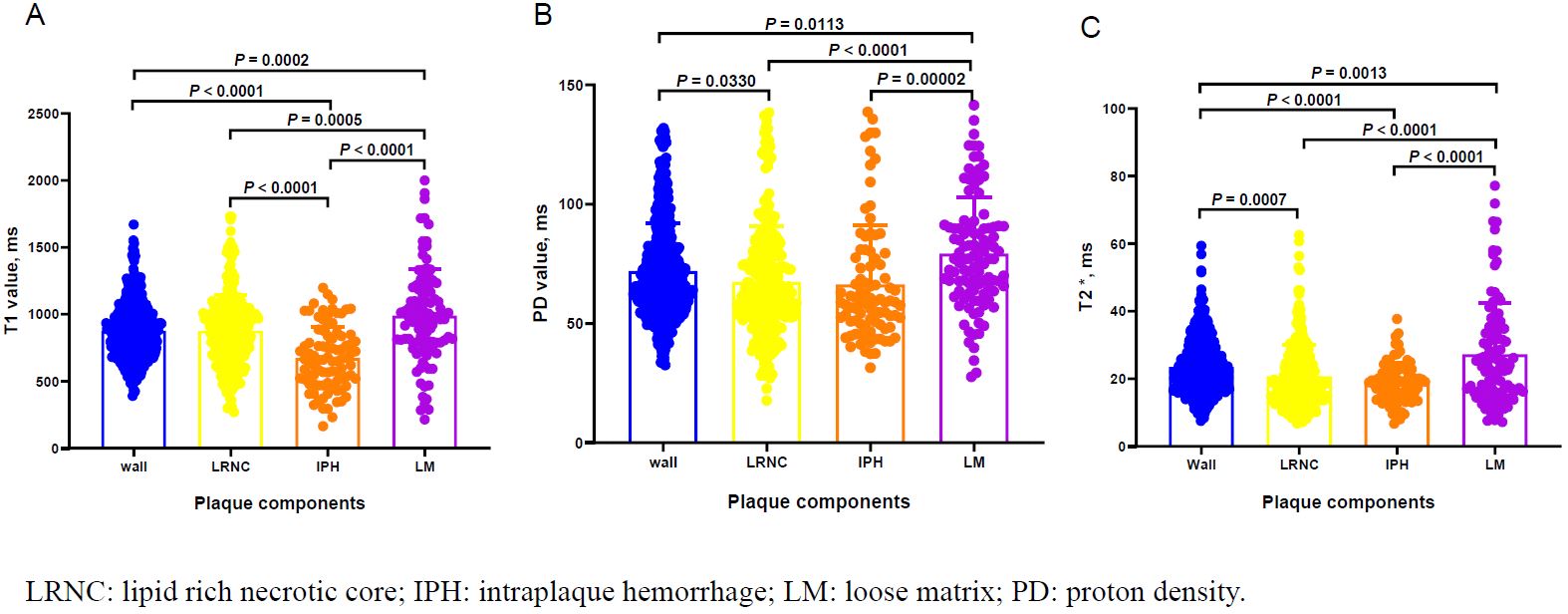
Results: In total, 33 subjects (65.3 ± 7.2 years, 21 males) were included, of which 32 (97.0%), 15 (45.5%) and 22 (66.7%) had carotid LRNC and IPH as well as LM respectively. The mean and standard deviations were as follows: 1) T1 values (ms), wall/LRNC/IPH/LM, 878.1 ± 208.3/877.6 ± 267.6/673.8 ± 234.6/990.1 ± 350.2; 2) PD values (ms), wall/LRNC/IPH/LM, 72.1 ± 20.0/67.5 ± 23.4/66.4 ± 24.9/79.4 ± 23.6; and 3) T2* values (ms), wall/LRNC/IPH/LM, 23.5 ± 8.0/20.8 ± 9.4/18.8 ± 5.9/27.2 ± 15.3. Our ANOVA results identified significant differences (Fig. 4) (T1: F = 27.2, p< 0.001; PD: F = 9.0, p< 0.001; and T2*: F = 18.5, p< 0.001) across all the three groups. Post hoc analysis identified the PD/T2* mean values of LRNC were lower than that of wall, the T1/T2* mean values of IPH were lower than that of wall, and T1/PD/T2* mean values of LM were always higher than those of wall. Furthermore, the results of inter-composition comparasions identified that significant differences in T1/PD/T2* mean values between LRNC and LM (ps< 0.001), in T1/PD/T2* values between IPH and LM (ps< 0.001), and in T1 mean values between LRNC and IPH (p< 0.001).
Conclusion: The carotid MR imaging with MULTIPLEX including quantitative values of T1/PD/T2* have the potential capability of evaluating plaque compositional features.
Acknowledgements
This work was supported by National Natural Science Foundation of China (82302287).References
[1] Ye Y, Lyu J, Hu Y, et al. MULTI-parametric MR imaging with fLEXible design (MULTIPLEX). Magn Reson Med 2022;87(2):658-673.
[2] Warntjes JB, Leinhard OD, West J, Lundberg P. Rapid magnetic resonance quantification on the brain: optimization for clinical usage. Magn Reson Med 2008;60:320-329.
[3] Saam T, Ferguson MS, Yarnykh VL, et al. Quantitative evaluation of carotid plaque composition by in vivo MRI. Arterioscler Thromb Vasc Biol 2005;25(1):234-239.
[4] Chu B, Kampschulte A, Ferguson MS, et al. Hemorrhage in the atherosclerotic carotid plaque: A high-resolution MRI study. Stroke 2004;35(5):1079-1084.
[5] Cai JM. Hatsukami TS, Ferguson MS, et al. Classification of human carotid atherosclerotic lesions with in vivo multicontrast magnetic resonance imaging. Circulation;106(11):1368-73.
Figures