3376
MRI findings of aneurysmal inside and walls associated with sac shrinkage after endovascular aortic repair1Dapartment Of Radiology, Nippon Medical School Hospital, Tokyo, Japan, 2Dapartment Of Radiology, Nippon Medical School Chiba Hokusoh Hospital, Inzai, Japan, 3Dapartment Of Radiology, Nippon Medical School Musashikosugi Hospital, Kawasaki, Japan, 4Department Of Cardiothoracic Surgery, Nippon Medical School Chiba Hokusoh Hospital, Inzai, Japan
Synopsis
Keywords: Vascular, Cardiovascular, Abdominal aortic aneurysm
Motivation: To survey radiographical parameters to predict outcomes after EVAR.
Goal(s): To reveal new MRI findings associated with aneurysmal shrinkage.
Approach: Various MRI findings were extracted from fifty patients and the relationship between each finding and aneurysmal volume change was analyzed.
Results: Lack of endoleak, endoleak with clear boundary shapes, homogenous signal pattern or uncomplex heterogenous signal pattern of intra-aneurysmal thrombus, and aneurysmal wall enhancement and thickening were noted as the factors for sac shrinkage.
Impact: Some specific MRI findings as lack of endoleak, clear endoleak boundary, homogenous or uncomplex heterogenous thrombus, and aneurysmal wall enhancement thickening were noted as the factors for sac shrinkage.
Introduction
Imaging characteristics indicating outcomes after endovascular aortic repair (EVAR) for abdominal aortic aneurysms (AAA) are not satisfactory established. The issue regarding how endoleak relates with sac enlargement has not been fully demonstrated1,2). Meanwhile, some other imaging characteristics other than endoleak are also known as the predictive factors of volume changes3). This study aimed to reveal various new MRI findings involving aneurysmal shrinkage. We analyzed the association with aneurysmal volume change and the MRI findings of endoleak, signals within intra-aneurysmal thrombus, and aneurysmal wall enhancement and thickening.Methods
PatientsPatients underwent EVAR for AAA and/or common iliac artery aneurysms and were examined using contrast-enhanced MRI as the follow-up survey between April 2018 and September 2023 were enrolled.
MR Imaging Techniques
MR images were obtained using a 3-T whole-body scanner (Discovery MR750; GE) equipped with a 16-channel body matrix coil. Three sequences—T2WI with a Single-shot Fast Spin Echo (SSFSE), T1WI Black-Blood (BB), and Gadolinium (Gd)-enhanced fast time-of-flight spoiled gradient recalled echo (Fast TOF SPGR)—were mainly used in this study. In T2WI with SSFSE, following parameters were used: repetition time (TR)/echo time (TE), 3500/81.7 ms; flip angle, 90°; field of view (FOV), 320 × 320 mm2; image matrix, 320 × 320; resulting pixel size, 0.9 × 0.9 mm; and slice thickness, 8 mm. In T1WI BB, following parameters were used: TR/TE, 1304/37.6ms; flip angle, 107°; FOV, 320 × 320 mm2; image matrix, 320 × 320; resulting pixel size, 0.9 × 0.9 mm; and slice thickness, 8 mm. In Gd-enhanced Fast TOF SPGR with chemical shift-selective fat-suppression, Gd-contrast medium with the amount of 0.1 mmol per kg of body weight was injected at the speed of 0.1-0.2 ml/sec, and images were acquired during 3–3.5 min using following parameters: TR/TE, 7.1/2.3 ms; flip angle, 14°; FOV, 320 × 320 mm2; image matrix, 388 × 388; resulting pixel size, 0.8 ×0.8 mm; and slice thickness, 0.8 mm.
CT volumetry
The aneurysm sac volumes were measured using CT data gained at the nearest date from MRI scan and approximately one year before. Intra-arterial volume between the level immediately distally to the lowest renal artery and the aneurysmal distal end was obtained4), and the volume change ratio (VCR) for one year was calculated.
Image Analysis
MRI findings were stratified as follows. First, from Gd-enhanced fast SPGR sequence, whether visible endoleak existed or not was differentiated and the boundary of endoleak were divided into clear or unclear shape(Figure1). Second, based on signal patterns in the non-contrast T1WI BB and T2WI with SSFSE, intra-aneurysmal thrombus was divided into homogenous or heterogenous. Homogenous group was further divided into methemoglobin or hemosiderin pattern(Figure2). Heterogenous group was further divided into uncomplex or complex pattern(Figure3). Third, the existence of aneurysmal wall enhancement and thickening was extracted. Thereafter, the relationship between each MRI finding and the aneurysmal volume change was statistically analyzed.
Results
Fifty patients (41 males and 9 females, mean age; 78 [range 57–91] years old) were analyzed. The lack of endoleak (n=21; VCR: 93.4 ± 22.8%) and the endoleak with clear boundary shape(n=13; VCR: 95.0 ± 15.1%) related to shrinkage than the endoleak with unclear boundary (n=16; VCR: 113.7 ± 22.0%), (p=0.001) (Figure4). Regarding intra-aneurysmal thrombus, the homogenous group (n=21; VCR: 88.2 ± 17.7%) shrunk more than the heterogenous group (n=29; VCR: 109 ± 21.6%), (p<0.001). Among the heterogenous group, the complex pattern as multi-cracked or mix patterns (n=14) was mostly associated with enlargement (VCR: 120 ± 23.8%, p<0.001)(Figure5). The aneurysmal wall thickening (n=10; VCR: 77.9 ± 15.5%) showed higher shrinking tendency than the lesions without wall enhancement and thickening (n=34; VCR: 106 ± 19.9%), (p<0.001).Discussion
MR signal pattern of thrombus could be considered based on the oxygenation of hemoglobin (Hb)5). The area where blood inflow and outflow are in balance tends to form simple endoleak channel with the clear boundary shape; There, the surrounding thrombus has little connection with oxy-Hb and changes to met-Hb or hemosiderin. Meanwhile multiple endoleak channels with unclear boundary shapes, the risk factor of aneurysm enlargement, irregularly spreads into the surrounding thrombus; There, different phases of unorganized thrombus simultaneously exist, and the MR signals tends to appear heterogenous and complex patterns. The issue about the association with aneurysmal wall enhancement and sac shrinkage is recently argued from the CT data6,7). We could more clearly detected this phenomenon using superior spatial resolution of MRI.Conclusion
Several imaging features demonstrated from MRI related to the change in aneurysmal volume. Lack of endoleak, clear endoleak boundary, homogenous or uncomplex heterogenous thrombus, and wall enhancement and thickening were noted as the factors for sac shrinkage.Acknowledgements
No acknowledgement found.References
1) Patel R, Sweeting MJ, Powell JT, et al. Endovascular versus open repair of abdominal aortic aneurysm in 15-years’ follow-up of the UK endovascular aneurysm repair trial 1 (EVAR trial 1): a randomised controlled trial. Lancet 2016;388:2366-74
2) Williams AB, Williams ZB. Imaging modalities for endoleak surveillance. J Med Radiat Sci. 2021;68(4):446–452.
3) Cornelissen S.A., Verhagen H.J., van Herwaarden J.A., et al. Lack of thrombus organization in nonshrinking aneurysms years after endovascular abdominal aortic aneurysm repair. J Vasc Surg. 2012;56:938–942.
4) Muller-Wille R, Schotz S, Zeman F, et al. CT features of early type II endoleaks after endovascular repair of abdominal aortic aneurysms help predict aneurysm sac enlargement. Radiology 2015;274:906–916
5) Macellari F, Maurizio P, Giancarlo A, et al. Neuroimaging in intracerebral hemorrhage.Stroke. 2014;45(3):903–908.
6) Ito E, Toya N, Toya N, Fukushima S, et al. Aneurysm wall enhancement detected by contrast computed tomography scan is associated with aneurysm shrinkage after endovascular aneurysm repair for abdominal aortic aneurysm. Circ J 2018; 82: 340-5.
7) Shinya Okata 1, Katsuyuki Hoshina, Kazuhiro Miyahara, et al. High aneurysm wall enhancement values are associated with late sac shrinkage after endovascular repair of abdominal aortic aneurysms. Medicine. 2021 Jan 15;100(2):e24133
Figures
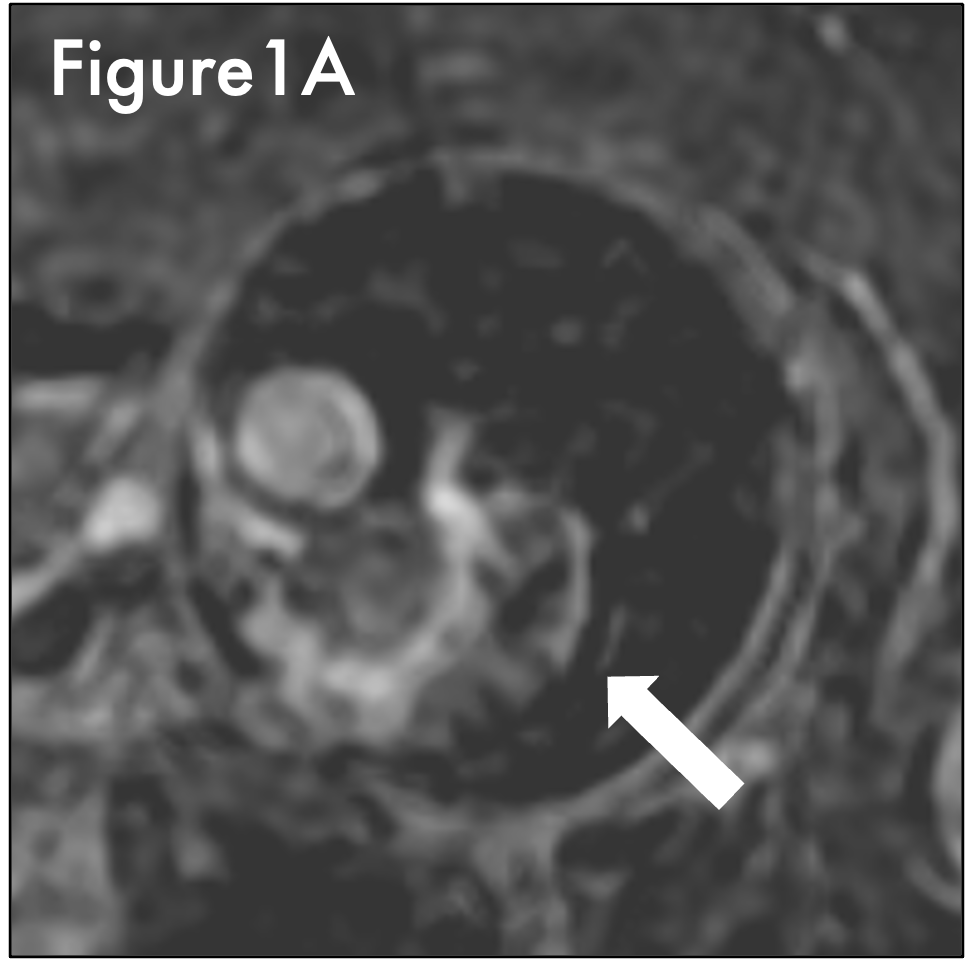

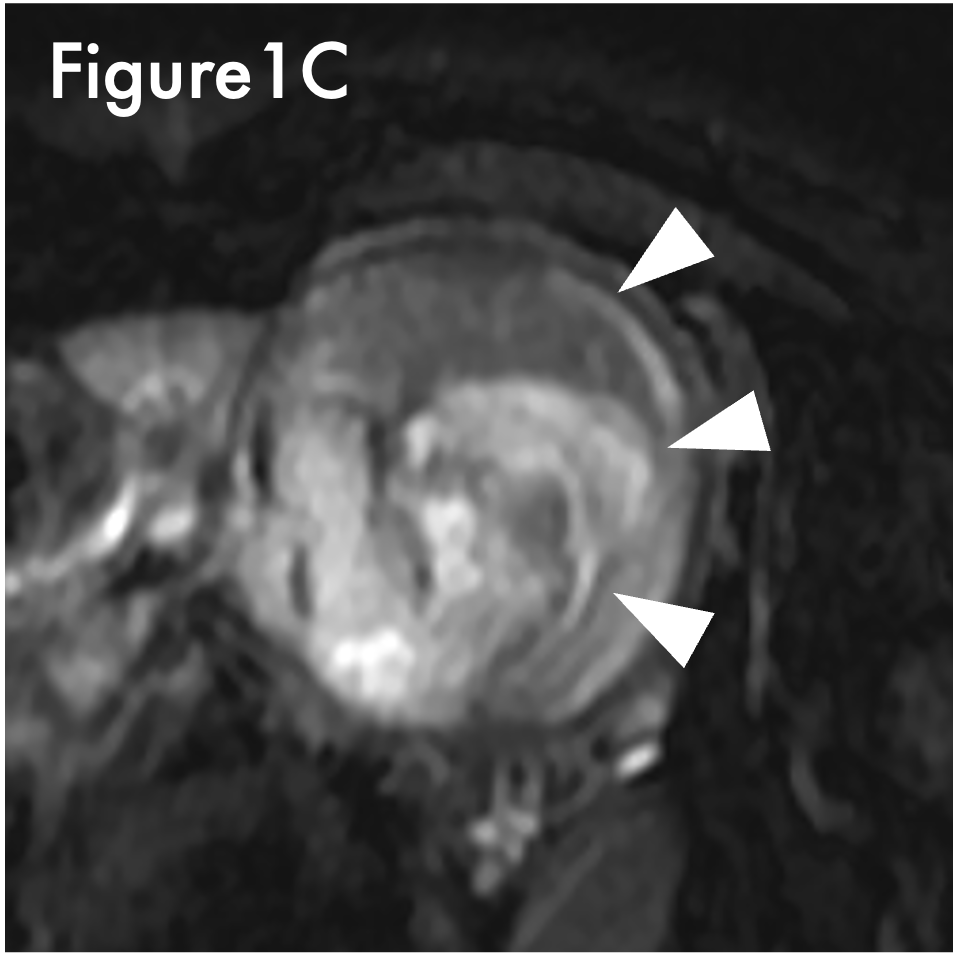
Figure1C. Complex heterogneous signal pattern of thrombus (FS T2WI with SSFSE). There were multi-cracked in the cavity(arrowhead).
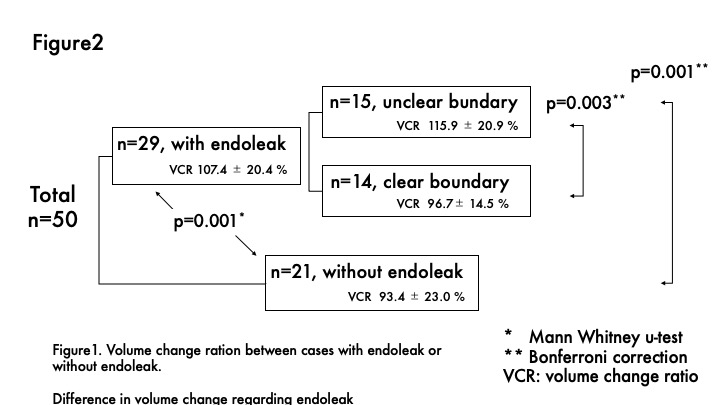
Figure2. Difference in volume change regarding endoleak.
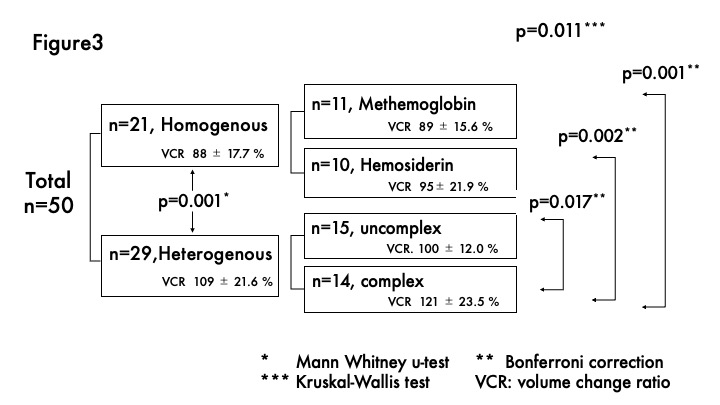
Figure3. Difference in volume change regarding signal of intra-aneurysmal thrombus.