3372
A preliminary study of accelerated mDIXON for segmented coronary adipose tissue evaluation in patients with suspected coronary artery disease1Radiology, West China Hospital, Sichuan University,, Chengdu, China, 2Clinical Science, Philips Healthcare, Chengdu, China
Synopsis
Keywords: Atherosclerosis, Cardiovascular, pericoronary adipose tissue
Motivation: We attempted to assess pericoronary adipose tissue using the mDIXON sequence of magnetic resonance imaging
Goal(s): To evaluate the relationship between pericoronary adipose tissue and coronary stenosis grade and plaque type
Approach: Study design to test the hypothesis
Results: Pericoronary adipose tissue volume is independently associated with the type of coronary plaque
Impact: Magnetic resonance imaging is more accurate for the assessment of adipose tissue. This is the first time to apply MRI to the assessment of pericoronary adipose tissue, and to verify its direct relationship with coronary plaque type and stenosis grade.
Introduction
Pericoronary adipose tissue (PCAT) has been suggested to contribute to the development of coronary artery disease (CAD) (1). The secretion of dysfunctional PCAT is positively correlated with coronary artery stenosis, degree of calcification, and plaque progression (2). It is important to develop novel clinical diagnostic tools for coronary heart disease based on PCAT assessment. Coronary computed tomography angiography (CCTA) is the preferred method for quantitative PCAT assessment (3). But it is not suitable for follow-up examinations due to radiation exposure. Homsi et al. (4) introduced and validated coronary magnetic resonance angiography (MRA), based on the three-dimensional (3D)-modified Dixon (mDIXON) technique, for epicardial adipose tissue (EAT) quantification. They reported excellent agreement between the measured and actual EAT volumes. However, to maintain a high spatial resolution, conventional 3D-mDixon whole-heart coronary MRA requires a long scan time and makes the image quality susceptible to heart rate and respiratory pattern drift (5). To speed up scanning without compromising image quality, we used the compressed sensing artificial intelligence (CSAI) framework which combines deep learning (DL) and CS techniques to optimize the CS reconstruction algorithm while performing denoising and shortening the scanning time (6).Therefore, the present study was to use non-contrast-enhanced CSAI-based 3D mDIXON coronary MRA for PCAT quantification in patients with suspected CAD. It also evaluated segmented PCAT’s relationship with coronary plaque characteristics and stenosis severity.Methods
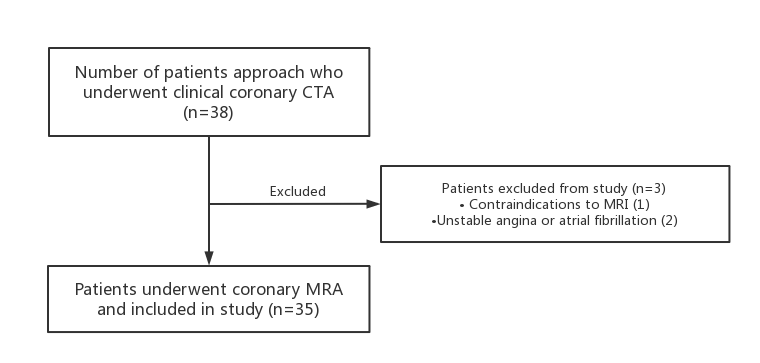
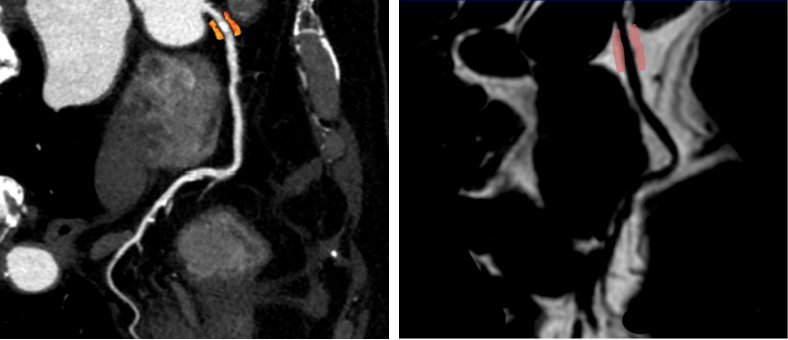
The study protocol was approved by the institutional ethics committee of the hospital. We included 35 symptomatic patients with CAD (111 arteries with plaque, 169 without plaque) (Figure 1). All the subjects underwent cardiac magnetic resonance (CMR) on a 3T clinical MR scanner (Ingenia Elition, Philips Healthcare) with a 16-channel body matrix coil combined with a 12-channel spine matrix coil to evaluate segmented PCAT volume and fat-fraction of 8 coronary segments. Data was acquired using a 3D ECG-gated and respiratory navigator magnetization-prepared mDixon-sequence with the following optimized parameters: FOV = 265 × 301 × 112 mm³; acquisition voxel size = 1.5 × 1.5 × 1.5 mm³ (150 overcontiguous slices), reconstructed voxel size = 0.75 × 0.75 × 0.75 mm³, TR = 4.1 ms. The analysis was performed using IntelliSpace Discovery (Philips Healthcare). We manually traced the segmented PCAT volume (Figure 2), and calculated the fat fraction of the segmented PCAT by formula: only fat images (F)/F + only water images (W) (7). We compared the segmented PCAT volume and fat-fraction across 8 coronary segments with different plaque types and degrees of stenosis defined with CCTA and explored the relationship between them using Kruskal - Wallis H test and One-way analysis of variance (ANOVA) testing.Results
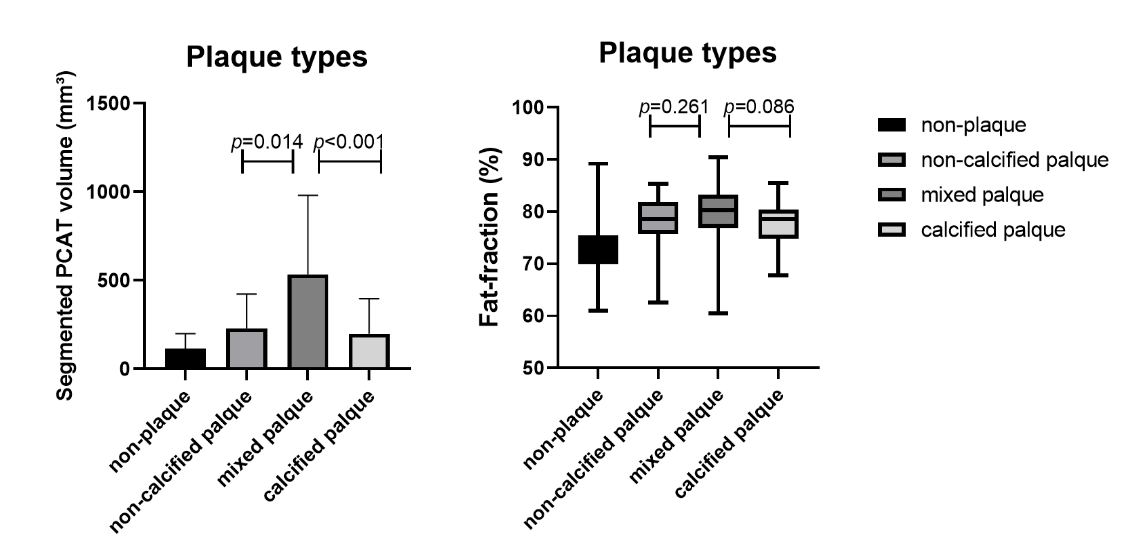
The coronary segments with plaques had a higher segmented PCAT volume and fat-fraction than those without plaques. Meanwhile, segmented PCAT volume around mixed plaques was larger than non-calcified or calcified plaques (p = 0.014 and p < 0.001) (Figure 3). There was a moderate correlation between the segmented PCAT volume and plaque type (r = 0.493, p < 0.001). The fat-fraction had similar results (r = 0.480, p < 0.001).Discussion
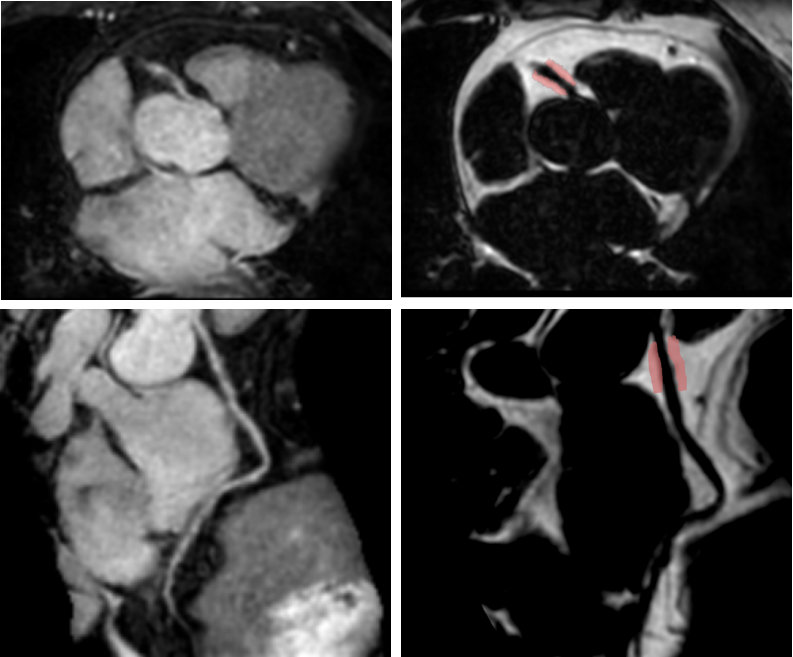
Our results indicate that the accelerated 3D-mDixon coronary MRA can be used to effectively measure PCAT volumes and fat-fractions (Figure 4). The segmented PCAT volume and fat-fraction were greatest in vessels with mixed-type plaques compared to other plaque types. This aligns with the hypothesis that plaque calcification increases its stability (8), and supports the role of a signaling pathway originating from PCAT that could lead to vascular inflammation and plaque instability (9). There was also an independent association of segmented PCAT volume with plaque characteristics in the coronary segment.Conclusion
The non-contrast-enhanced, whole-heart coronary MRA framework with CSAI is able to measure segmented PCAT volume and fat-fraction. The segmented PCAT volume is more significantly associated with the coronary plaque characters than fat-fraction.Acknowledgements
No acknowledgement found.References
1. Rosito GA, Massaro JM, Hoffmann U, Ruberg FL, Mahabadi AA, Vasan RS, et al. Pericardial fat, visceral abdominal fat, cardiovascular disease risk factors, and vascular calcification in a community-based sample: the Framingham Heart Study. Circulation 2008;117:605-613
2. Mahabadi AA, Massaro JM, Rosito GA, Levy D, Murabito JM, Wolf PA, et al. Association of pericardial fat, intrathoracic fat, and visceral abdominal fat with cardiovascular disease burden: the Framingham Heart Study. Eur Heart J 2009;30:850-856
3. Goeller M, Achenbach S, Cadet S, Kwan AC, Commandeur F, Slomka PJ, et al. Pericoronary Adipose Tissue Computed Tomography Attenuation and High-Risk Plaque Characteristics in Acute Coronary Syndrome Compared With Stable Coronary Artery Disease. JAMA Cardiol 2018;3:858-863
4. Homsi R, Meier-Schroers M, Gieseke J, Dabir D, Luetkens JA, Kuetting DL, et al. 3D-Dixon MRI based volumetry of peri- and epicardial fat. Int J Cardiovasc Imaging 2016;32:291-299
5. Lu H, Guo J, Zhao S, Yang S, Ma J, Ge M, et al. Assessment of Non-contrast-enhanced Dixon Water-fat Separation Compressed Sensing Whole-heart Coronary MR Angiography at 3.0 T: A Single-center Experience. Acad Radiol 2022;29 Suppl 4:S82-S90
6. Wu X, Deng L, Li W, Peng P, Yue X, Tang L, et al. Deep Learning-Based Acceleration of Compressed Sensing for Noncontrast-Enhanced Coronary Magnetic Resonance Angiography in Patients With Suspected Coronary Artery Disease. J Magn Reson Imaging 2023
7. Homsi R, Meier-Schroers M, Gieseke J, Dabir D, Luetkens JA, Kuetting DL, et al. 3D-Dixon MRI based volumetry of peri- and epicardial fat. Int J Cardiovasc Imaging 2016;32:291-299
8. Margaritis M, Antonopoulos AS, Digby J, Lee R, Reilly S, Coutinho P, et al. Interactions between vascular wall and perivascular adipose tissue reveal novel roles for adiponectin in the regulation of endothelial nitric oxide synthase function in human vessels. Circulation 2013;127:2209-2221
9. Ahn SG, Lim HS, Joe DY, Kang SJ, Choi BJ, Choi SY, et al. Relationship of epicardial adipose tissue by echocardiography to coronary artery disease. Heart 2008;94:e7
Figures