3369
Turbo spin-echo based enhanced acceleration-selective arterial spin labeling (eAccASL) for the lower extremity MR angiography1Department of Radiology, Tokai University Hospital, Kanagawa, Japan, 2Division of Health Sciences, Graduate School of Medical Sciences, Kanazawa University, Ishikawa, Japan, 3Department of Radiological Technology, Juntendo University, Tokyo, Japan, 4Department of Diagnostic Radiology, Tokai University School of Medicine, Kanagawa, Japan, 5Philips Japan, Tokyo, Japan
Synopsis
Keywords: Vascular, Blood vessels
Motivation: The lower extremity MR angiography (MRA) without electrocardiography (ECG) or peripheral pulse unit (PPU) triggering and contrast enhancement is useful for diagnosing peripheral arterial disease (PAD), which can avoid synchronization failure and nephrogenic systemic fibrosis (NSF).
Goal(s): Our goal was to improve peripheral arterial depiction without ECG or PPU and contrast agent.
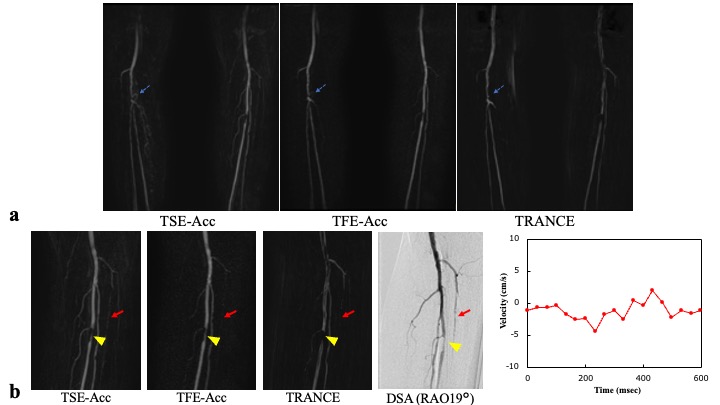
Approach: TSE-based enhanced acceleration-selective arterial spin labeling (eAccASL) (TSE-Acc) was compared with TFE-based eAccASL (TFE-Acc), and TRANCE as a reference standard by SIR, CNR, and visual inspection.
Results: CNR and arterial visibility score for TSE-Acc were higher than TFE-Acc, but no difference compared with TRANCE.
Impact: TSE-based enhanced acceleration-selective arterial spin labeling (eAccASL) can provide clear depiction of the peripheral arteries without ECG or PPU and contrast agent, providing sufficient diagnostic performance in PAD patients with arrhythmia and CKD.
Introduction
The lower extremity MR angiography (MRA) without electrocardiography (ECG) or peripheral pulse unit (PPU) triggering and contrast enhancement is useful for diagnosing peripheral arterial disease (PAD), which can avoid synchronization failure and nephrogenic systemic fibrosis (NSF). Recently, TFE-based enhanced acceleration-selective arterial spin labeling (eAccASL) (TFE-Acc)1,2. is reported as the lower extremity MRA technique without ECG, PPU, and contrast agents3. However, the arterial depiction of TFE-Acc on distal side was slightly weak due to weak inflow effect. The PAD patients have slower arterial blood flow. We aimed to compare TSE-based eAccASL (TSE-Acc)4 and TFE-Acc without ECG or PPU triggering and contrast enhancement as peripheral lower extremity MRA, using triggered angiography non-contrast enhanced (TRANCE) as a reference standard.Methods
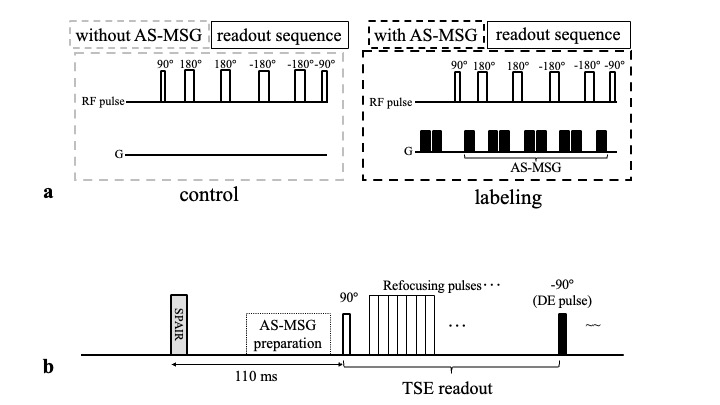
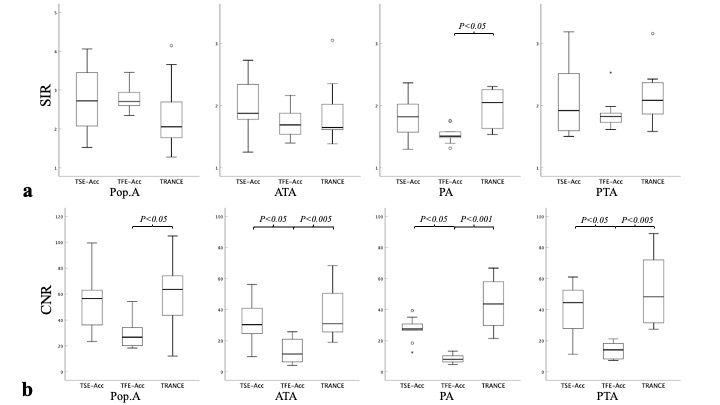
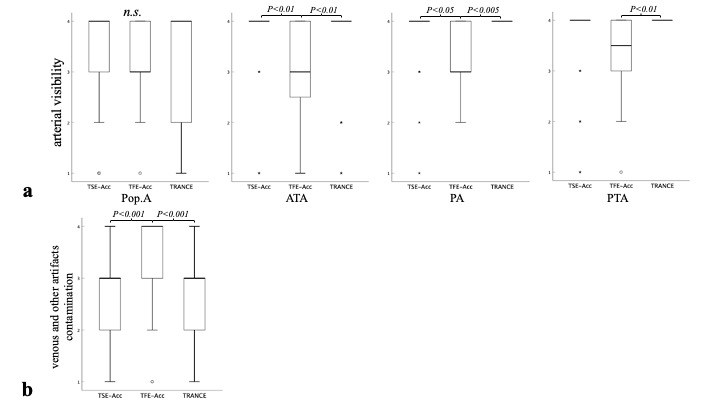
eAccASL technique: The eAccASL sequences consist of a control and labeling module. The control or labeling module consists of T2 preparation pulse of a 90°excitation pulse, MLEV 180° refocusing pulses, and a -90° flip back pulse. In addition, MSGs were placed in the labeling module. The number of 180° refocusing pulses in the control or labeling module is four for eAccASL. The MSG strength is defined by the acceleration causing a phase change of π (AENC: acceleration-encoding).Subjects and equipment: Nine healthy volunteers were studied after obtaining informed consent as required by hospital review board; these sequences were implemented on a 3.0 T MR system (Philips, Ingenia R5). .Acquisition parameters: TSE-Acc were: sequence, 3D T2-TSE; TR/TE, 800/65 ms; FA, 90°; refocusing angle, 150°; ETL, 20; SPAIR; driven equilibrium (DE) pulse; SENSE factor (RL/AP), 3.0/2.0; prep TE, 56ms; AENC, 0.58m/s2; and total acquisition time (labeling and control), 3 m 04 s. TFE-Acc were: sequence, 3D T1-TFE; TR/TE, 8.3/3.3 ms; FA, 11°; ETL, 60; PROSET; SENSE factor (RL/AP), 3.0/1.3; prep TE, 56ms; AENC, 0.58m/s2; and total acquisition time (labeling and control), 3 m 48 s. TRANCE were: sequence, 3D T2-TSE; TR/TE, 1 heartbeat/65 ms; FA, 90°; refocusing angle, 150°; ETL, 20; SENSE factor, 3.0/2.0; and total acquisition time, from 3 min 37 s to 4 min 15 s depending on heart rate (HR).Image assessment: Artery-to-muscle signal intensity ratio (SIR) and contrast-to-noise ratio (CNR) of popliteal artery (Pop. A), anterior tibial artery (ATA), posterior tibial artery (PTA), and peroneal artery (Pero. A) were calculated. Rectangular region-of interests (ROIs) were placed on gastrocnemius muscle (GM) and above arteries in the subtracted images. The following equations were used for SIR and CNR: SIR = Aave/GMave and CNR = (Aave−GMave)/GMSD, where the Aave is mean signal intensity in each arterial ROI, GMave and GMSD are mean signal intensity and standard deviation in the GM ROI. In addition, arterial visibility (1: poor, 4: excellent), and artifacts contamination (1: severe, 4: no) were assessed independently by two radiologists. The Friedman and post-hoc tests were used for the statistical analysis and a p value less than 0.05 was considered significant.Clinical test: a PAD patient with diabetes, chronic kidney disease (CKD), and arrhythmia (ankle-brachial index: right, 1.11; left, 1.25) was examined using the same protocol after obtaining informed consent as required by hospital review board. In a PAD patient, phase contrast (PC) MRI data and digital subtraction angiography (DSA) were referenced.Results and Discussion
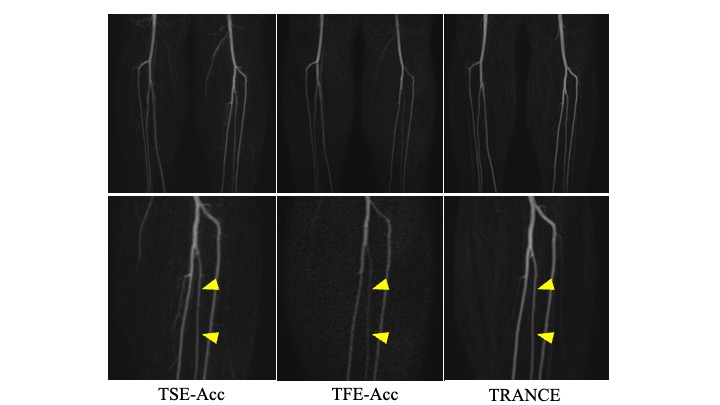
Almost all SIRs did not differ significantly among three MRA methods. On distal arterial segments, TSE-Acc had significantly higher CNRs than TFE-Acc (anterior tibial artery, p = 0.014; peroneal artery, p = 0.029; and posterior tibial artery, p = 0.014), but no difference compared with TRANCE (all p > 0.05). Since the SIRs of TSE-Acc did not differ from those of TFE-Acc, the higher CNRs on TSE-Acc may attribute to less noise components than TFE-Acc. Because the signal-to-noise ratio (SNR) of TSE-Acc using a 90° excitation pulse is higher than that of TFE-Acc using a 11° excitation pulse in terms of the MR signal amplitude, the noise components of TSE-Acc should be less than those of TFE-Acc for the same SIR. Arterial visibility scores showed the same trend as the CNRs. Meanwhile, artifacts contamination of TSE-Acc showed significantly inferior, but within acceptable level, compared with TFE-Acc. In a PAD patient, TSE-Acc more accurately visualized the slowed down peripheral arteries than TFE-Acc, and the collateral and stenosis vessels than TRANCE. eAccASL is considered sensitive to visualize tortuous vessels and turbulent flow such as collateral vessels. The appropriate visualization of the peripheral arteries is crucial for determining limb amputation in PAD patients.Conclusion
TSE-Acc can provide clear depiction of the peripheral arteries without ECG or PPU and contrast agent. TSE-Acc would provide sufficient diagnostic performance in PAD patients with arrhythmia and CKD.Acknowledgements
None.References
1. Obara M, Togao O, Yoneyama M, et al. Acceleration-selective arterial spin labeling for intracranial MR angiography with improved visualization of cortical arteries and suppression of cortical veins. Magn Reson Med. 2017; 77: 1996-2004.
2. Akamine Y, Obara M, Togao O, et al. Robust visualization of middle cerebral artery main trunk by enhanced acceleration-selective arterial spin labeling (eAccASL) for intracranial MRA. Magn Reson Med. 2019; 81: 3185-3191.
3. Shibukawa S, Konta N, Niwa T, et al. Non-enhanced and Non-gated MR Angiography for Robust Visualization of Peripheral Arteries Using Enhanced Acceleration-selective Arterial Spin Labeling (eAccASL). Magn Reson Med Sci. 2021; 20: 312-319.
4. Shibukawa S, Saito M, Niwa T, et al. Optimized enhanced acceleration selective arterial spin labeling (eAccASL) for non-gated and non-enhanced MR angiography of the hands. Magn Reson Imaging. 2021; 78: 1-6.
Figures