3368
Delivery of small mocluer drugs with Metal-Organic Cage-Based Microenvironment-Responsive Nanomedicine for Atherosclerosis theranostic1department of radiology, Sun Yat sen Memorial Hospital, Sun Yat-sen University, Guangzhou, China, 2Philips Healthcare, Guangzhou, China
Synopsis
Keywords: Atherosclerosis, Atherosclerosis
Motivation: Due to the complex pathogenesis of AS formation, the clinical treatment of AS with medicine is durable and often ineffective. it is necessary to seek a new strategy that is broadly applicable to all patients for AS theranostics .
Goal(s): MM nanoparticles could delivering small molecule drugs to plaques and monitored by MR in real time upon Mn2+ released from AS microenvironment-responsive MnO2 nanoparticles.
Approach: In vitro and vivo studies on 3.0T and 9.4T MR scaner.
Results: In vitro and vivo studies showed that MM could be monitored by MR in real time upon Mn2+ released from acidic- and H2O2- microenvironment-responsive MnO2 nanoparticles.
Impact: Nanocarriers(MM) exhibited remarkable in vivo MRI monitoring of the therapeutic process with a long imaging window and good biocompatibility and biosafety. This MRI-visible nanomedicine shows immense potential as a theranostic platform for AS therapy.
Atherosclerosis (AS) is a serious threat to human health due to its high incidence and induction of multivessel bed diseases.[1] Due to the complex pathogenesis of plaque formation, the clinical treatment of AS with medicine is durable and often ineffective, likely attributed to the rapid drug clearance and unsatisfactory accumulation at the arterial injury site.[2] Therefore, it is necessary to seek a new strategy that is broadly applicable to all AS patients and can alleviate plaque progression with high efficiency and biosafety.Metal-organic cage (MOC)-68-doped MnO2 (MM) nanoparticles were developed as a microenvironment-responsive nanodrug with a capacity of in-situ co-delivering small molecule drugs and O2 to inflammatory cells within plaques. Furthermore, the treatment process and therapeutic effect could be monitored by magnetic resonance imaging (MRI) in real time upon Mn2+ released from acidic- and H2O2- microenvironment-responsive MnO2 nanoparticles.
Methods
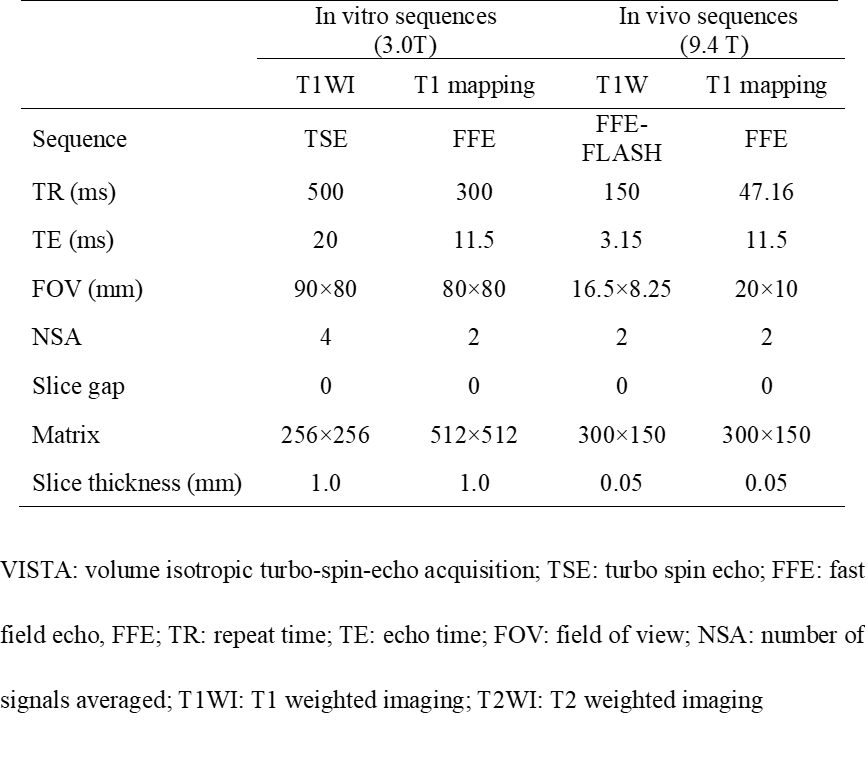
Study sample: ApoE KO mice (apolipoprotein E-deficient mice, ApoE–/–) with a C57BL/6 background fed a high-fat diet (HFD) were used for the AS model.MR imaging: For in vitro MRI, MnCl2 and MM were diluted to different concentrations in PBS (pH 6.5) with increasing Mn concentrations from 0.025 mM to 0.4 mM. The samples were then treated under different pH and H2O2 conditions in a 96-well plate and imaged using a clinical 3.0T MRI scanner (Ingenia; Philips, Netherland) with an 8-channel animal coil. For in vivo MRI, MRI scanner (9.4T, BioSpec 94/30, Bruker, USA) with 154 to 23 mm aperture volume coil and cardiac phased array coil were used to detect plaque accumulation in vivo with MM. AS model mice were injected with MM (100 μL) via the tail vein at a dose of 2.5 mg Mn kg-1 body weight. Mice were randomly selected for MRI at 0, 2, 4, 6, 8, 12, and 48 hours after injection. T1-weighted images serves as anatomical images for matching with T1 mapping to assist in delineating region of interest (ROI) and measuring T1 values. The acquisition parameters of MR sequences are detailed in Table1. Statistical analysis: The longitudinal relaxivitiy (r1 values) of MnCl2 and MM, T1 value of MM in aorta at different time points were measured and compared.
Results and Discussion
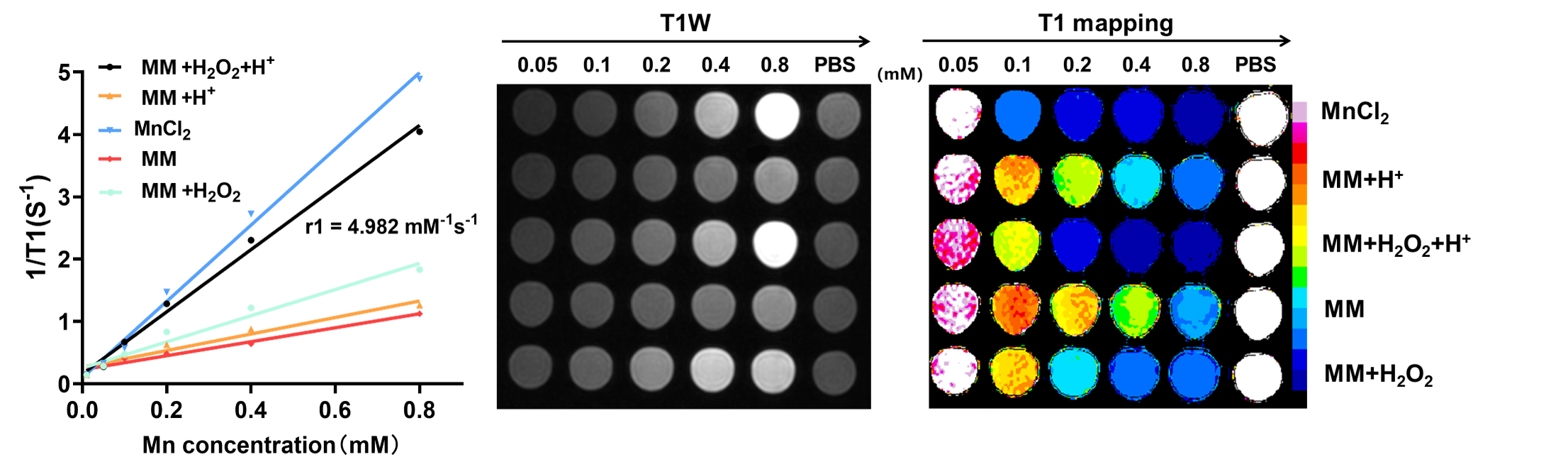
The longitudinal relaxivity (r1) of MM after treated with H2O2 at pH 6.0 was 4.982 mM-1 s-1, which is similar to that of MnCl2 (6.114 mM-1 s-1, p>0.05) and higher than that of MM treated with H2O2 at pH 7.4 (2.009 mM-1 s-1, p<0.05), without H2O2 at pH 6.0 (1.323 mM-1 s-1, p<0.05) or without H2O2 at pH 7.4 (1.121 mM-1 s-1, p<0.05, Fig. 1). These results suggest that MM has a capability of stimuli-triggered released of Mn2+ and high paramagnetic relaxivity properties. The r1 relaxivity of DMM is equivalent to that of MnCl2 and slightly higher than that of clinical contrast agents, such as gadopentetate dimeglumine (r1 = 4.1 mM-1 s-1).[3]
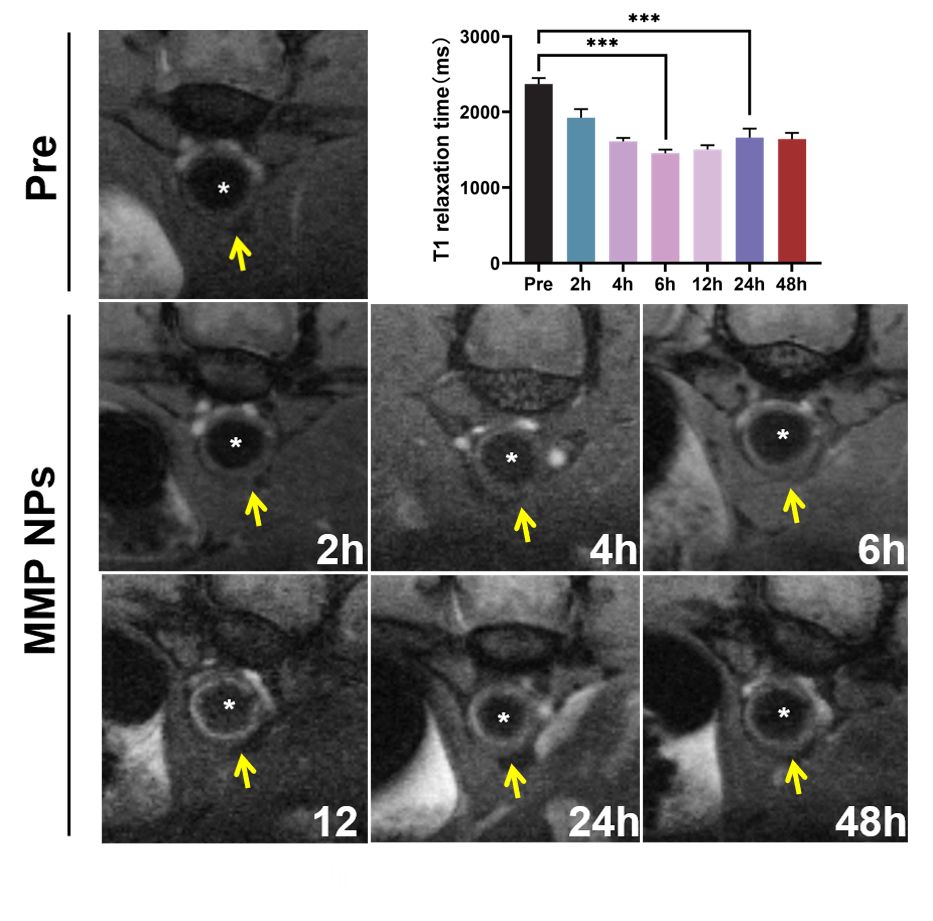
2 hours after tail vein injection of MM, a rapid contrast enhancement of the aortic plaque was found on T1-weighted imaging, reaching peak 12 hours after injection, and this enhancement slowly declined and remained over 48 hours. T1 mapping showed that the T1 values of aortic plaques gradually decreased 2 hours and reached trough at 12 hours and remained for 48 hours after injection (Fig. 2). These results suggest that MM can reach the target aortic plaques and release Mn2+ in response to the plaque microenvironment for MRI. The imaging window of 48 hours indicates the long retention time of MM in the plaque and can be continuously responsive to release of Mn2+ in the plaque, which reflects the inflammatory infiltration within the plaque.[4] Compared with other Mn-based contrast agent for plaque MRI, MM possesses higher imaging capability of plaques, which may be attributed to site-specific release of Mn2+ from MM within macrophages and foam cells in the plaque, which can interacte with intracellular components and metalloproteinases to significantly improvie the MR efficacy (>20 fold).[5, 6]
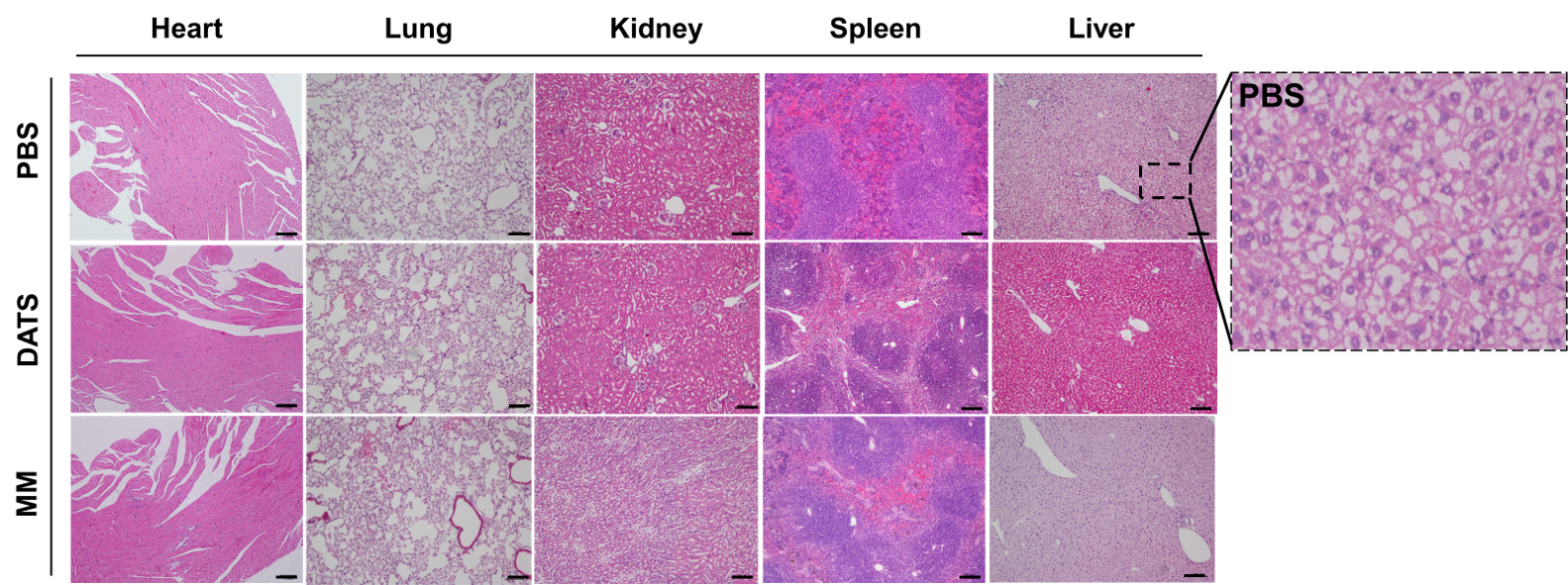
Furthermore, no apparent pathological changes were observed in the major organs (heart, spleen, lungs, or kidneys) of ApoE-/- mice after treatment with MM (Fig 3). These suggest that MM had advantageous like traditional MRI contrast agents, such as Gd-based agent, in terms of pharmacokinetics characteristics and biosafety.[7]
Conclusion
MM can reach at the target site of atherosclerotic plaque in ApoE-/- mouse model of AS and exhibited remarkable in vivo MRI monitoring of the therapeutic process with a long imaging window and good biocompatibility and biosafety. This MRI-visible nanomedicine shows immense potential as a theranostic platform for AS therapy.
Acknowledgements
None.References
- P. Libby, J. E. Buring, L. Badimon, G. K. Hansson, J. Deanfield, M. S. Bittencourt, L. Tokgozoglu, E. F. Lewis, Nat Rev Dis Primers 2019, 5 (1), 56, https://doi.org/10.1038/s41572-019-0106-z.
- W. Martinet, G. R. De Meyer, Circ Res 2009, 104 (3), 304, https://doi.org/10.1161/CIRCRESAHA.108.188318;
- Y. Chen, D. Ye, M. Wu, H. Chen, L. Zhang, J. Shi, L. Wang, Adv Mater 2014, 26 (41), 7019, https://doi.org/10.1002/adma.201402572.
- B. Ding, P. Zheng, P. Ma, J. Lin, Adv Mater 2020, 32 (10), e1905823, https://doi.org/10.1002/adma.201905823.
- W. Nordhoy, H. W. Anthonsen, M. Bruvold, H. Brurok, S. Skarra, J. Krane, P. Jynge, Magn Reson Med 2004, 52 (3), 506, https://doi.org/10.1002/mrm.20199.
- W. Nordhoy, H. W. Anthonsen, M. Bruvold, P. Jynge, J. Krane, H. Brurok, NMR Biomed 2003, 16 (2), 82, https://doi.org/10.1002/nbm.817
- E. M. Gale, H. Y. Wey, I. Ramsay, Y. F. Yen, D. E. Sosnovik, P. Caravan, Radiology 2018, 286 (3), 865, https://doi.org/10.1148/radiol.2017170977.
Figures