3367
A clinical strategy of 3.0-T non-contrast coronary MRA: a combination of diastole and systole imaging1Department of Radiology, Zhongshan Hospital, Fudan University, Shanghai, China, 2Philips Healthcare, Beijing, China, 3Philips Healthcare, Shanghai, China
Synopsis
Keywords: Vascular, Cardiovascular, coronary
Motivation: Coronary magnetic resonance angiography (MRA) has not been widely used due to lower diagnostic accuracy. The combination of diastole and systole imaging may enhance its clinical applications.
Goal(s): Designing a coronary MRA protocol combining diastole and systole imaging and evaluating its diagnostic performance for detecting significant coronary artery disease (CAD).
Approach: 3.0-T non-contrast coronary MRA was carried out twice at diastole and systole. Significant CAD was evaluated by coronary MRA as follows:1) by diastole mode, 2) by systole mode, and 3) by combined mode.
Results: Combined coronary MRA showed equally high sensitivity but improved specificity than single diastolic mode.
Impact: This study demonstrated that 1) 3.0-T non-contrast coronary MRA using combinational diastole and systole imaging can noninvasively detect CAD with high sensitivity and moderate specificity; 2) Combining diastole and systole imaging improved the diagnostic accuracy of coronary MRA, especially specificity.
Introduction
Coronary magnetic resonance angiography (MRA) is a safe, non-invasive, radiation and iodinated contrast-free potential alternative for imaging coronary artery stenosis. Still, it has yet to be widely used in clinical practice (1) due to lower diagnostic accuracy than coronary computed tomography angiography (CTA) (2,3). There are two relatively quiescent periods in the cardiac cycle, mid-diastole, and end-systole, for acquiring coronary images (4). The clinical applications of coronary MRA combining diastole and systole imaging have never been described comprehensively in coronary artery disease (CAD) patients. We aimed to design an optimal non-contrast coronary MRA scan protocol combining diastole and systole imaging and to evaluate its diagnostic performance for detecting significant CAD.Methods
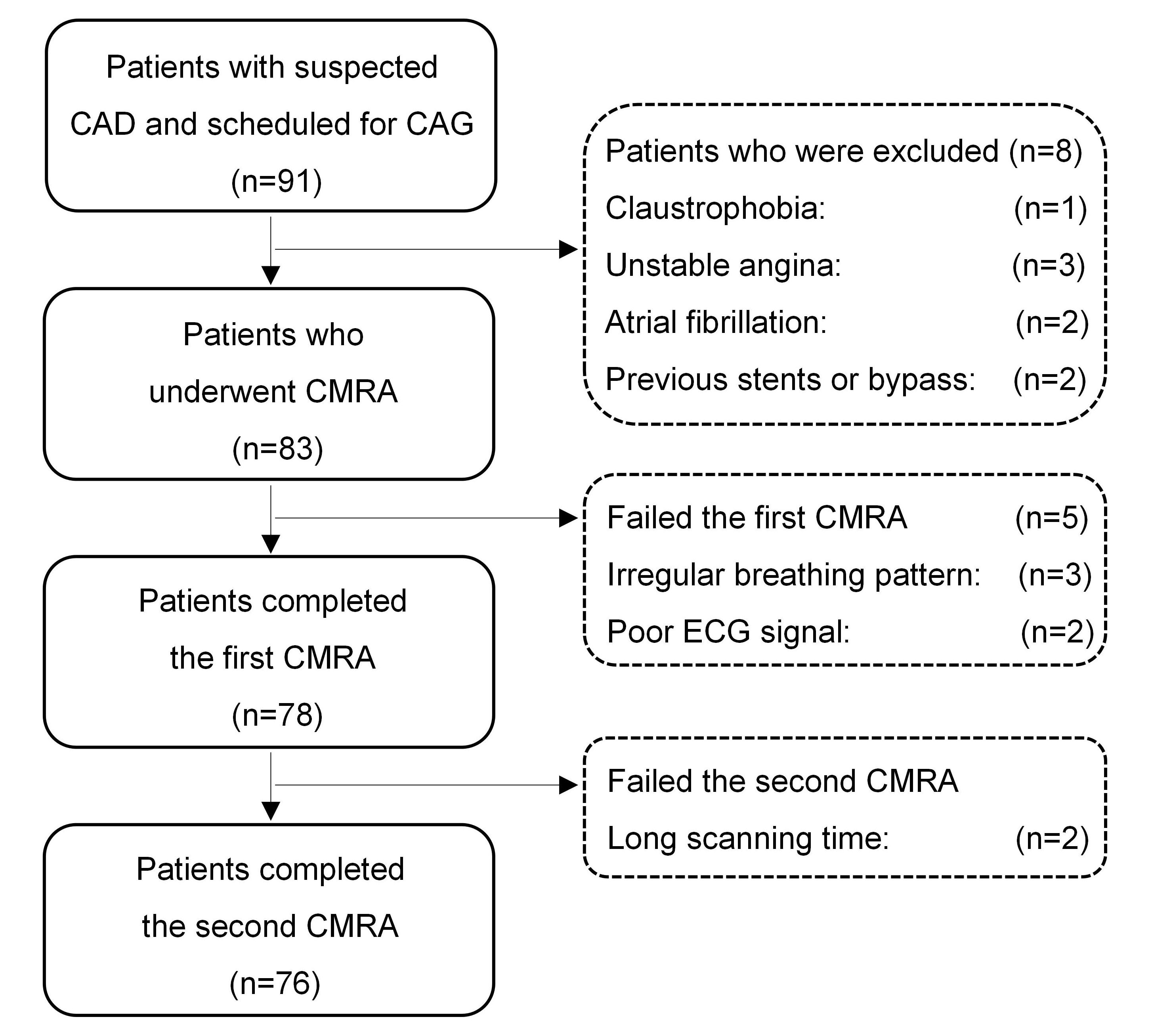
In this prospective study, 91 patients scheduled for CAG were enrolled for coronary MRA. 3.0-T (Ingenia CX, Netherland, Best) non-contrast whole-heart coronary MRA was carried out twice at diastole and systole. Two radiologists who were blinded to the CAG results assessed the images independently. The image quality of each coronary artery segment was rated on the following four-point scale: 1 = poor, non-assessable with severe image artifacts; 2 = fair, assessable with moderate image artifacts; 3 = good, assessable with minor artifacts; and 4 = excellent, assessable with no apparent artifacts. Scores of the two observers were averaged for image quality analysis. Significant coronary stenosis was defined as a luminal diameter reduction of ≥ 50% using CAG as the reference and was evaluated as follows:1) by coronary MRA at diastole alone; 2) by coronary MRA at systole alone 3) by combined coronary MRA (diastole and systole images). For combined coronary MRA analysis, only location-matched stenosis presented in both modes was determined to be significant. Otherwise, it was defined as having no significant stenosis. Consensus reading was performed for the segments with disagreement between the two observers.Results
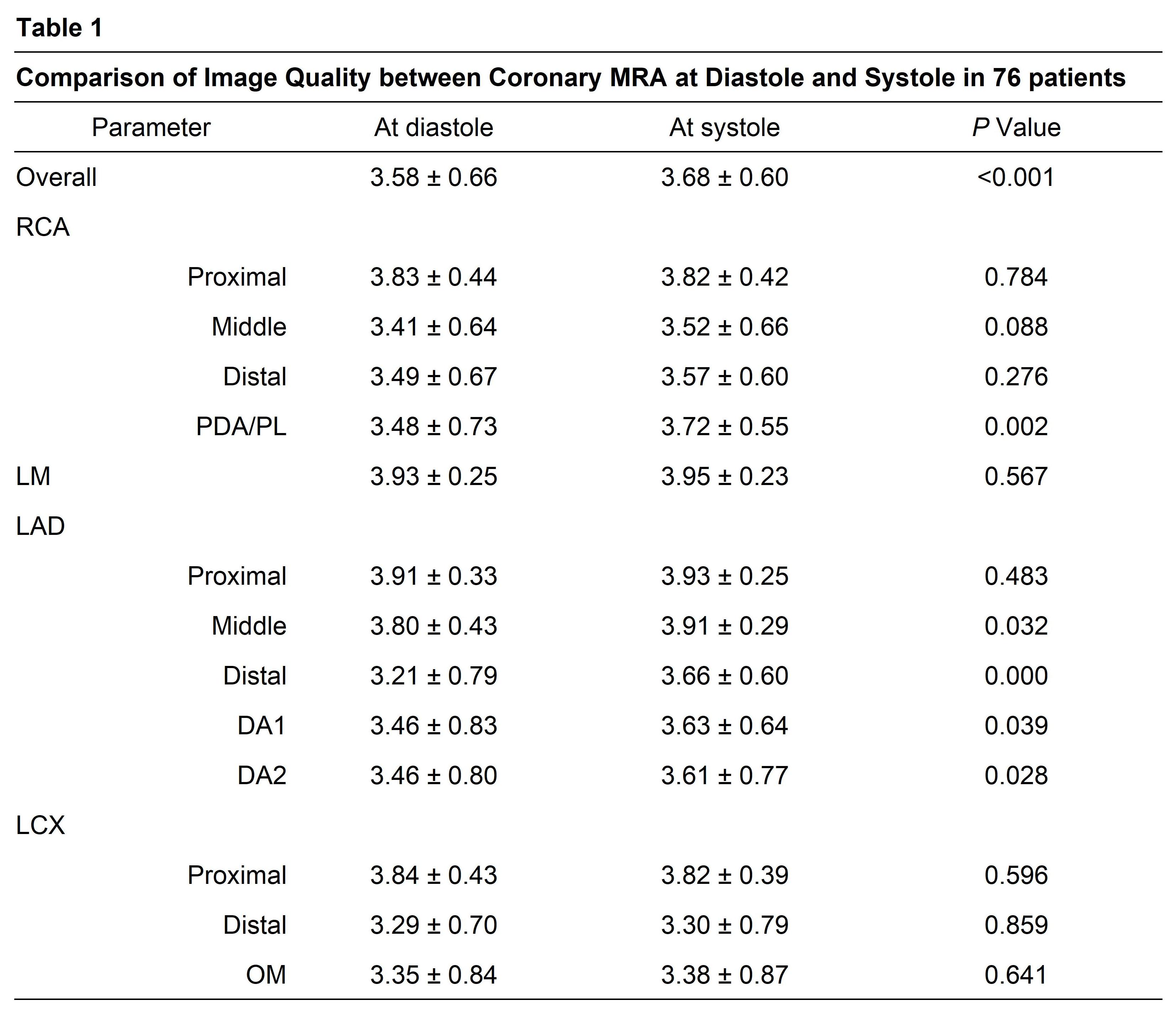
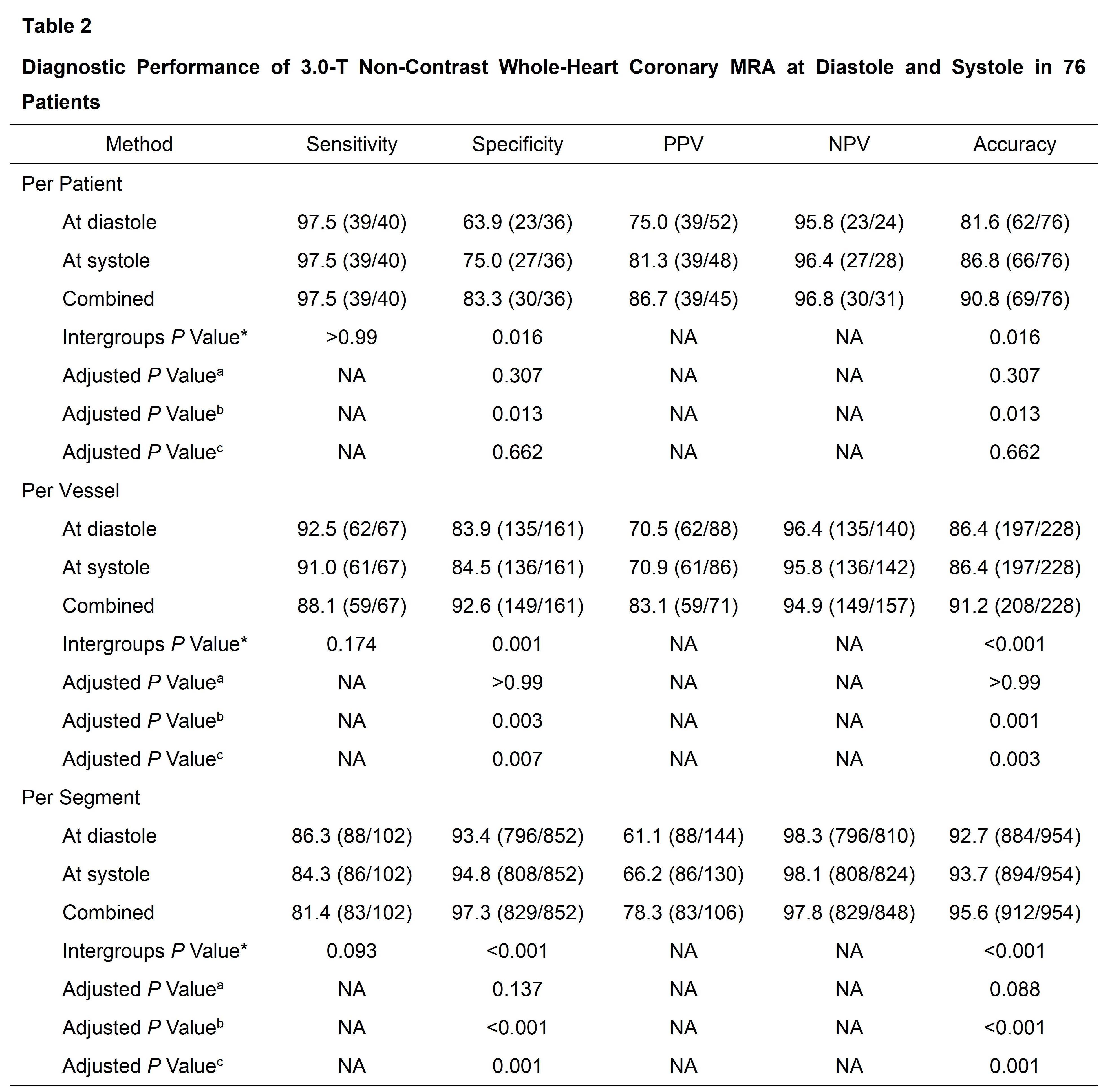
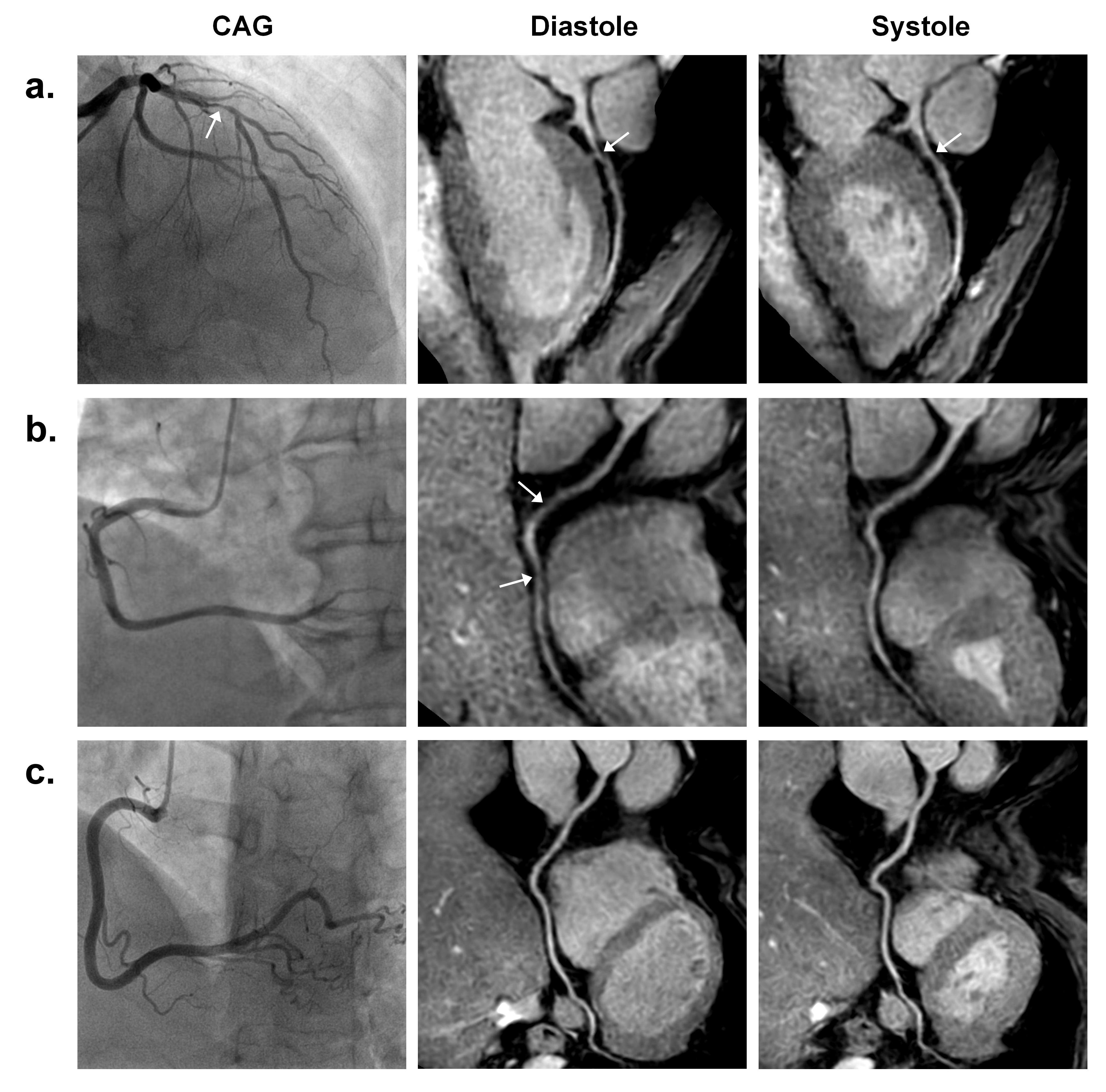
The study participants' inclusion flowchart is shown in Figure 1. The diastolic and systolic coronary MRA was completed in 76 patients. The total time of two coronary MRA scanning was 16.2 ± 3.1 min, and acquisition time was longer at systole than at diastole (8.9 ± 2.1 min vs. 7.3 ± 1.6 min, P < 0.001). The comparison of image quality between diastolic and systolic coronary MRA is shown in Figure 2 - Table 1. The overall image quality at systole was higher than at diastole (P < 0.001), particularly in middle-distal segments.The diagnostic performance of coronary MRA for detecting significant coronary stenoses using the three strategies is listed in Figure 3 -Table 2. For the three coronary MRA strategies (diastolic, systolic, and combined), there was no significant difference in sensitivity on a per-patient, per-vessel, and per-segment basis (P > 0.05 for all). At the same time, the specificity and accuracy were significantly different on a per-patient, per-vessel, and per-segment basis (P < 0.05 for all). Compared with diastolic coronary MRA, systolic coronary MRA had similar specificity and accuracy on a per-patient, per-vessel, and per-segment basis (adjusted P > 0.05 for all). Compared with diastolic coronary MRA, combined coronary MRA had significantly higher specificity and accuracy on a per-patient, per-vessel, and per-segment basis (adjusted P < 0.05 for all). Figure 4 illustrates the diagnostic performance of coronary MRA combining diastole and systole.Discussion
This study found that systole imaging offered better image quality in middle-distal segments. However, the mean imaging time of coronary MRA was longer at systole than diastole. We showed higher sensitivity but relatively lower specificity by the diastole or systole mode alone, with no significant difference between diastole and systole. Compared with diastole, the duration of systole is less affected by HR variability (5). End-systolic imaging may be an alternative to more conventional diastolic imaging to minimize the adverse effects of RR variability. However, the abbreviated systolic rest period necessitates image data collection in a relatively short acquisition window, which prolongs scanning time. The long acquisition time increases the chance of respiratory pattern and drift bulk motion and degrades the final image quality. Therefore, both methods have advantages and disadvantages and could be helpful for clinical applications of coronary MRA. In our study, when diastole and systole images were combined, more false positive interpretations for poor image quality and ambiguous local artifacts were corrected, enhancing diagnostic specificity.Conclusion
3.0-T non-contrast coronary MRA at diastole or systole can noninvasively detect coronary stenoses with high sensitivity and moderate specificity. Combined coronary MRA at 3.0-T significantly improved diagnostic performance, especially specificity, compared with single-phase coronary MRA mode.Acknowledgements
The authors thank the members of the Center of Cardiac Magnetic Resonance team at the Zhongshan Hospital Affiliated to Fudan University and the MR technologists for their valuable participation, helpfulness, and support during this study.References
1. American College of Cardiology Foundation Task Force on Expert Consensus Documents, Hundley WG, Bluemke DA, et al. ACCF/ACR/AHA/NASCI/SCMR 2010 expert consensus document on cardiovascular magnetic resonance: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. J Am Coll Cardiol. 2010;55(23):2614–2662.2. Di Leo G, Fisci E, Secchi F et al. Diagnostic accuracy of magnetic resonance angiography for detection of coronary artery disease: a systematic review and meta-analysis. Eur Radiol. 2016;26(10):3706–3718.3. Pouleur AC, le Polain de Waroux JB, Kefer J, et al. Direct comparison of whole-heart navigator-gated magnetic resonance coronary angiography and 40- and 64-slice multidetector row computed tomography to detect coronary artery stenosis in patients scheduled for conventional coronary angiography. Circ Cardiovasc Imaging. 2008;1(2):114–121.4. Johnson KR, Patel SJ, Whigham A, et al. Three-dimensional, time-resolved motion of the coronary arteries. J Cardiovasc Magn Reson. 2004;6(3):663–773.5. Gharib AM, Herzka DA, Ustun AO, et al. Coronary MR angiography at 3T during diastole and systole. J Magn Reson Imaging. 2007;26(4):921-926.Figures