3365
Efficient native MRA at 0.55T using motion-correction1Siemens Healthineers, Erlangen, Germany, 2Physikalisch - Technische Bundesanstalt (PTB), Braunschweig and Berlin, Germany
Synopsis
Keywords: Vascular, Cardiovascular
Motivation: MRI at 0.55T with an 80cm bore has allowed improved access to CMR for patients. The application of robust native whole-thorax MRA at low-field remains limited especially due to the challenge of respiratory motion.
Goal(s): To develop a large field-of-view, whole-thorax, self-gated and breathing-motion corrected native MRA with a predictable scan time and efficient data usage at 0.55T.
Approach: An optimized sampling pattern is used with T2-prep, dual-echo Dixon and non-rigid motion correction is developed.
Results: The approach was successfully applied in-vivo and shows successful mitigation of motion artefacts and blurring and good separation of water and fat in the entire thoracic region.
Impact: Proof of the viability of self-gated MOCO MRA at 0.55T.
Introduction
Cardiac MRI at 0.55T with an 80cm bore size holds promise to improve accessibility (1). Although having several advantages such as improved B0-homogeneity or lower SAR, several challenges need to be tackled including the intrinsic lower SNR as well as the spectral vicinity of water and fat which makes fat suppression techniques challenging. Here, we propose a novel research sequence tailored to 0.55T that covers the entire thorax with high spatial resolution, runs with a predictable scan time and uses 100% of the data by performing non-rigid respiratory motion correction based on a self-gating signal.Methods
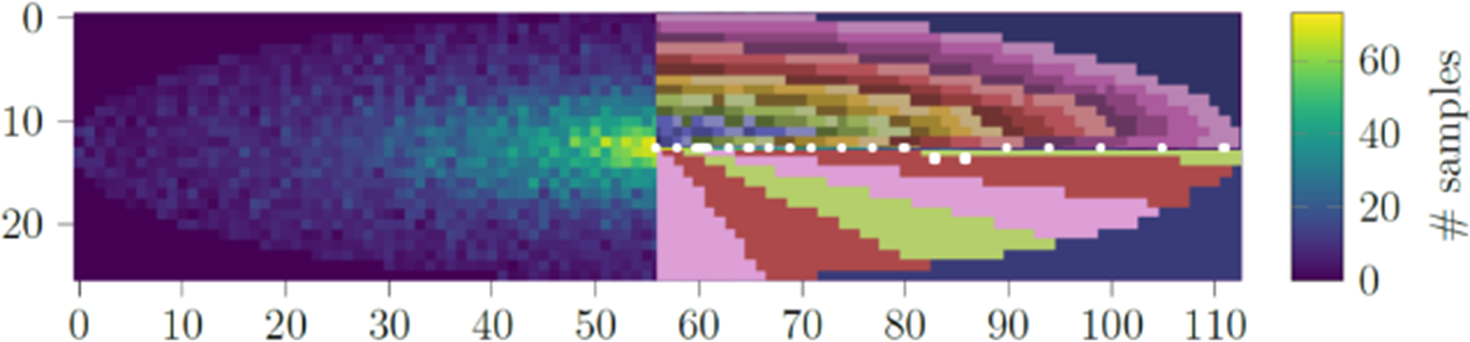
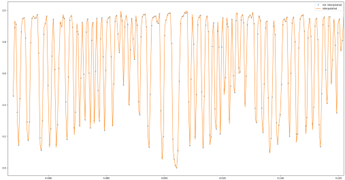
The research sequence was ECG-triggered during diastole with an acquisition window of 181ms. A T2prep module (50ms) was used for blood/myocardium contrast enhancement and a two-point Dixon approach was implemented for water/fat separation (TE=2.77/6.47 ms). The FoV was 450x450x120mm with an acquired isotropic resolution of 1.5mm3. The cartesian sampling pattern consisted of multiple overlayed Poisson disc patterns with cropped corners and a partial Fourier factor of 87.5% in y and z. The points were then divided w.r.t. angle (20 bins) and normalized radius (24 bins). During each ECG cycle the central k-space point (ky=kz=0) followed by 24 points are sampled within one angular bin. Sampling is performed in a pseudo-radial out-in fashion (fig. 1). In the next acquisition window, the angular bin is rotated by the golden angle. Total acquisition time was 13:05 min. The central k-space line acquired during each ECG cycle is extracted from the first echo and used as a surrogate signal for respiratory motion after PCA along the temporal and coil dimensions (fig. 2). A total number of 6 respiratory bins were then reconstructed with 10% data sharing using a temporally and spatially TV regularized CG-SENSE algorithm (2). 3D motion fields were then calculated using MIRTK (3) on the respiratory-resolved images of the first echo. Motion fields were then incorporated into a spatially TV-regularized CG-SENSE reconstruction. Both echo images were reconstructed using the same motion fields. Finally, a Graph-Cut based Dixon algorithm (4) was applied to separate water and fat images. The proposed technique was applied in a healthy volunteer on a 0.55T system (MAGNETOM Free.Max, Siemens Healthcare AG, Erlangen, Germany) using two body array coils (12-channel anterior & 6-channel posterior) and the results compared to a reconstruction without motion compensation.Results and Discussion
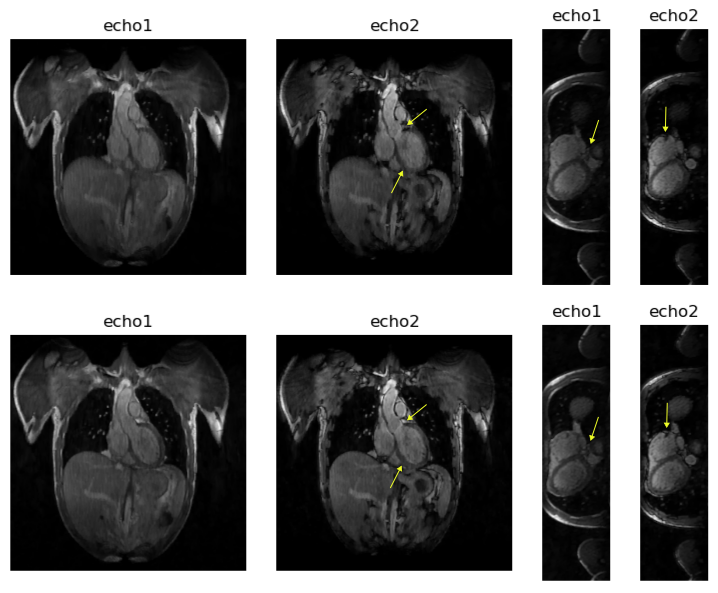
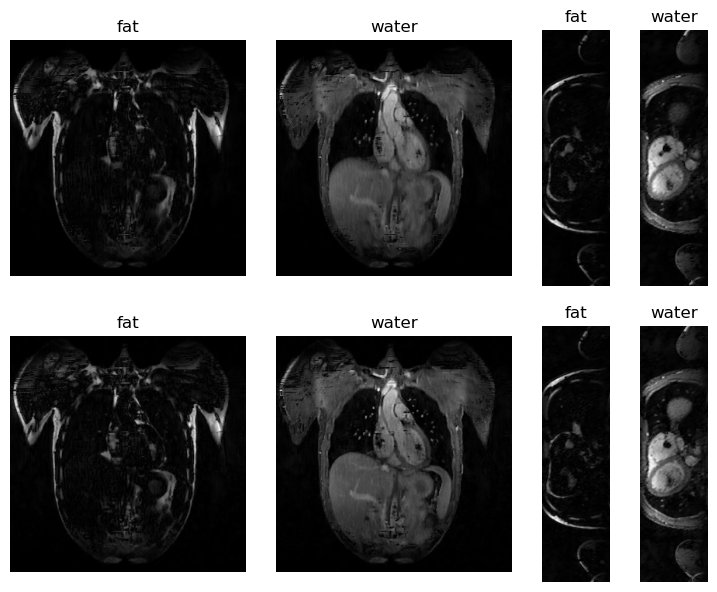
In fig. 3, the computed motion fields are visualized during the respiratory resolved image series. The corresponding inverse application of the motion fields (right) demonstrates the successful correction of the respiratory-induced motion in the heart and its surrounding vessels as well as in the abdominal region. This is shown only to demonstrate the quality of the obtained motion fields. For the final reconstruction, the motion fields were included in the reconstruction. In fig. 4, both echoes are shown for the uncorrected (top) and the proposed motion-corrected (bottom) approach. A reduction of motion artefacts as well as increased overall sharpness is observed using the proposed method. In fig. 5 the water and fat images are displayed for the two methods. An overall successful separation can be observed as well as a clearly improved image quality when using the proposed method. The remaining local swaps are currently under investigation and can potentially be attributed to blood flow during the acquisition window. Future investigation will therefore include optimizing the triggering delay, decreasing the acquisition window to mitigate phase shifts due to blood flow and the use of a three-point Dixon acquisition to improve robustness of the unfolding process. As the acquisition time of 13:05 minutes might not always be acceptable, a stronger acceleration factor is warranted in the future.Conclusion
We successfully present a native MRA that covers the entire thorax with an isotropic resolution of 1.5mm3 at 0.55T. It runs during free breathing, has a predictable scan time and makes use of all of the acquired data by successfully performing non-rigid motion correction.Acknowledgements
Funded by the German Research Foundation (GRK2260, BIOQIC). The project (22HLT02 A4IM) has received funding from the European Partnership on Metrology, co-financed from the European Union’s Horizon Europe Research and Innovation Programme and by the Participating States.References
1. Varghese J, et al. Building a comprehensive cardiovascular magnetic resonance exam on a commercial 0.55 T system: A pictorial essay on potential applications. Front Cardiovasc Med. 2023 Mar 1;10:1120982. doi: 10.3389/fcvm.2023.1120982. PMID: 36937932; PMCID: PMC10014600.
2. Mayer J, Blaszczyk E, Cipriani A, Ferrazzi G, Schulz-Menger J, Schaeffter T, Kolbitsch C. Cardio-respiratory motion-corrected 3D cardiac water-fat MRI using model-based image reconstruction. Magn Reson Med. 2022 Oct;88(4):1561-1574. doi: 10.1002/mrm.29284. Epub 2022 Jul 1. PMID: 35775790.
3. Rueckert D, et al. Nonrigid registration using free-form deformations: application to breast MR images. IEEE transactions on medical imaging 18.8 (1999): 712-721.
4. Hernando D, Kellman P, Haldar JP, Liang ZP. Robust water/fat separation in the presence of large field inhomogeneities using a graph cut algorithm. Magn Reson Med. 2010 Jan;63(1):79-90. doi: 10.1002/mrm.22177. PMID: 19859956; PMCID: PMC3414226.
Figures