3361
Comparison of iNAV-based Free-Breathing Non-Contrast Coronary Magnetic Resonance Angiography Acquired at 0.7mm3 and 0.9mm3 Resolution1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2Department of Cardiology, Aarhus University Hospital, Aarhus, Denmark, 3Department of Clinical Medicine, Aarhus University, Aarhus, Denmark, 4MR Research Collaborations, Siemens Healthcare Limited, Camberley, United Kingdom, 5School of Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile, 6Institute for Biological and Medical Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile
Synopsis
Keywords: Atherosclerosis, Atherosclerosis, Angiography, whole-heart
Motivation: Coronary artery disease remains a significant problem worldwide and current methods for anatomical assessment involve ionising radiation and iodinated contrast agents.
Goal(s): To develop a novel free-breathing, 3D whole-heart, coronary magnetic resonance angiography sequence with high spatial resolution for the assessment of coronary anatomy and coronary artery disease.
Approach: Nine patients referred for assessment of suspected coronary artery disease were scanned using the proposed sequence at 1.5T. Acquisitions at 0.9mm3 and 0.7mm3 were compared.
Results: The 0.7mm3 acquisition demonstrated improved qualitative and semi-quantitative vessel visualisation and coronary stenosis detection compared with 0.9mm3 acquisition in an average scan time of <14 minutes.
Impact: This work demonstrates improved coronary artery lumen visualisation and stenosis detection compared to 0.9mm3 acquisitions, providing a further step forward towards clinical adoption as a contrast- and radiation-free alternative to CTCA.
Introduction
Coronary artery disease (CAD) remains the leading cause of morbidity and mortality in the developed world. While computed tomography coronary angiography (CTCA) with a spatial resolution of approximately 0.6mm remains the gold standard in both American1 and European2 guidelines for non-invasive anatomical assessment of coronary arteries and CAD. However, it involves ionising radiation and the use of iodinated contrast agents. In contrast, coronary magnetic resonance angiography (CMRA) offers a promising radiation- and contrast-free alternative. However, clinical adoption has been hampered by challenges such as low spatial resolution, prolonged and unpredictable scan durations, and susceptibility to motion artefacts.3 Recent advancements have demonstrated high-resolution CMRA acquired at 0.9mm3 with a clinically feasible and predictable scan time of approximately 10 minutes.4 This study aims to further push the boundaries by achieving free-breathing, motion-compensated CMRA with 0.7mm³ spatial resolution and assess its feasibility, image quality and CAD detection when compared to 0.9mm3 resolution acquisitions in patients with suspected CAD.Methods
Individuals referred for suspected CAD evaluation were enrolled in the study. An ECG-triggered, free-breathing, 3D whole-heart, balanced steady-state free precession (bSSFP) research sequence with an undersampled 3D variable density spiral-like Cartesian trajectory with golden-angle rotation was utilised5. Low-resolution 2D image navigators (iNAV)6 were incorporated into the sequence to enable 100% respiratory scan efficiency with predictable scan times (Figure 1). Preceding image acquisition, a spectral presaturation with inversion recovery (SPIR) fat-saturation pulse with a flip-angle (FA) of 130 ° was used to null epicardial fat and thereby improve coronary visualisation. A T2 preparation pulse of duration 40ms was used to enhance the contrast between blood and cardiac muscle. Patient preparation involved sublingual nitrates for coronary dilatation and oral +/- intravenous beta-blockers to achieve a target resting heart rate of 50-60 beats-per-minute (bpm). The acquisition window was defined by the diastolic rest period of the right coronary artery (RCA). Imaging was performed using a 1.5T MRI scanner (MAGNETOM Sola, Siemens Healthineers, Erlangen, Germany) with the following parameters: coronal orientation, isotropic spatial resolution= 0.7mm³, bandwidth= 723 Hz/Px, and 4.5x acceleration. Images were reconstructed using a 3-part framework; 1) beat-to-beat respiratory binning and intra-bin translational motion correction, 2) bin-to-bin 3D non-rigid motion estimation, and 3) non-rigid motion-corrected 3D patch-based low-rank denoising (PROST).7 Both 0.9mm3and 0.7mm3 datasets were Fourier interpolated to a final resolution of 0.6mm3. Image analysis and multiplanar reconstruction was performed using cvi42 software (Circle Cardiovascular Imaging Inc., Calgary, Alberta, Canada) and quantitative analysis of vessel sharpness and vessel length was performed using dedicated research software; “Soap-Bubble”.8Results
Nine patients were successfully scanned utilising the described CMRA technique. The average heart rate was 60 bpm, and all were in sinus rhythm. The average scan time for the 0.9mm3 acquisition and 0.7mm3 acquisition was 8 minutes 14 seconds and 13 minutes 42 seconds respectively. Both acquisitions provided clear visualisation of the proximal and mid portions of all three coronary arteries (Figure 2). There was improved depiction of the distal coronary segments with the 0.7mm3 vs 0.9mm3 acquisition leading to improved vessel length measurements (mean 140mm vs 124mm) respectively. Visual assessment of vessel sharpness and depiction of coronary stenosis (Figure 3) was improved by the 0.7mm3 acquisition. Quantitative vessel sharpness assessment calculated as the mean of the left and right edge signal intensity divided by the signal intensity at the centre of the vessel was similar (46%) for the two acquisitions.Discussion
This study demonstrates CMRA at 0.7mm3 isotropic spatial resolution with a predictable feasible scan time. Image quality and stenosis detection, as assessed by both qualitative and semi-quantitative measures, was improved by the 0.7mm3 acquisition compared to the 0.9mm3. Future research will focus on expanding the patient cohort to evaluate the efficacy of this high resolution in detecting clinically significant coronary stenosis in different vessel locations. If successful, CMRA may provide a radiation and contrast agent-free alternative to CTCA and enter routine clinical adoption.Acknowledgements
The authors acknowledge financial support from: (1) King’s BHF Centre for Award Excellence RE/18/2/34213, BHF PG/18/59/33955, RG/20/1/34802 and FS/CRTF/20/24011 (2) EPSRC EP/V044087/1, EP/P001009/1, EP/P032311/1, EP/P007619, (3) Wellcome EPSRC Centre for Medical Engineering (NS/A000049/1), (4) Millennium Institute for Intelligent Healthcare Engineering ICN2021_004, FONDECYT 1210637 and 1210638, (5) IMPACT, Center of Interventional Medicine for Precision and Advanced Cellular Therapy, Santiago, Chile. ANID—Basal funding for Scientific and Technological Center of Excellence, IMPACT, #FB210024 (6) the Department of Health through the National Institute for Health Research (NIHR) comprehensive Biomedical Research Centre award, (7) NIHR Cardiovascular MedTech Co-operative and (8) the Technical University of Munich – Institute for Advanced Study. The views expressed are those of the authors and not necessarily those of the BHF, NHS, the NIHR or the Department of Health.
References
1. Gulati M, Levy PD, Mukherjee D, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;144(22). doi:10.1161/cir.0000000000001029
2. Knuuti J, Wijns W, Saraste A, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41(3):407-477. doi:10.1093/eurheartj/ehz425
3. Danias PG, Stuber M, Botnar RM, Kissinger K V, Edelman RR, Manning WJ. Relationship between motion of coronary arteries and diaphragm during free breathing: lessons from real-time MR imaging. American Journal of Roentgenology. 1999;172(4):1061-1065. doi:10.2214/ajr.172.4.10587147
4. Hajhosseiny R, Rashid I, Bustin A, et al. Clinical comparison of sub-mm high-resolution non-contrast coronary CMR angiography against coronary CT angiography in patients with low-intermediate risk of coronary artery disease: a single center trial. Journal of Cardiovascular Magnetic Resonance. 2021;23(1):57. doi:10.1186/s12968-021-00758-9
5. Prieto C, Doneva M, Usman M, et al. Highly efficient respiratory motion compensated free-breathing coronary mra using golden-step Cartesian acquisition. Journal of Magnetic Resonance Imaging. 2015;41(3):738-746. doi:https://doi.org/10.1002/jmri.24602
6. Luo J, Addy NO, Ingle RR, et al. Nonrigid Motion Correction With 3D Image-Based Navigators for Coronary MR Angiography. Magn Reson Med. 2017;77(5):1884-1893. doi:https://doi.org/10.1002/mrm.26273
7. Bustin A, Lima da Cruz G, Jaubert O, Lopez K, Botnar RM, Prieto C. High-dimensionality undersampled patch-based reconstruction (HD-PROST) for accelerated multi-contrast MRI. Magn Reson Med. 2019;81(6):3705-3719. doi:https://doi.org/10.1002/mrm.27694
8. Etienne A, Botnar RM, van Muiswinkel AMC, Boesiger P, Manning WJ, Stuber M. “Soap-Bubble” visualization and quantitative analysis of 3D coronary magnetic resonance angiograms. Magn Reson Med. 2002;48(4):658-666. doi:https://doi.org/10.1002/mrm.10253
Figures
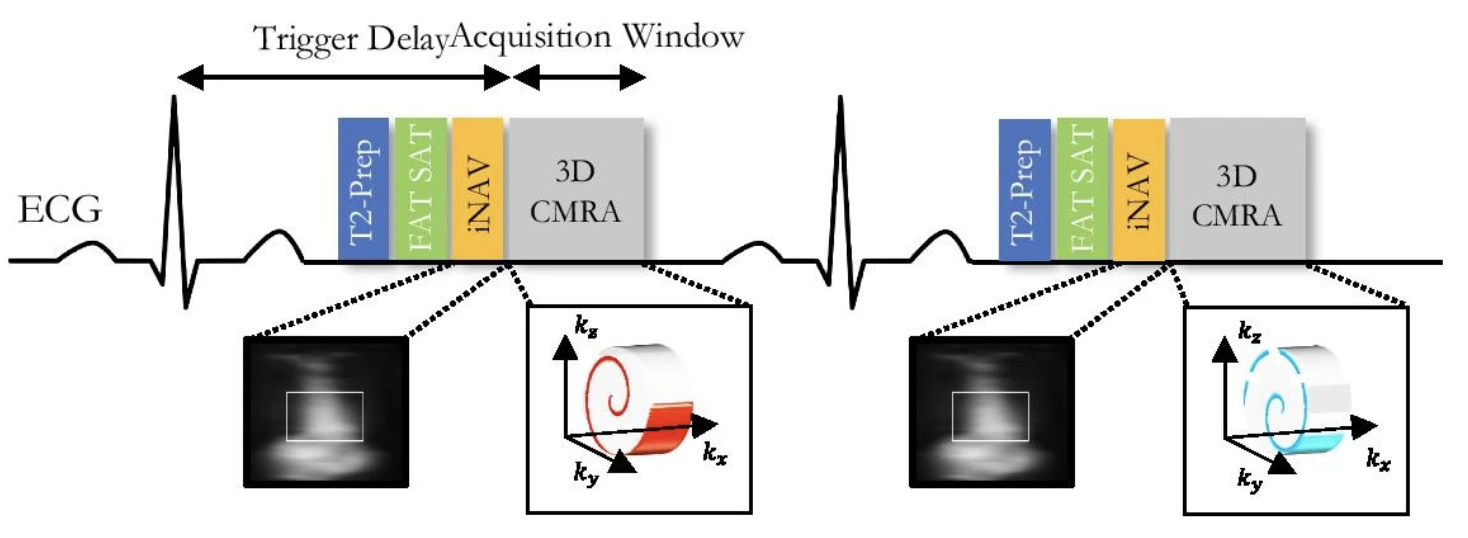
Framework for the 3D whole heart CMRA acquisition: an under-sampled 3D variable density spiral-like Cartesian trajectory with golden angle between spiral-like interleaves (VD-CASPR), preceded by 2D image navigators (iNAV) to allow for 100% scan efficiency and beat-to-beat translational respiratory-induced motion correction of the heart.
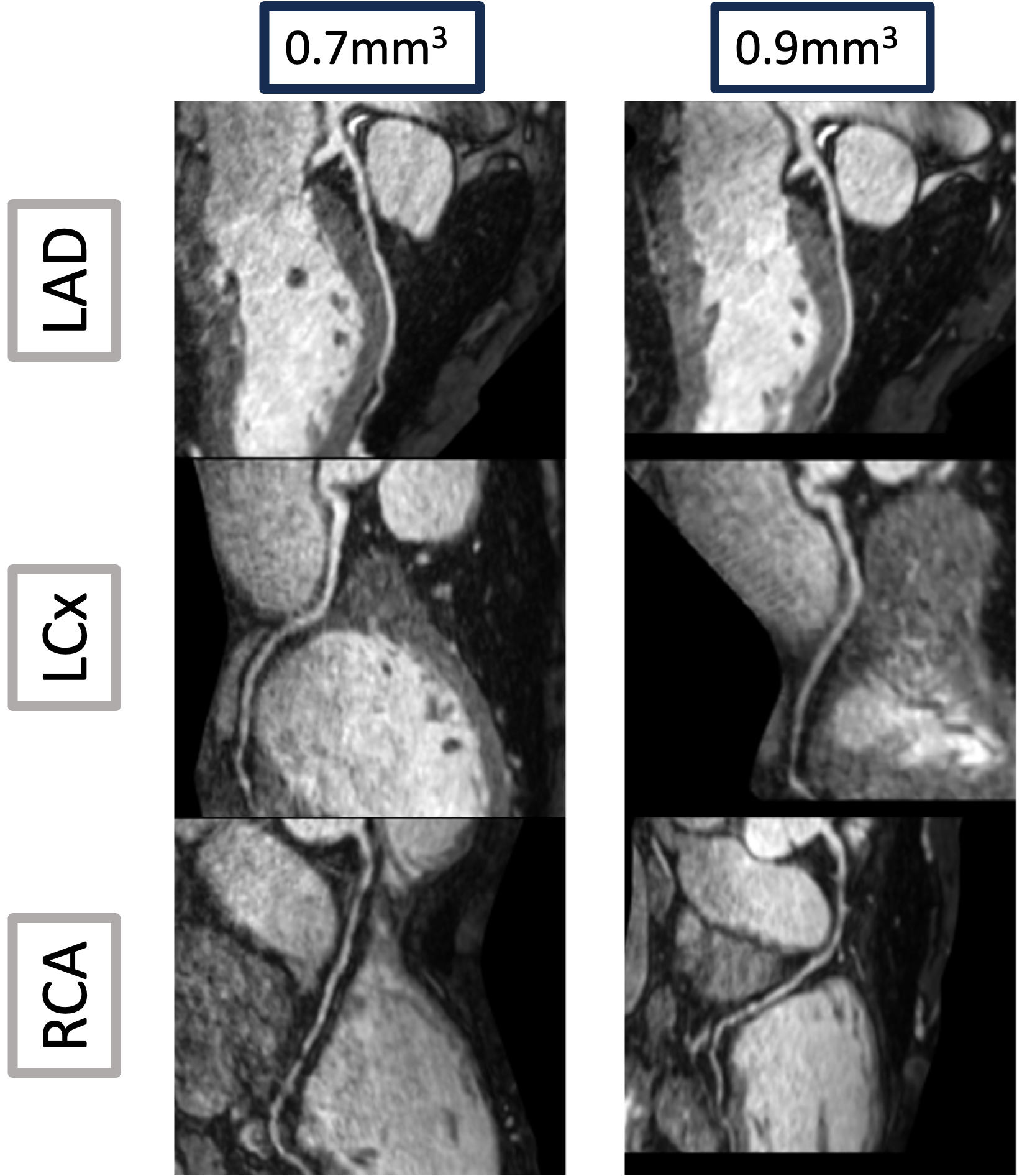
Reformatted 2D view of coronary arteries in a patient with suspected CAD acquired at 0.7mm3 (left) and 0.9mm3 (right) without contrast agent. Left anterior descending (LAD), left circumflex (LCx) and right coronary artery (RCA).
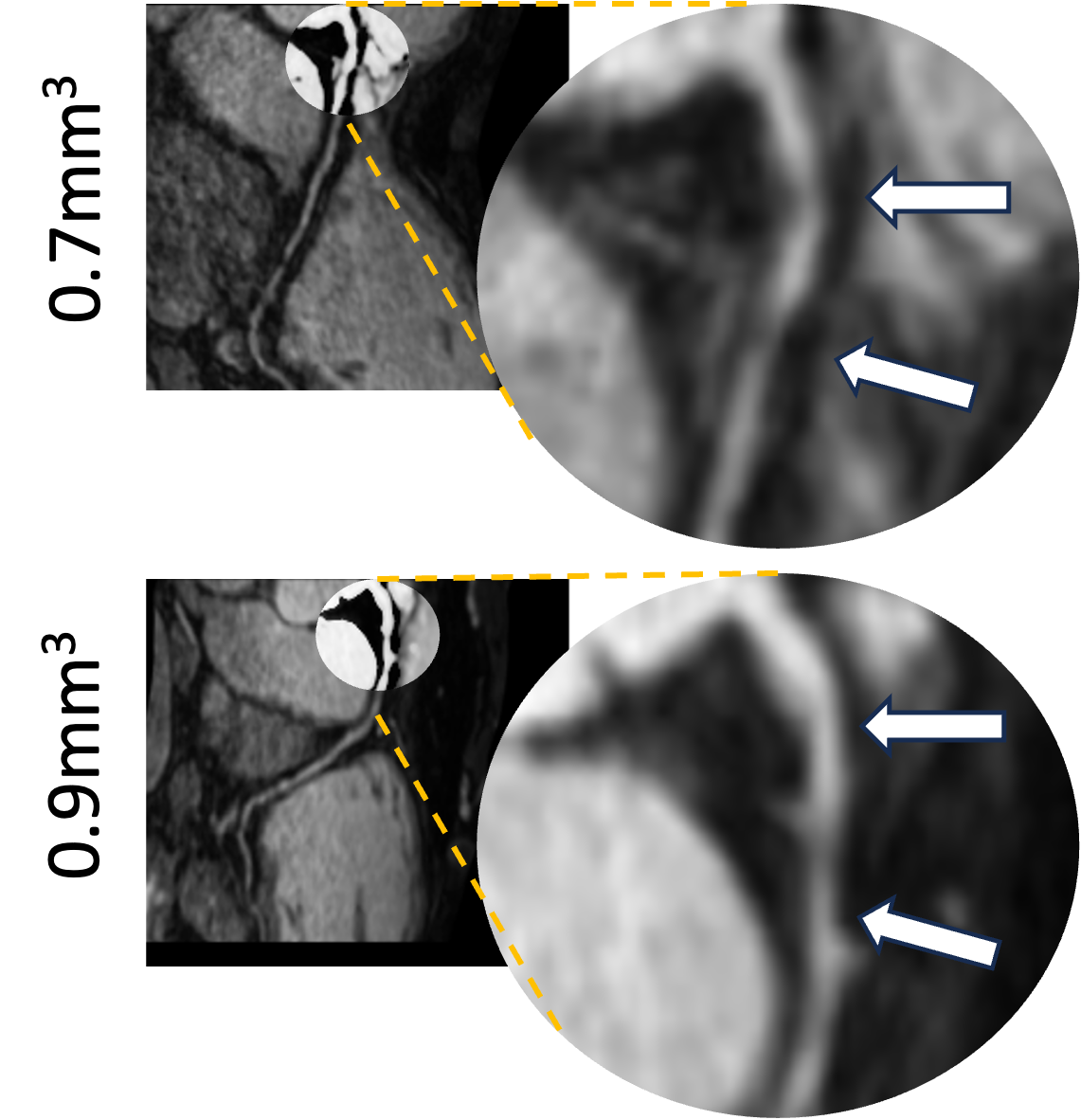
Reformatted images of the RCA in a single patient with CAD. Tandem lesions are depicted in the proximal vessel (white arrows) and demonstrate improved visualisation of stenosis at 0.7mm3 (top) acquisition compared to 0.9mm3 (bottom).