3359
GRASP-MRA: Ultra-high temporal resolution 3D-cine MRI of pulsatile aneurysmal motion at 7T1Graduate School of Medicine, Kyoto University, Kyoto, Japan, 2University of Queensland, Brisbane, Australia
Synopsis
Keywords: Vessel Wall, Vessels, GRASP, MRA
Motivation: The mortality and disability rates following cerebral aneurysm rupture remain significantly high. Recently, pulsation of aneurysms has been suggested as a novel risk factor of rupture.
Goal(s): To harness the ultra-high temporal resolution and signal-to-noise ratio of the modified GRASP technique with 7T MRI to visualize pulsatile motions of cerebral aneurysms.
Approach: A pulsatile aneurysm phantom and aneurysm patient were scanned using a 3D-cine MRI technique, aiming to capture dynamic aneurysmal wall movements at high spatial and ultra-high temporal resolution.
Results: The new imaging technique successfully depicted pulsatile movements in the aneurysm phantom and subject, suggesting a novel predictor for aneurysm rupture.
Impact: This study presents a 3D-cine MRI method at 7T, capturing aneurysm pulsations with ultra-high frame rates in the tens of milliseconds range, promising to refine rupture risk assessments and potentially reducing adverse outcomes in cerebral aneurysm management.
INTRODUCTION
The fatality rates for ruptured intracranial aneurysms (IAs) range between 35-50%, with up to half of those who survive experiencing long-term disabilities1. While preventative measures such as clipping and coiling are generally effective, they come with a significant risk of negative neurological outcomes—about 10%, which is substantially higher than the average 5-year risk of an IA rupturing, estimated at 3.4%. Further complicating matters, recent retrospective studies have revealed a greater incidence of small ruptured IAs than previously understood, underscoring the need for better predictors of rupture risk. The pulsation of IAs has emerged as a potential new indicator particularly with 4D CTA (CT angiography) studies1,2. Our study seeks to leverage the high signal-to-noise ratio of 7T MRI with an imaging technique we denote as “GRASP-MRA”, which builds on GRASP (Golden-Angle Radial Sparse Parallel)3, a relatively novel MRI technique that utilizes radial sampling and compressed sensing. We aim to capture the pulsation of IAs as a 3D-cine image at frame rates that can be retrospectively and arbitrarily determined, potentially up to an ultra-high, 100 frames per second.METHODS
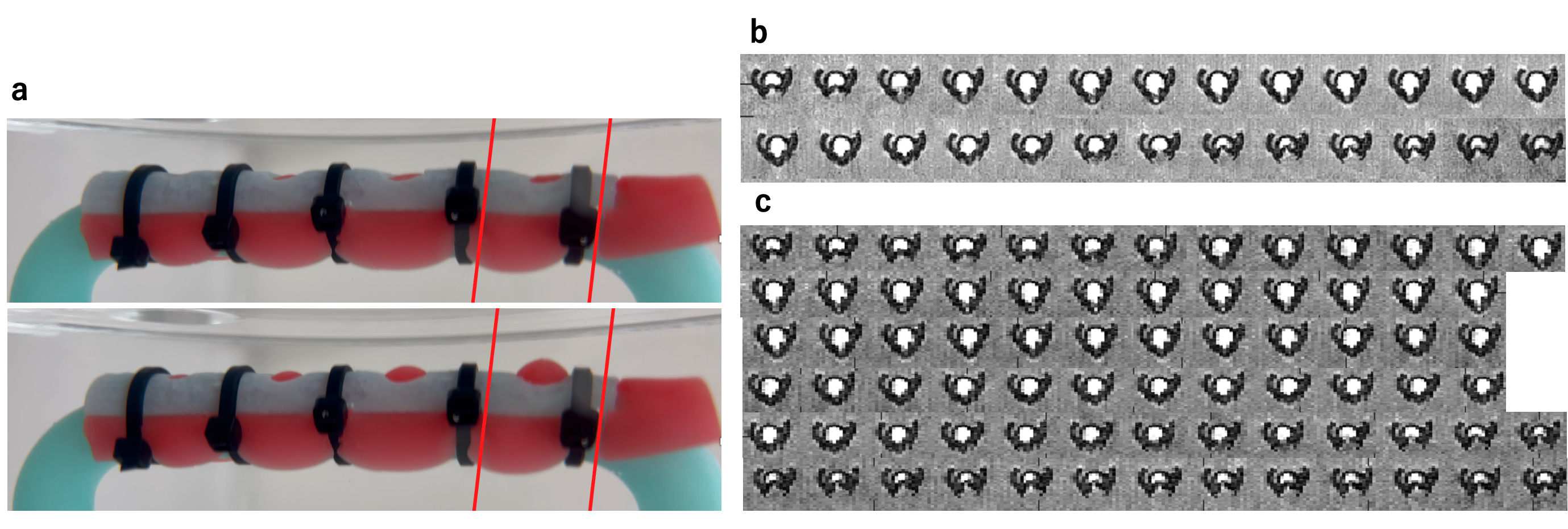
To test and develop our MRI technique which we call “GRASP-MRA”, a pulsating phantom was first constructed of a rigid tubular structure with a 4mm hole sealed by a highly elastic rubber tube (Figure 1). The phantom was housed in an MRI-compatible acrylic case, which was connected to a pulsatile flow pump and controller (Alpha Flow SP-1, Alpha FC PR-1, Fuyo Corporation, Japan) with a tube filled with water and Gadolinium (2.5mmol/L) to simulate the pulsation of an aneurysm (Figure 1). The pulsating phantom was scanned with an in-house golden-angle radial gradient echo stack-of-stars 3D MRI sequence (TR/TE = 13/6.6 ms, FA = 12 deg, resolution = 320 x 320 x 22, spatial resolution = 0.5 mm isotropic, FOV = 160 x 160 x 11 mm, radial spokes = 2000, scan time = 9m32s, angle increment = 137.51 deg, with flow compensation) on a 7T MRI scanner (MAGNETOM 7T, Siemens Healthineers, Germany) with a 32-channel receiver head coil (Nova Medical, USA). The acquired k-space data was synchronized with the ECG signal output from the pulsatile pump (set to 60 beats per minutes) and binned in units of readouts into 26 and 75 time phases per pulse.A 74-year-old male patient with a 3mm IA in the M2 segment of the left middle cerebral artery was scanned with the same MRI sequence and parameters as the phantom study with some modifications (FA = 20 deg, radial spokes = 6000, scan time = 28m36s). The acquired data was binned into 72 time phases per pulse, respectively, by synchronization with the data from the pulse oximeter worn on the patient’s finger.
In both scans, the acquired k-space data were subject to preprocessing steps that included coil compression, gradient delay correction, and coil streaking artifact reduction. The data was then reconstructed into 4D volumes (i.e., 3D volume of each time phase) by utilizing 3D-NUFFT (non-uniform fast Fourier transform) and a compressed sensing algorithm using FISTA (Fast Iterative Shrinkage-Thresholding Algorithm) as its solver which exploits the sparsity of the total variation between neighboring time phase volumes4.
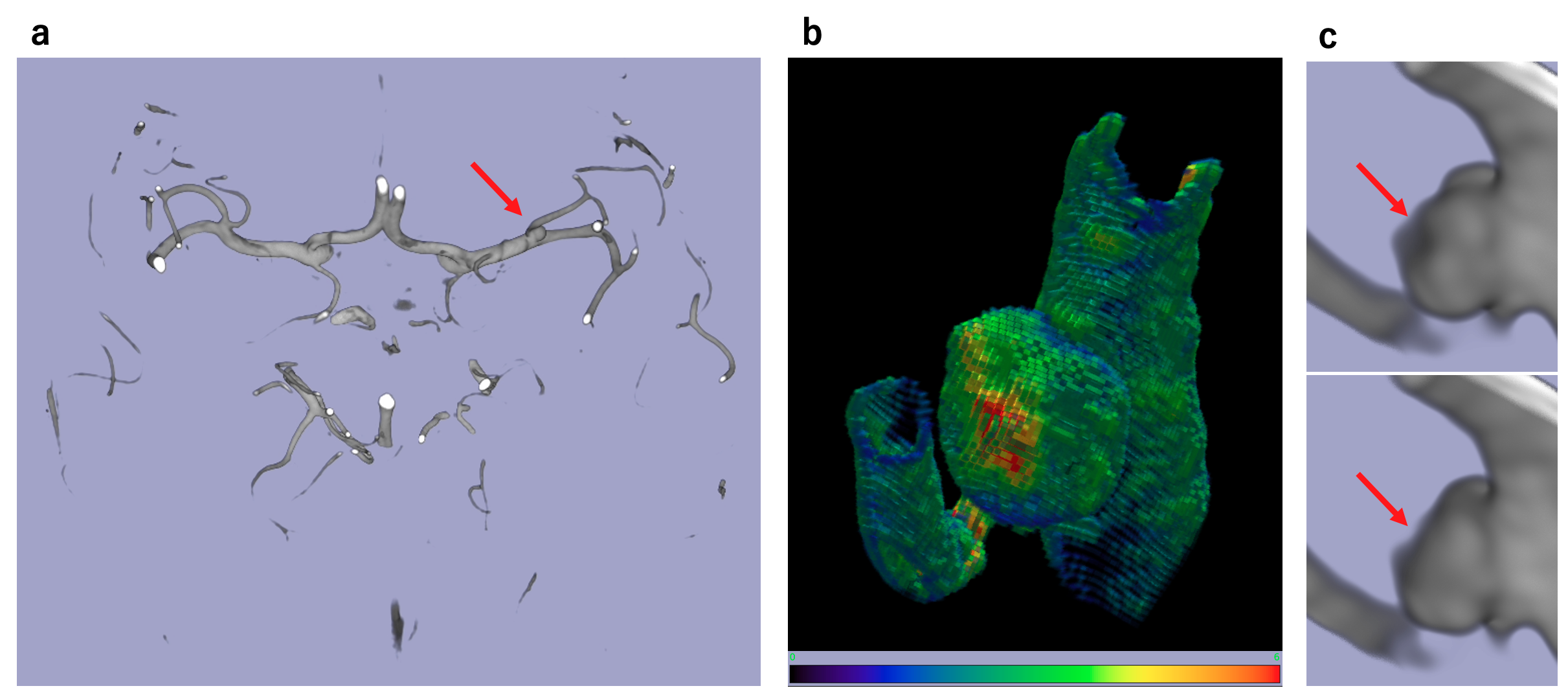
For detailed analysis, a section highlighting the patient's aneurysm was isolated into a smaller volume, which was then enlarged 5-fold to 100 x 100 x 75 pixels using cubic interpolation. This resampled data was processed with a minimal line integral algorithm to track the aneurysm wall's motion over time5. Finally, the greatest extent of wall movement at each voxel was illustrated on a surface color map (Figure 2).
RESULTS and DISCUSSION
The dynamic behavior of the aneurysm phantom was depicted as 3D-cine images, at 26 and 75 frames per pulse (Figure 1). Similarly, the patient's aneurysmal vessel motion was visualized as well, at 72 frames per pulse. A colormap overlay on the aneurysm wall motion enabled precise identification and quantification of the regions with significant wall movement, potentially indicative of rupture risk (Figure 2).Further research is necessary to ascertain the accuracy of the depicted wall motions, by scanning more patients and conducting comparative analysis with 4D CTA. Additionally, our initial findings from whole-brain 3D-cine vessel imaging utilizing a full-3D golden-angle k-space trajectory, hold promise for potentially advancing our understanding of the glymphatic system6.
CONCLUSION
Our novel GRASP-MRA method with 7T MRI effectively captured aneurysm wall motion at ultra-high temporal resolution, suggesting its potential in evaluating intracranial aneurysm pulsations and their risk of rupture.Acknowledgements
No acknowledgement found.References
1. Stam, L. B. et al. A review on imaging techniques and quantitative measurements for dynamic imaging of cerebral aneurysm pulsations. Sci Rep 11, (2021).2. Zhang, J. et al. Irregular pulsation of intracranial unruptured aneurysm detected by four-dimensional CT angiography is associated with increased estimated rupture risk and conventional risk factors. J Neurointerv Surg 13, 854–859 (2021).
3. Feng, L. et al. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magn Reson Med 75, 775–788 (2016).
4. Beck, A. & Teboulle, M. A fast iterative shrinkage-thresholding algorithm for linear inverse problems. SIAM J Imaging Sci 2, 183–202 (2009).
5. Aganj, I., Sapiro, G., Parikshak, N., Madsen, S. K. & Thompson, P. M. Measurement of cortical thickness from MRI by minimum line integrals on soft-classified tissue. Hum Brain Mapp 30, 3188–3199 (2009).
6. Mestre, H. et al. Flow of cerebrospinal fluid is driven by arterial pulsations and is reduced in hypertension. Nat Commun 9, (2018).
Figures