3354
Cerebral Blood Flow Variations by pCASL Corroborates Clinical Neurobehavioral Scores in a Canine Model of Hypothermic Circulatory Arrest1Surgery, Johns Hopkins University, Baltimore, MD, United States, 2Radiology, Johns Hopkins University, Baltimore, MD, United States, 3Johns Hopkins University, Baltimore, MD, United States, 4Division of Cardiac Surgery, Johns Hopkins University, Baltimore, MD, United States, 5Surgery, University of Vermont, Burlington, VT, United States, 6Pediatric Neuroscience, Johns Hopkins University, Johns Hopkins University, Baltimore, MD, United States, 7Developmental Neurology, Kenney Krieger Institute, Johns Hopkins University, Baltimore, MD, United States, 8Neuroradiology, Johns Hopkins University, Johns Hopkins University, Baltimore, MD, United States, 9Division of MR Research, Johns Hopkins Radiology, Johns Hopkins University, Baltimore, MD, United States, 10Division of Cardiac Surgery, Johns Hopkins University, Johns Hopkins University, Baltimore, MD, United States
Synopsis
Keywords: Flow, Cardiovascular, neuroprotection in cardiac surgery
Motivation: Cerebral injury following deep hypothermic circulatory arrest (HCA) remains an important clinical problem in cardiac surgery. Investigating mechanisms of neuroprotection and establishing clinically efficient means to assess acute brain injury following HCA has been the cornerstone of our laboratory's work.
Goal(s): Identify mechanism of cerebral injury following HCA. Establish accurate and efficient mechanisms for diagnosing acute brain injury following HCA.
Approach: Double blinded, prospective, randomized large animal study using canines and multiple neurobehavioral testing instruments including clinically validated methods and pCASL MR imaging.
Results: Cerebral blood flow corroborates with clinically validated neurobehavioral scoring instruments in a canine model of HCA.
Impact: By employing highly effective mechanisms for acute brain injury diagnosis and matching these with ongoing RO1-funded mechanism of neuroprotection following HCA, we aim to impact all cardiac patients in the world who may need deep hypothermic circulatory arrest.
Introduction
Varying degrees of brain injury have been documented in as high as 30% of patients undergoing hypothermic circulatory arrest (HCA).1 Among others, excessive glutamate release and overactivation of the NMDA receptors have been implicated in the HCA-related cerebral injuries2-3. The regions of the brain most susceptible to HCA-related injury include the cerebellum, hippocampus, thalamus, amygdala and cortex4. In a canine model of HCA, a non-invasive, an efficient assessment of pre and postoperative neurological testing is imperative. At the bedside, a number of neurobehavioral batteries are available including the Pittsburgh and Finnish Canine Neurological Testing instruments5-6. From prior literature, the Finnish canine neurological measurement instrument can better correlate with degrees of brain injury in a canine model of HCA. Pseudo-continuous arterial spin labeling (pCASL), a non-invasive and emerging magnetic resonance (MR) technique with excellent sensitivity and specificity to perfusion alterations in the acute brain injury, has shown great promise in delineating regional differences in cerebral perfusion7-8. In this study, we hypothesized that variations in pre and post cerebellar relative brain perfusion would corroborate with the Finnish and Pittsburgh canine testing instruments following HCA.Methods
In a survival model of canine HCA, baseline assessment was completed using the Finnish and Pittsburgh instruments. Additionally, baseline brain MRI with pCASL was completed. Following 90-minutes of deep HCA, repeat testing was done on post-operative days (POD) 1, 2 and 3. Pre- and post-op MRI was obtained on post-op day (POD) 0 and POD1, respectively. MRI images were acquired using a 3T Philips using a 32 channel receiver head coil. To measure the cerebral blood flow (CBF), pseudo-continuous arterial spin imaging (pCASL) was used. The imaging parameters for pCASL acquisition were: FOV = 140×140×80 mm2, TR/TE = 3600/11.74 ms, labelling duration (LD) = 1100 ms, post-labelling delay = 1800 ms, voxel dimension = 2.18×2.18×4 mm3, dynamic = 40, readout = single-shot multi-slice (MS) echo planar imaging (EPI) with SENSE 2.5. CBF was quantified using control label subtraction followed by normalization with M01. CBF was adjusted for each slice to account for the time delay between slice acquisitions. To compute relative CBF (rCBF), voxel-wise CBF map was normalized using the global mean CBF value. Cerebellum was manually segmented, and relative percentage variation (RPV) was used as a quantitative matric to evaluate the regional variation in rCBF value pre- and post-HCA.Results
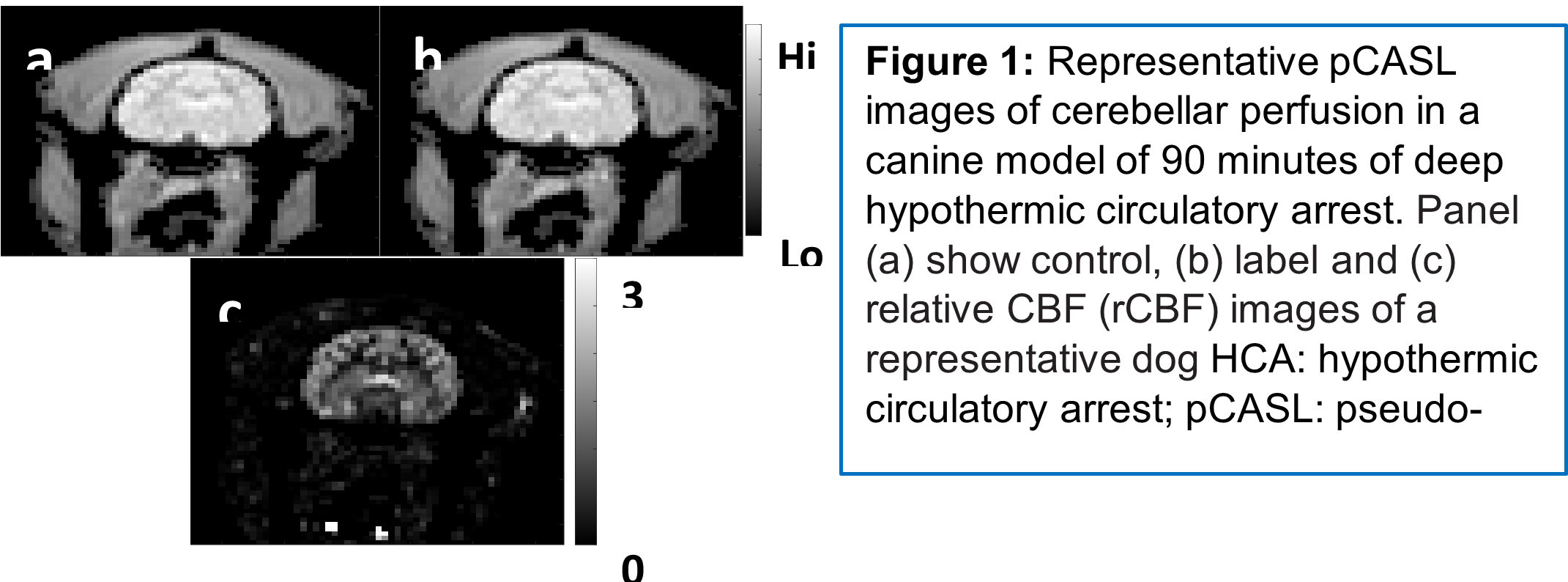
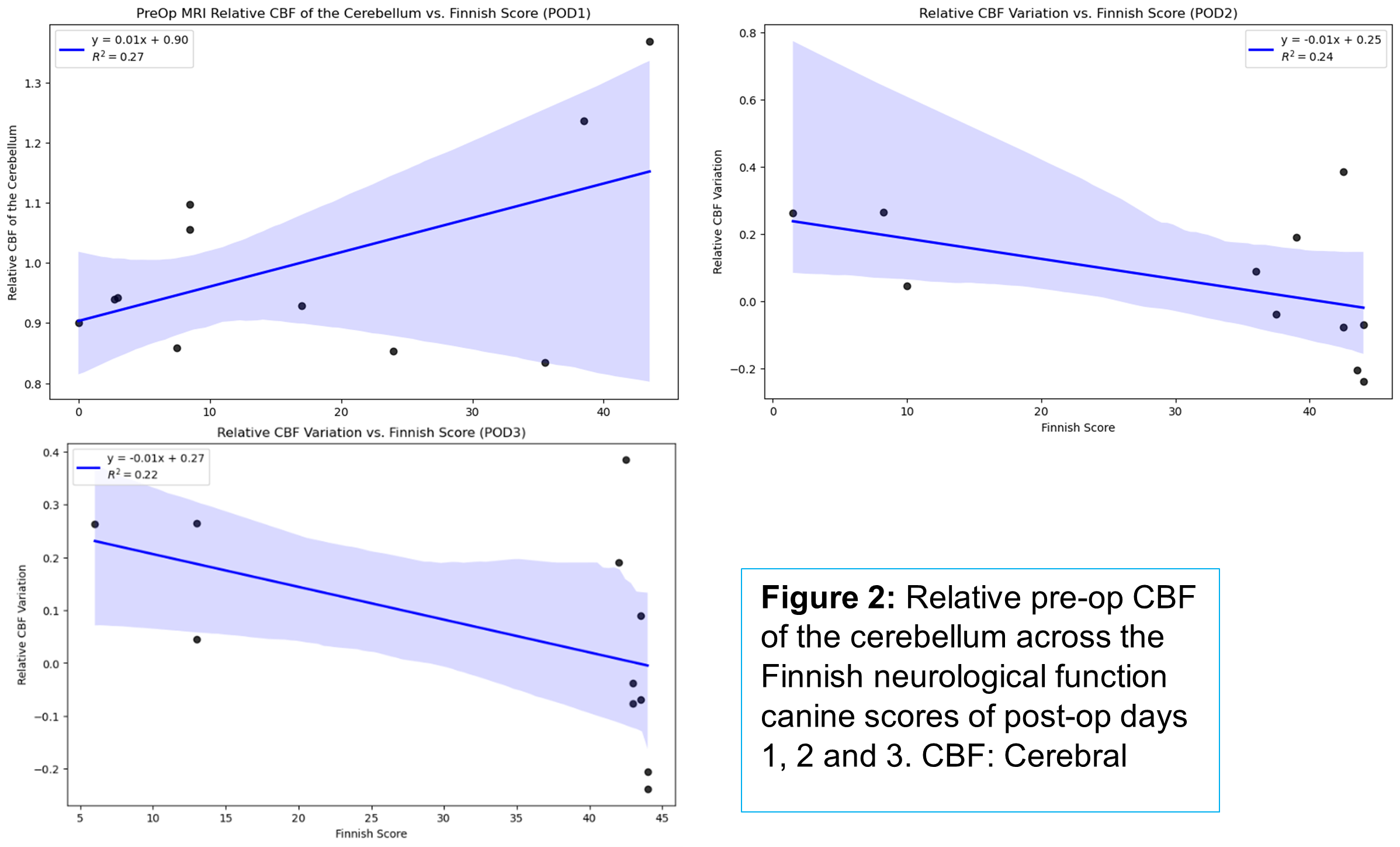
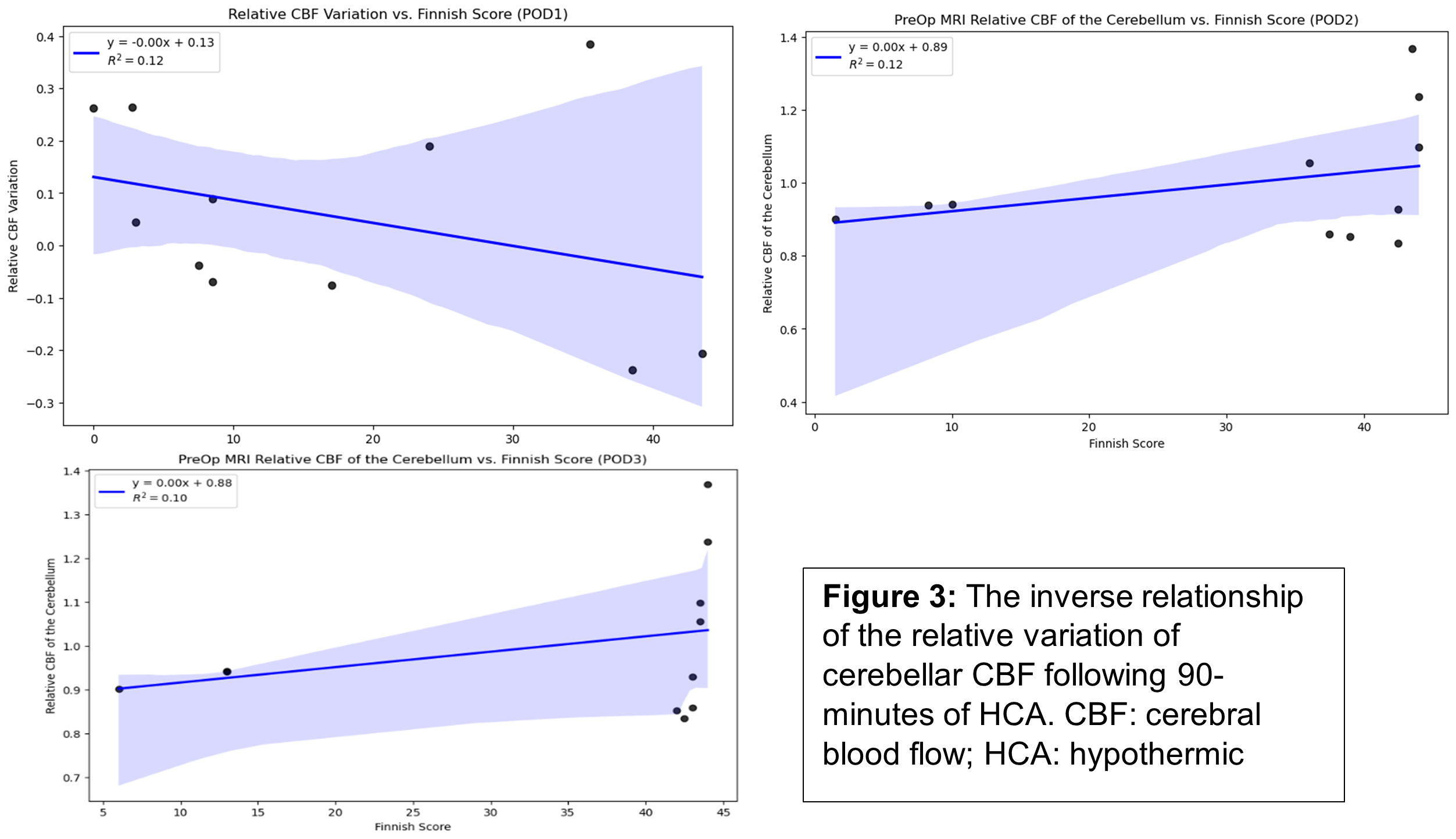
Figure 1 shows a representative CBF map. Out of n=23 canines, 17 completed post-operative evaluation with neurobehavioral testing and MR imaging. Finnish scores were worst at 24 hours (median 8.5 (5.25, 29.75) following HCA and showed improvements in treated animals from the 48-hour (median 39 (23, 43), timepoint and continuing for 72 hours, median 43, (27.5, 43.5). In 55% of subjects (n=6) the post-operative relative cerebellar CBF was higher than baseline. However, 5 animals showed reduced relative cerebellar CBF post-operatively. Although there was no statistically significant differences in the pre- and post- relative cerebellar blood flow, higher relative pre-op cerebellar blood flow correlated with lower Finnish neurological scores across POD1, 2 and 3 (Figure 2). The relative CBF variation, a measure of the degree of variance between the pre- and post-HCA relative CBF (rCBF), was inversely correlated with the Finnish score across POD 1, 2, 3 (R2= 0.12, 0.24, and 0.22, respectively) and positively correlated with the Pittsburgh canine neurobehavioral score (R2= 0.15, 0.21, and 0.18), Figure 3.Discussion
ASL can detect acute differences in regional perfusion following HCA. Evidence shows that the cerebellum is one of the most susceptible regions for injury following HCA. We hypothesized that in animals with higher neurobehavioral scores following HCA, the pre- and post-relative cerebellar cerebral blood flow variability would be lower compared to animals with worse neurological scores. The differences in variability are likely related to differences in treatment groups and sustained cerebral injury, although the limited sample size deters our ability to detect statistical significance at this time. The observed correlation between pCASL relative CBF was strongest with the Finnish, which clinically has been demonstrated to be a robust test for acute brain injury in canines5.Conclusion
In a canine model of HCA, the Finnish, Pittsburgh and pCASL MR imaging can help facilitate quick assessment of acute brain injury. In this study, higher variability between pre- and post-HCA relative CBF was correlated with worse neurological outcomes as measured by bedside Finnish neurological function test. Although a clear association was demonstrated, further analysis with more subjects would help elucidate any statistical significance of the relative CBF measurements as a surrogate for evaluating and possibly predicting clinical neurobehavioral scores following 90-minutes of HCA.Acknowledgements
No acknowledgement found.References
1. Giuliano, K., Etchill, E., Zhou, X., Lui, C., Suarez-Pierre, A., Sharma, R., Wilson, M. A., Blue, M. E., Troncoso, J. C., Kannan, S., Johnston, M. V., Sharma, A., Kannan, R. M., Baumgartner, W. A., & Lawton, J. (2021). NMDA Receptor Antagonism for Neuroprotection in a Canine Model of Hypothermic Circulatory Arrest. The Journal of surgical research, 260, 177–189. https://doi.org/10.1016/j.jss.2020.11.075 2. Giuliano, K., Etchill, E., Velez, A. K., Wilson, M. A., Blue, M. E., Troncoso, J. C., Baumgartner, W. A., & Lawton, J. S. (2023). Ketamine Mitigates Neurobehavioral Deficits in a Canine Model of Hypothermic Circulatory Arrest. Seminars in thoracic and cardiovascular surgery, 35(2), 251–258. https://doi.org/10.1053/j.semtcvs.2021.12.004 3. Shake, J. G., Peck, E. A., Marban, E., Gott, V. L., Johnston, M. V., Troncoso, J. C., Redmond, J. M., & Baumgartner, W. A. (2001). Pharmacologically induced preconditioning with diazoxide: a novel approach to brain protection. The Annals of thoracic surgery, 72(6), 1849–1854. https://doi.org/10.1016/s0003-4975(01)03192-7 4. Ananiadou, O. G., Drossos, G. E., Bibou, K. N., Palatianos, G. M., & Johnson, E. O. (2005). Acute regional neuronal injury following hypothermic circulatory arrest in a porcine model. Interactive cardiovascular and thoracic surgery, 4(6), 597–601. https://doi.org/10.1510/icvts.2005.112813 5. Korpi, E. R., Lindholm, D., Panula, P., Tienari, P. J., & Haltia, M. (2020). Finnish neuroscience from past to present. European Journal of Neuroscience, 52(5), 3273-3289. https://doi.org/10.1111/ejn.14693 6. Goldstein, G., Tarter, R. E., Shelly, C., & Hegedus, A. M. (1983). The pittsburgh initial neuropsychological testing system (pints): a neuropsychological screening battery for psychiatric patients. Journal of Behavioral Assessment, 5(3), 227-238. https://doi.org/10.1007/bf01322150 7. Alsop, D. C. et al. Recommended implementation of arterial spin-labeled Perfusion mri for clinical applications: A consensus of the ISMRM Perfusion Study group and the European consortium for ASL in dementia. Magn Reson Med 73, 102–116 (2015). 8. Iutaka, T., Freitas, M. B. d., Omar, S. S., Scortegagna, F. A., Nael, K., Nunes, R. H., … & Rocha, A. J. d. (2023). Arterial spin labeling: techniques, clinical applications, and interpretation. RadioGraphics, 43(1). https://doi.org/10.1148/rg.220088Figures