3352
Association of Systemic inflammatory response index with intracranial plaque vulnerability and the severity of ischemic events1The Second Affiliated Hospital of Chongqing Medical University, Chongqing, China, 2Third Military Medical University(Army Medical University), Chongqing, China, 3Clinical Science, Philips Healthcare, Chengdu, China
Synopsis
Keywords: Atherosclerosis, Atherosclerosis, High-resolution magnetic resonance vessel wall imaging; Systemic Inflammatory Response Index
Motivation: The activation of inflammation can aggravate plaque rupture, thrombosis and cause brain tissue ischemia and infarction. Looking for reliable inflammatory markers might provide potential targets for the treatment of atherosclerosis patients.
Goal(s): We investigated the relationship between systemic inflammatory response index (SIRI)and intracranial plaque features, as well as the risk factors related to the severity of cerebral ischemic events.
Approach: Compare the differences in imaging features and SIRI among patients with transient ischemic attack, mild stroke, and moderate-severe stroke.
Results: SIRI levels were significantly associated with plaque vulnerable characteristics and burden. Higher SIRIlevels and plaque featureswere independently related to moderate-severe stroke.
Impact: Our study suggested that immune inflammation may have adverse effects on intracranial atherosclerosis, and link to the severity of cerebral ischemic events. Therefore, the regulation of immune inflammation may be a potential therapeutic target for sICAD.
Introduction
Symptomatic intracranial atherosclerosis (sICAD) is the main cause of stroke burden in Chinese population, with a prevalence as high as 46% [1]. Chronic inflammation plays an important role in the occurrence and development of atherosclerosis and stroke [2,3]. The systemic inflammatory response index (SIRI = neutrophils x monocytes/lymphocytes) [4] has been reported to be related to the prevalence and severity of femoral plaque, carotid plaque, and coronary artery disease (CAD) [5,6]. As a disease of the atherosclerotic spectrum, intracranial atherosclerotic disease (ICAD) may have similar pathophysiological mechanisms. High resolution vascular wall imaging provides an opportunity to evaluate the characteristics and burden of ICAD. Therefore, the purpose of our study is to investigate (a) the association of SIRI levels with intracranial culprit plaques characteristics and ICAD burden, and (b) further evaluate the risk factors related to the severity of sICAD.Methods
This study was approved by the institutional ethics committee. We enrolled 120 patients [59.70±11.55; 76, (63.3%) male] with symptomatic intracranial atherosclerosis (sICAD). All the subjects underwent magnetic resonance examination, including DWI、3D time-of-flight (TOF) MRA、pre- and post-contrast 3D volume isotropic turbo spin-echo acquisition (VISTA), on a 3T clinical scanner (Achieva, Philips Healthcare). The correlation between SIRI levels and intracranial plaque features were analyzed by multiple sample ANOVA or Spearman's test. Multivariable ordered logistic regression was evaluated the risk factors associated with the severity of cerebral ischemic events. The efficacy of combined evaluation to classify clinical subtypes of sICAD was performed through the receiver operating characteristic (ROC) curve.Results
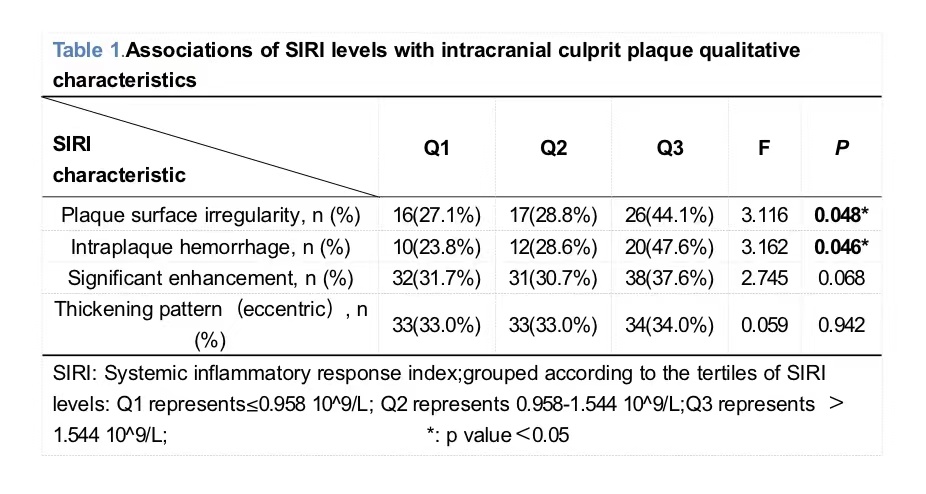
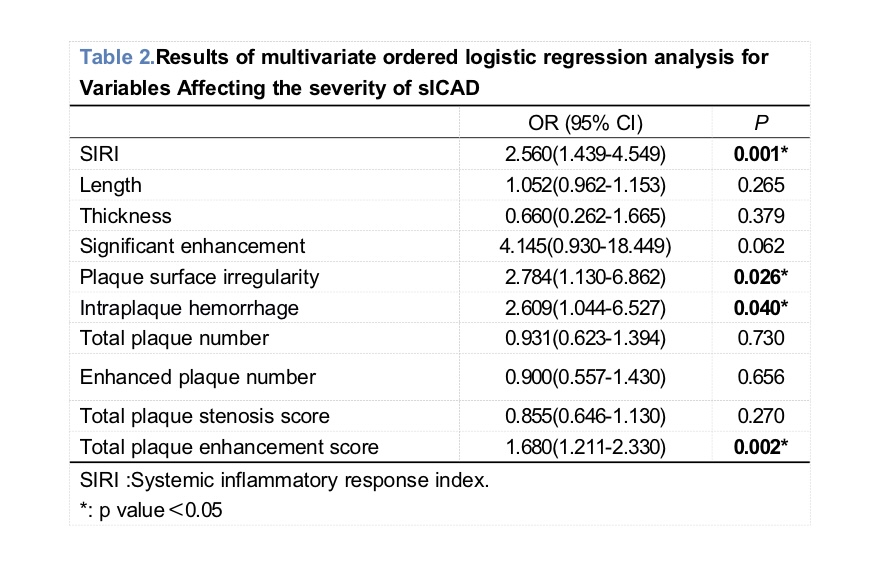
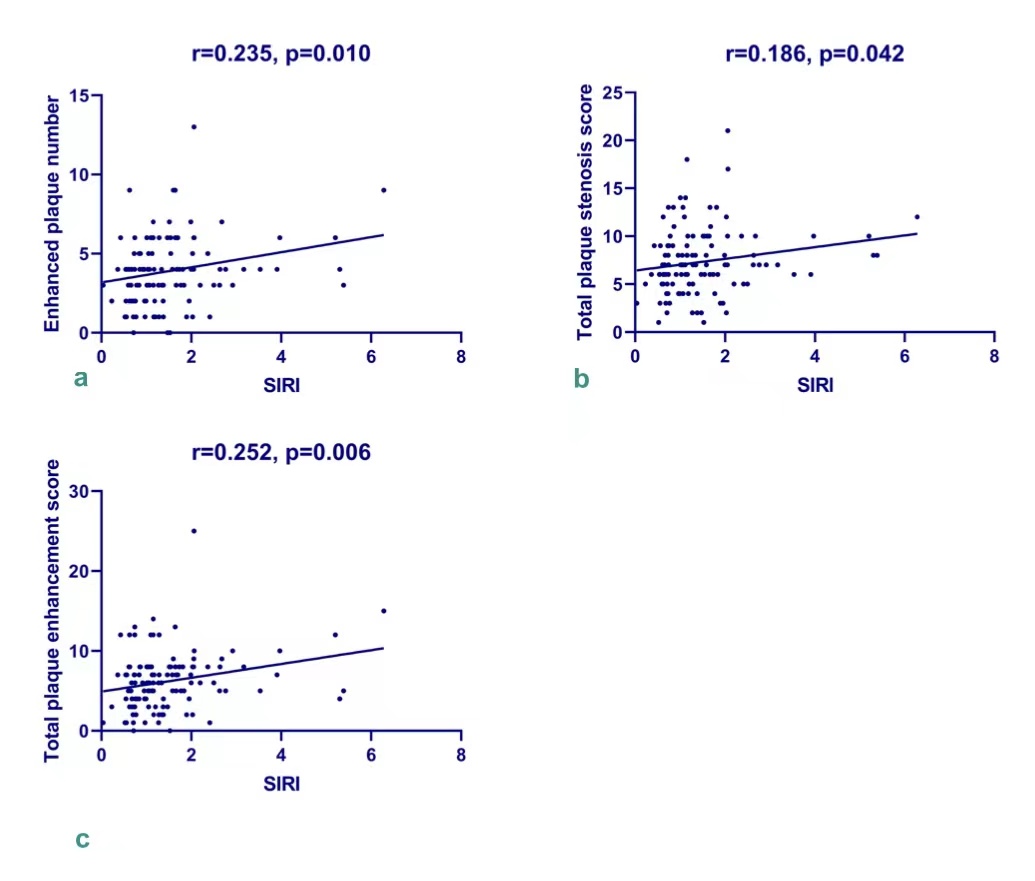
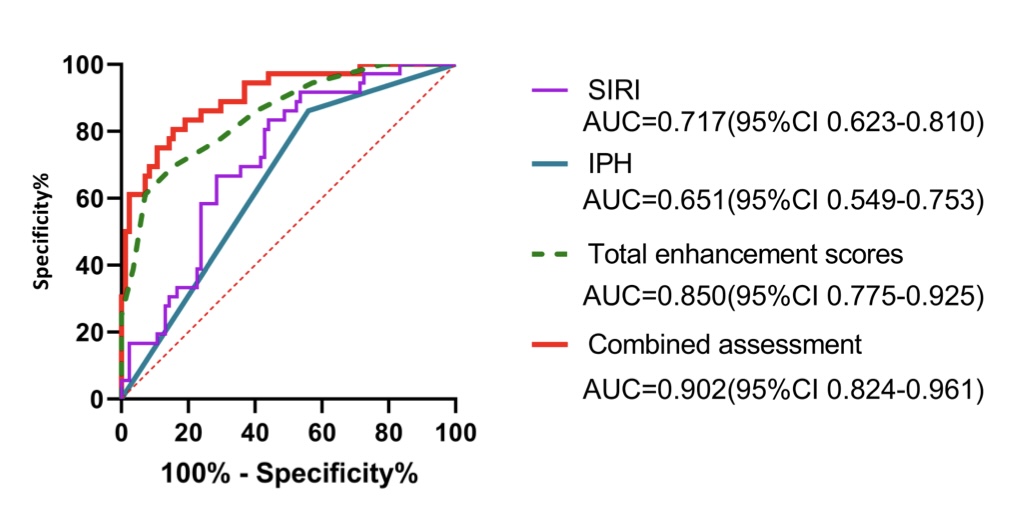
SIRI levels were significantly associated with the enhanced plaque number (r = 0.235, p = 0.010), total plaque stenosis score (r = 0.186, p = 0.042), total plaque enhancement score (r = 0.252, p = 0.006) (Figure 1), intraplaque hemorrhage (F = 3.162, p = 0.046), and plaque surface irregularity (F = 3.116, p = 0.048) (Table 1). Higher SIRI levels (OR =2.560), total plaque enhancement score (OR =1.680), intraplaque hemorrhage (OR =2.609) and plaque surface irregularity (OR =2.784) were independently related to moderate-severe stroke (Table 2). The SIRI combined with plaque characteristics showed the best performance in the ROC curve, with an area under the curve of 0.902 (95%CI 0.842-0.961), significantly higher than intraplaque hemorrhage 0.651 (95%CI 0.549-0.753) and plaque enhancement scores 0.850 (95%CI 0.775-0.925) alone (Figure 2).Discussion
The results showed that SIRI levels were significantly positively linked to enhanced plaque number, total plaque stenosis score, and total plaque enhancement score. Since atherosclerosis is a systemic inflammatory disease, often involving multiple blood vessels [7], it is not difficult to explain that the impact of peripheral inflammation on ICAD is not limited to culprit plaque, but the entire burden caused by atherosclerosis. Similar to previous studies on the same topic [8,9], we found that SIRI levels were independently associated with intraplaque hemorrhage and plaque surface irregularity, and our study extended this association to the intracranial large artery vascular tree. This indicated that the imbalance of immune inflammation might be related to plaque vulnerability, but it cannot explain causality and needs to be further validated in future prospective studies. And then, our study suggested that higher levels of SIRI, total plaque enhancement score, intraplaque hemorrhage, and plaque surface irregularity were independently associated with more severe cerebral ischemic events. It suggested that immune inflammation might play a role in the vulnerability and burden of intracranial atherosclerotic plaque, and might increase the risk and severity of stroke by affecting the plaque. In addition, the combined evaluation of SIRI levels and imaging indicators achieved the best diagnostic performance in distinguishing clinical subtypes of sICAD patients, we speculated that this might be attributed to the synergistic effect of SIRI on the occurrence of AIS by affecting plaque vulnerability and burden.Conclusion
SIRI is expected to become an important supplementary tool for predicting plaque instability and risk stratification in sICAD patients, and the regulation of immune inflammation may be a potential target for the future treatment.Acknowledgements
We thank all participants who contributed their time, knowledge, and energy to developing this research.References
[1]. Wang Y, Zhao X, Liu L, et al.CICAS Study Group. Prevalence and outcomes of symptomatic intracranial large artery stenoses and occlusions in China: the Chinese Intracranial Atherosclerosis (CICAS) Study. Stroke. 2014 Mar;45(3):663-9. doi: 10.1161/STROKEAHA.113.003508. Epub 2014 Jan 30. PMID: 24481975.
[2]. Kasikara C, Doran AC, Cai B, et al. The role of non-resolving inflammation in atherosclerosis. J Clin Invest. 2018 Jul 2;128(7):2713-2723. doi: 10.1172/JCI97950. Epub 2018 Jul 2. PMID: 30108191; PMCID: PMC6025992.
[3]. Hansson GK. Atherosclerosis--an immune disease: The Anitschkov Lecture 2007. Atherosclerosis. 2009 Jan;202(1):2-10. doi: 10.1016/j.atherosclerosis.2008.08.039. Epub 2008 Sep 6. PMID: 18951547.
[4]. Qi Q, et al. A novel systemic inflammation response index (SIRI) for predicting the survival of patients with pancreatic cancer after chemotherapy. Cancer. 2016 Jul 15;122(14):2158-67. doi: 10.1002/cncr.30057. Epub 2016 May 6. PMID: 27152949.
[5]. Feng R, Dai Y, Du S, et al. Leukocyte and Platelet Related Inflammatory Indicators and Risk of Carotid and Femoral Plaques: A Population-Based Cross-Sectional Study in Southeast China. Angiology. 2022 Sep 29:33197221129723. doi: 10.1177/00033197221129723. Epub ahead of print. PMID: 36175416.
[6]. Dziedzic EA,Gąsior JS, Tuzimek A, et al. Investigation of the Associations of Novel Inflammatory Biomarkers-Systemic Inflammatory Index (SII) and Systemic Inflammatory Response Index (SIRI)-With the Severity of Coronary Artery Disease and Acute Coronary Syndrome Occurrence. Int J Mol Sci. 2022 Aug 23;23(17):9553. doi: 10.3390/ijms23179553. PMID: 36076952; PMCID: PMC9455822.
[7]. Li J, Li D, Yang D, et al. Co-existing cerebrovascular atherosclerosis predicts subsequent vascular event: a multi-contrast cardiovascular magnetic resonance imaging study. J Cardiovasc Magn Reson. 2020 Jan 13;22(1):4. doi: 10.1186/s12968-019-0596-6. PMID: 31928532; PMCID: PMC6956475.
[8]. Fani L, van Dam-Nolen DHK, Vernooij M, et al. Circulatory markers of immunity and carotid atherosclerotic plaque. Atherosclerosis. 2021 May;325:69-74. doi: 10.1016/j.atherosclerosis.2021.03.040. Epub 2021 Apr 7. PMID: 33894597.
[9]. Zhang L, Lyu Q, Zhou W, et al. High systemic immune-inflammation index is associated with carotid plaque vulnerability: New findings based on carotid ultrasound imaging in patients with acute ischemic stroke. Front Neurol. 2022 Sep 1;13:959531. doi: 10.3389/fneur.2022.959531. PMID: 36158955; PMCID: PMC9505015.
Figures