3350
Assessment of Intracranial Curved and Distal Small Arteries by Using zTE-MRA: Comparison with TOF-MRA1Radiology, Ren ji Hospital, School of Medicine, Shanghai Jiaotong University, Shanghai, China, 2Radiology, Hangzhou Bay hospital, Ningbo, China, 3MR Research, GE Healthcare, Shanghai, China
Synopsis
Keywords: Vascular, Vessels
Motivation: Time-of-flight MRA (TOF-MRA) is sensitive to abnormal blood flow and result in susceptibility artifact signal and signal loss in distal small artery.
Goal(s): To investigate whether zero echo time MRA (zTE-MRA) could improve the image quality in intracranial artery with the same scan time.
Approach: Recruiting healthy subjects and taking zTE-MRA and TOF-MRA scanning.
Results: Compared with TOF-MRA using the same scan time, zTE-MRA could reduce susceptibility artifact signal in intracranial curved artery and suppress tissue signal intensity surrounding artery to better show ophthalmic artery.
Impact: Providing a non-invasive method to better reduce susceptibility artifact signal in intracranial curved artery and suppress tissue signal intensity surrounding artery to better show distal small artery.
Background and Purpose
Accurate and non-invasive assessment of intracranial artery is important for it relate to various diseases like ischemic and hemorrhagic stroke. Both zTE-MRA and TOF-MRA could evaluate intracranial artery lumen without contrast agent. Previous study found that zTE-MRA have advantage over TOF-MRA in susceptibility artifact signal, flow signal of parent artery, detection of vascular stenosis degree, intracranial aneurysm and coiled intracranial aneurysm[1-3]. However, the detectability of small artery was not mentioned yet. And the scan time of these two sequences was great different in previous studies.METHODS
A total of 18 healthy subjects were prospective recruited between August 2023 to October 2023. ZTE-MRA and TOF-MRA sequences were conducted for all participants using a 3.0T clinical MR system (Discovery 750w, GE Healthcare, USA) with a 24-channel head and neck joint coil. The protocols of zTE-MRA and TOF-MRA were as follows respectively: 1) zTE-MRA: TR/TE 1542/0 msec, number of slices 78, field of view 200mm×200mm, voxel size 1.0mm×1.0mm×1.0mm, flip angle 3°, acquisition matrix 192×192, and scan time 5 minutes 54 seconds. 2) TOF-MRA: TR/TE 11/2.4msec, number of slices 160, field of view 220mm×220mm, voxel size 0.6mm×0.6mm×1.0mm, flip angle 20°, acquisition matrix 366×366, and scan time 5 minutes 51 seconds. Both susceptibility artifact intensity and small artery detectability were evaluated. 1) The susceptibility artifact intensity mainly reflected by signal loss was evaluated on internal carotid artery C4-6 segments. A 4-point scale (4= no susceptibility signal loss; 3= minimal signal loss; 2= moderate signal loss, compromising image assessment; and 1= severe signal loss, preventing image evaluation) was applied to rate the susceptibility artifact intensity for both zTE- and TOF-MRA images. 2) Small artery detectability was evaluated in anterior choroidal artery, superior cerebellar artery and ophthalmic artery. A separate 4-point scale, reported previously for similar analysis, was applied also for data analysis. It is defined as: 4= excellent quality; 3=good quality, with minimal blurring or artifacts; 2= poor quality, with structures slightly visible and significant blurring; and 1= not visible. Weighted kappa (κ) statistics were used to assess the inter-observer agreement. The Wilcoxon signed-rank test was used to evaluate differences in image quality between zTE- and TOF-MRA images.RESULTS
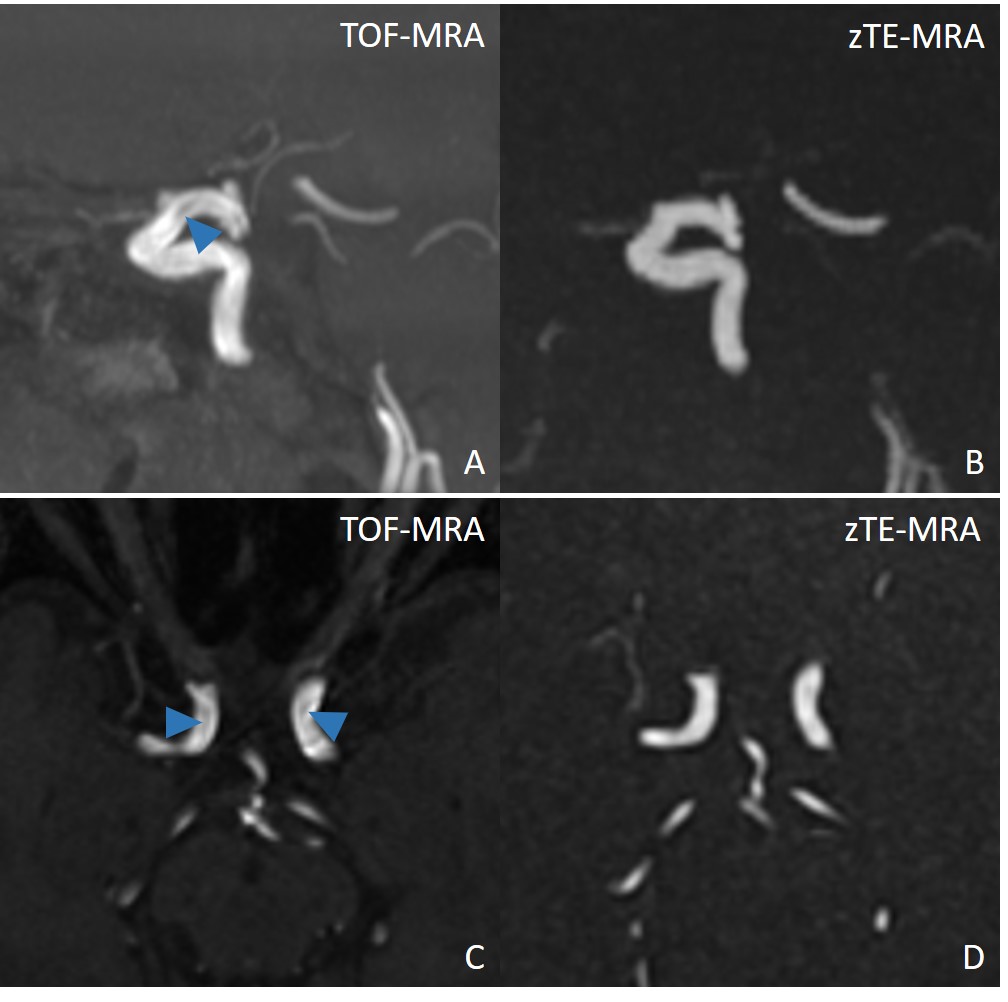
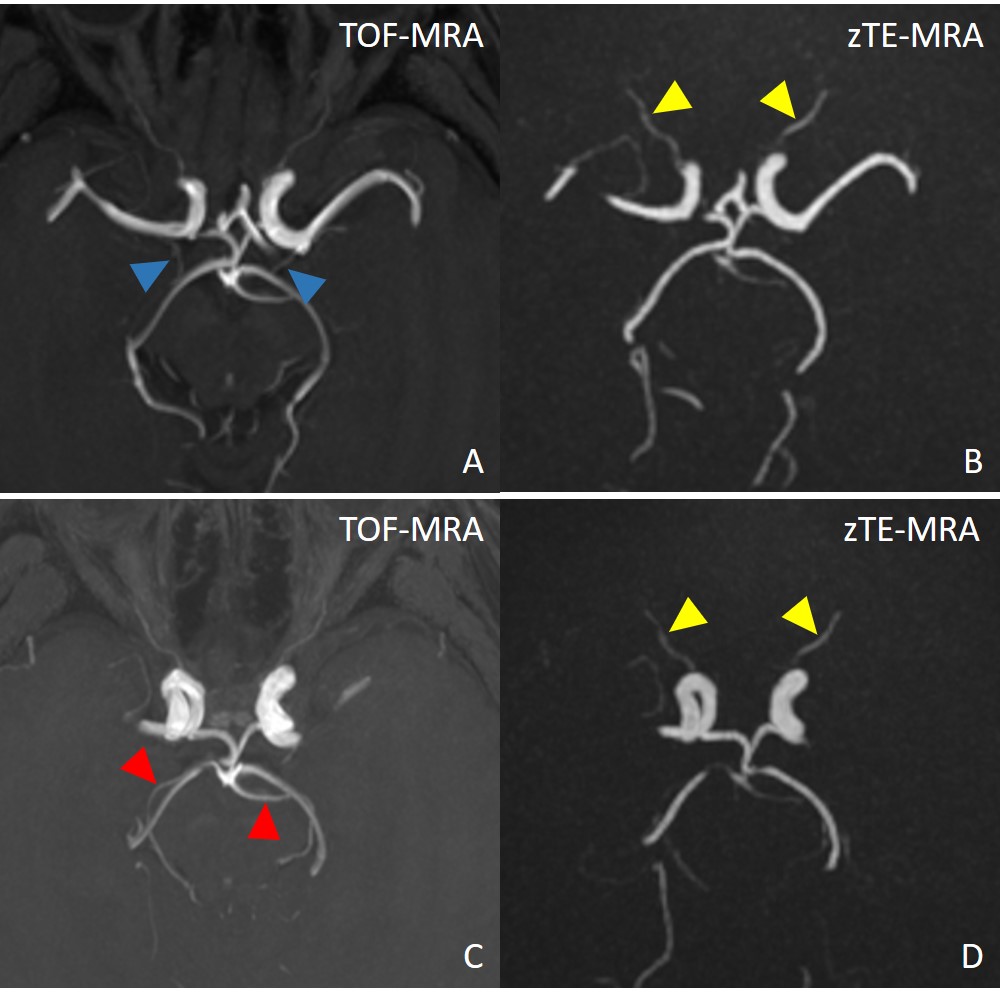
Eighteen healthy subjects were included in the study. Supported by high inter-observer agreement (all weighted κ>0.8), zTE-MRA generated significantly higher scores than TOF-MRA for susceptibility artifact signal (3.56±0.51 vs. 2.61±0.50, P<0.001). ZTE-MRA showed worse anterior choroidal artery and superior cerebellar artery detectability than TOF-MRA (2.17±0.62 vs. 3.39±0.50, P<0.001; 2.50±0.62 vs. 3.61±0.50, P<0.001; respectively), while better ophthalmic artery detectability than TOF-MRA (3.50±0.51 vs. 3.00±0.49, P=0.003).DISCUSSION
We found with the same scan time, zTE-MRA could reduce the artifact signal in curved segment of distal internal carotid artery than TOF-MRA. It is consistent with previous study[1]. TOF-MRA is sensitive to abnormal blood flow at different velocities and thus its application for patients with intracranial vascular diseases like dissection and aneurysm is generally challenging. In contrast, the rising novel technology of zTE-MRA using a 3D radial acquisition read-out scheme with an ultrashort echo time (~10 µs) can generate high signal intensity and is immune to local field inhomogeneity and magnetic susceptibility artifacts, which is essential for accurate display of blood vessels[4]. Besides, it’s also important to evaluate the small intracranial artery, like anterior choroidal artery, superior cerebellar artery and ophthalmic artery, which is sensitive to vascular disease and lead to stroke. With the same scan time, zTE-MRA showed worse anterior choroidal artery and superior cerebellar artery detectability while better ophthalmic artery detectability than TOF-MRA. The poor performance may cause by inversion recovery in the distal small artery. The superior performance of ophthalmic artery may benefit from suppressing tissue signal intensity surrounding artery.CONCLUSION
Compared with TOF-MRA, zTE-MRA could reduce susceptibility artifact signal and suppress tissue signal intensity surrounding artery to better show ophthalmic artery with the same scan time. ZTE-MRA has potential for use as a routine clinical method for patients with intracranial artery disease, but need further improvement.Acknowledgements
No acknowledgement found.References
1. Zhang C, Dou W, Yu K, et al. The feasibility of non-contrast-enhanced zero echo time magnetic resonance angiography for characterization of intracranial atherosclerotic disease. Quant Imaging Med Surg. 2021;11(6):2442-2452. doi:10.21037/qims-20-696
2. Shang S, Ye J, Luo X, Qu J, Zhen Y, Wu J. Follow-up assessment of coiled intracranial aneurysms using zTE MRA as compared with TOF MRA: a preliminary image quality study. Eur Radiol. 2017;27(10):4271-4280. doi:10.1007/s00330-017-4794-z
3. Li Y, Zhu Y, Liu Y, Li G, Qu X. Comparative Study of the Diagnostic Value of Zero-Echo-Time Magnetic Resonance Angiography With Time-of-Flight Magnetic Resonance Angiography for Intracranial Aneurysm [published online ahead of print, 2023 Aug 3]. J Comput Assist Tomogr. 2023;10.1097/RCT.0000000000001518. doi:10.1097/RCT.0000000000001518
4. Wu H, Block WF, Turski PA, Mistretta CA, Johnson KM. Noncontrast-enhanced three-dimensional (3D) intracranial MR angiography using pseudocontinuous arterial spin labeling and accelerated 3D radial acquisition. Magn Reson Med. 2013;69(3):708-715. doi:10.1002/mrm.24298
Figures