3339
Magnetic Resonance Fingerprinting and ADC mapping to optimize Biopsy Decision-Making in patients with a Negative Prostate MRI1Department of Radiology, University Hospitals Cleveland Medical Center, Cleveland, OH, United States, 2Department of Radiology, Case Western Reserve University, Cleveland, OH, United States, 3Department of Population and Quantitative Health Sciences, Case Western Reserve University, Cleveland, OH, United States
Synopsis
Keywords: Prostate, Prostate, magnetic resonance fingerprinting
Motivation: Prostate MRI alone cannot avoid all unnecessary biopsies in MRI-negative patients. This results in overdiagnosis, added morbidity and overtreatment.
Goal(s): Investigate if MRF-derived T1 and T2 maps alone or in combination with conventional ADC mapping can reduce unnecessary biopsies while maintaining optimal significant prostate cancer detection.
Approach: Regions of interest encompassing the right and left lobes of the peripheral zone were used to compute the mean T1, T2, and ADC values.
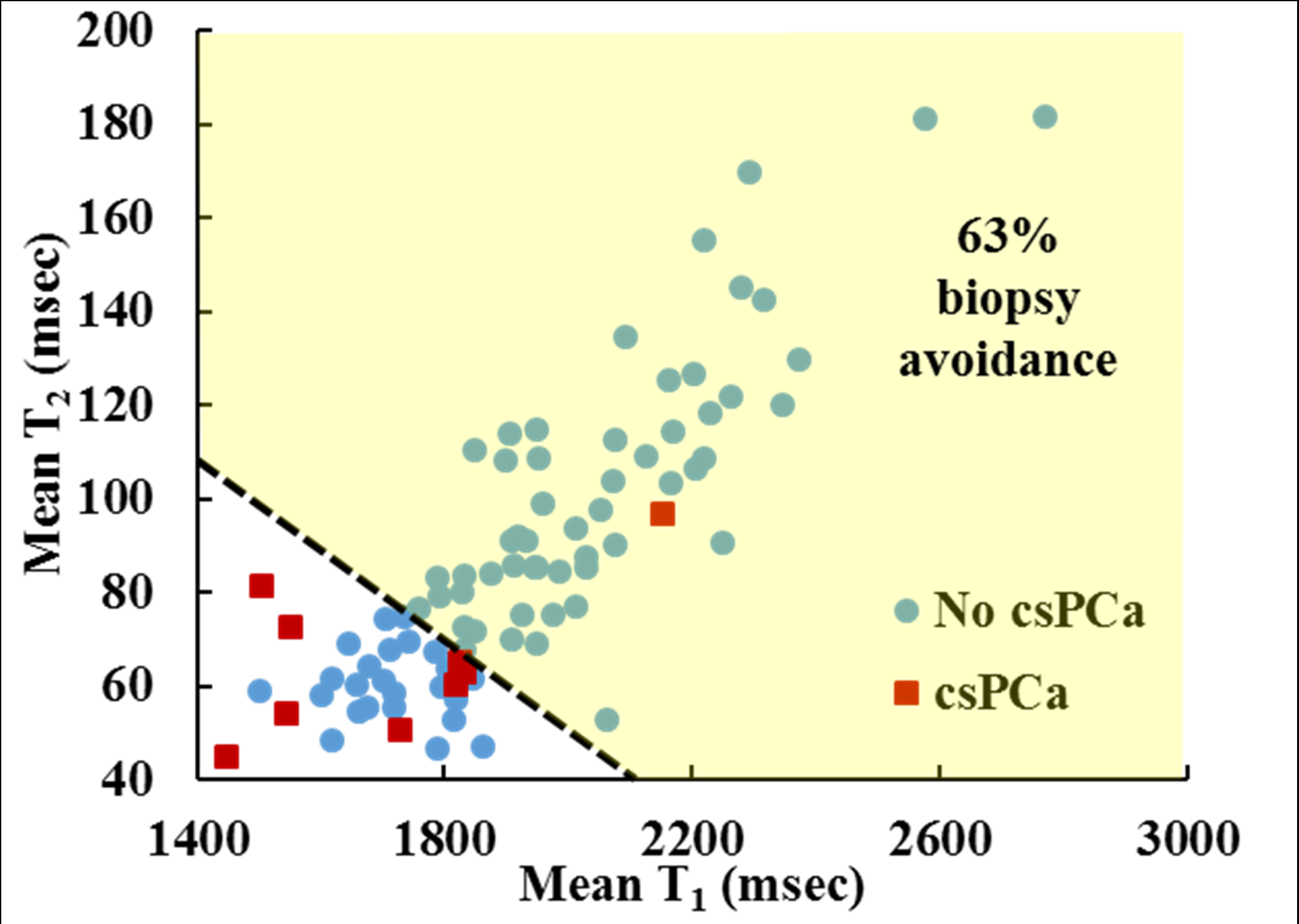
Results: With a linear regression of mean T1 and T2 values, 63% of all biopsies could be avoided, at the cost of missing one significant prostate cancer.
Impact: The use of MR Fingerprinting in prostate biopsy decision-making pathways could reduce unnecessary biopsies while maintaining optimal detection of significant prostate cancer in MRI-negative patients with clinically indicated biopsies. The prospective validation of these findings is crucial for patient outcomes.
INTRODUCTION
Magnetic resonance imaging (MRI) adhering to the Prostate Imaging Reporting and Data System (PI-RADS) v2.1 guidelines is internationally adopted for the detection and characterization of clinically significant prostate cancer (csPCa)1,2. Still, the American Urological Association3 guidelines recommend not deferring a prostate biopsy for MRI-negative patients (PI-RADS 1&2) based on MRI results alone. Clinical risk factors and ancillary tests should be used to select patients for a systematic biopsy3. Although this reduces the number of missed csPCa, it also results in overdiagnosis and a considerable number of unnecessary prostate biopsies performed in patients whose prevalence of csPCa ranges only from 8-10%. A quantitative MRI technique, MR fingerprinting (MRF), was shown to improve the characterization of prostatic lesions with exceptional reproducibility4–7. Therefore, in this retrospective study of MRI-negative patients who had a clinically indicated biopsy, we aim to investigate if MRF-derived T1 and T2 maps alone or in combination with conventional ADC mapping can avoid unnecessary biopsies while maintaining optimal csPCa detection.METHODS
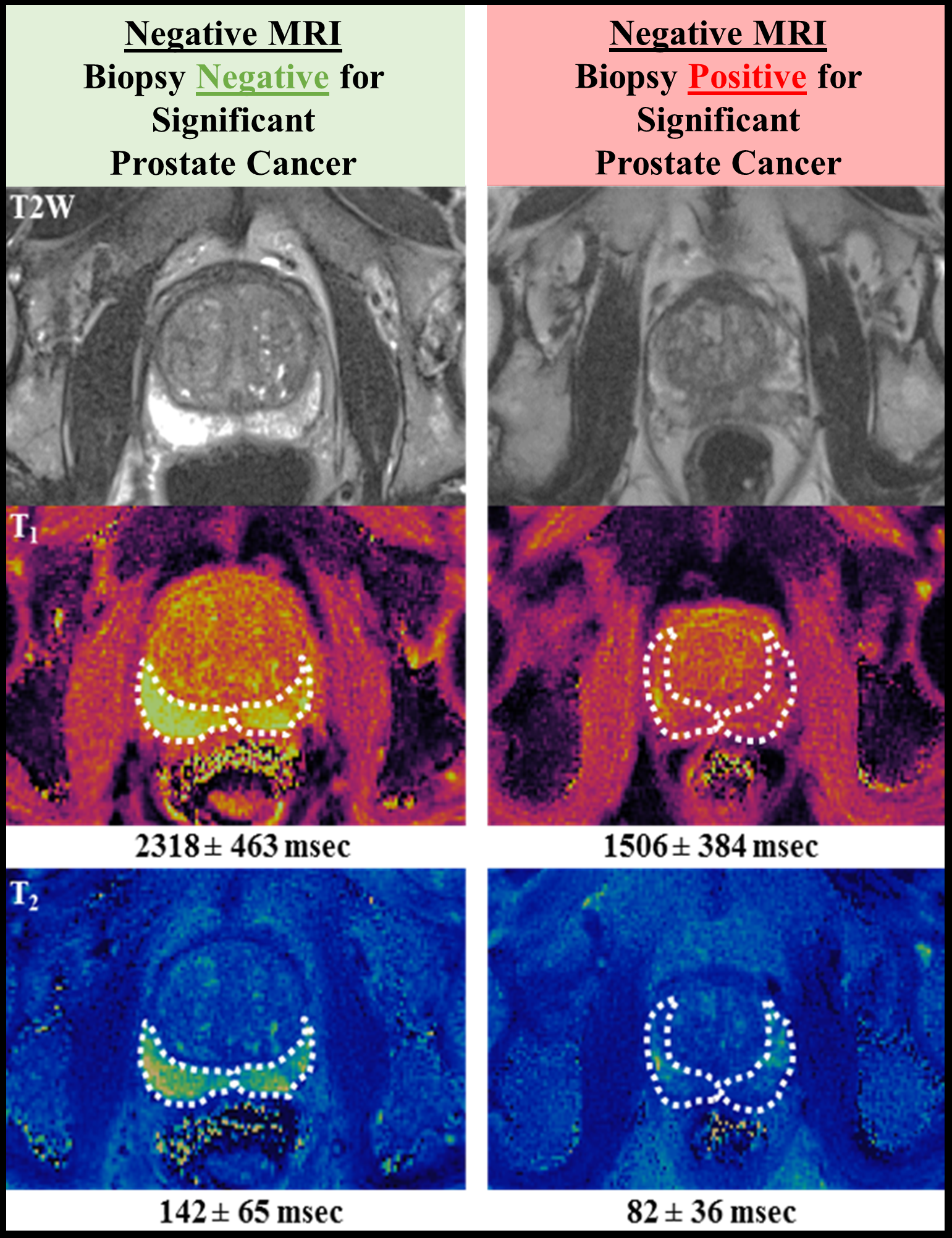
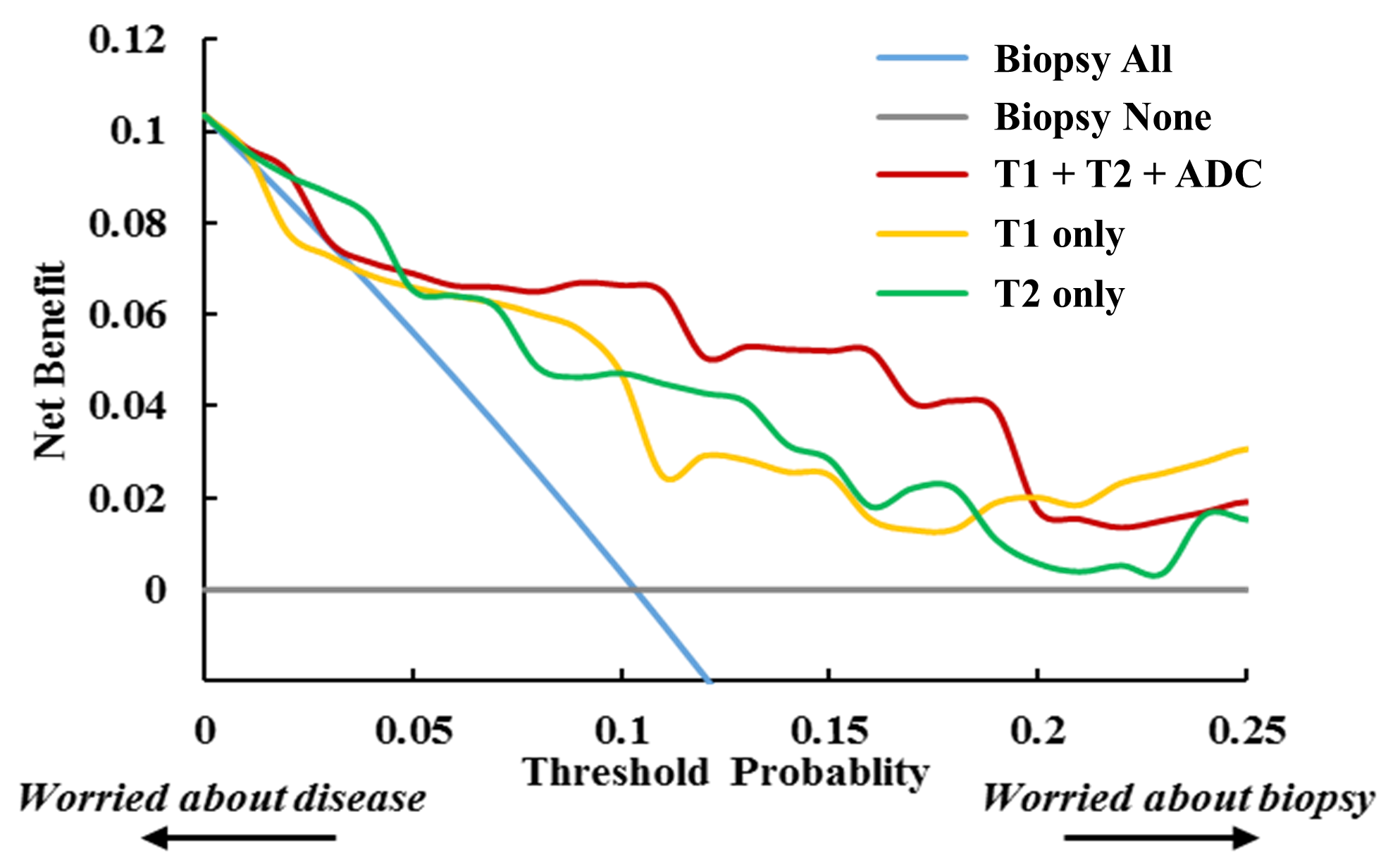
We retrospectively reviewed our prostate MRF institutional database for patients without prior history of diagnosis or treatment of prostate cancer, who underwent a prostate MRF from October 2017 to July 2019, and who had a systematic biopsy up to 6 months following the MRI. An experienced abdominal radiologist re-scored the MRIs based on PI-RADS v2.1 guidelines. MRI-negative patients with PI-RADS 1/2 scores were included. Regions of interest (ROIs) encompassing the right and left lobes of the peripheral zone (PZ) were drawn for three axial slices on ADC and T2 maps, with T2 ROIs copied to inherently co-registered T1 maps (Figure 1). These ROIs were used to compute mean T1, T2, and ADC values of the PZ. Logistic regressions were used to estimate changes in odds of csPCa for increases in mean T1, T2, and ADC values. Decision curve analysis8 was used to compare the net benefit of performing systematic biopsies for every patient with a clinical indication (current clinical standard), with further selecting patients based on mean T1 or T2 values alone, or in combination with mean ADC values of the PZ.RESULTS
Eighty-seven PI-RADS 1/2 patients with negative MRIs and clinically-indicated biopsies were included. Only 9 of those patients had csPCa on biopsy. Each 100 ms increase in mean T1 was associated with 46% reduced odds of csPCa (95%CI: 0.34-0.85, p < 0.01), whereas each 20 ms increase in mean T2 was associated with 61% reduced odds of csPCa (95%CI: 0.16-0.92, p = 0.03). For each 100 mm2/s increase in ADC values, there was a non-significant 36% reduced odds of csPCa (95%CI: 0.47-1.15, p = 0.18). By setting a mean T1 and T2 threshold for biopsy selection of <2200 and <100 ms, respectively, 30% of biopsies could be avoided without missing any csPCa. Moreover, with a linear regression analysis of mean T1 and T2 values, 63% of biopsies could be optimally avoided, at the cost of missing one csPCa (Figure 2). On a decision curve analysis, the combination of mean T1+T2+ADC values and even mean T1 or T2 values alone outperformed the current clinical standard for optimal biopsy decisions in the entire threshold probability range (0-25%). For probability intervals of 0-5%, 5-20%, and 20-25%, respectively, mean T2 alone, a combination of mean T1+T2+ADC and mean T1 alone, had the highest net benefit for biopsy selection (Figure 3).DISCUSSION
Our results show that increases in T1 and T2 values are associated with significantly lower odds of csPCa. Importantly, T1 and T2 outperformed the current clinical standard for biopsy selection in the entire probability threshold range. For instance, using T1 and T2 maps for biopsy selection meant avoiding 63% of all biopsies. The addition of conventional ADC mapping to T1 and T2 maps also improved the net benefit of MRF for biopsy selection in the majority of the probability range (5-20%). Based on current data from Medicare9,10, if this approach is validated, we would avoid up to 180,000 biopsies, 21,600 bleeding or infectious complications, and 5,400 hospitalizations per year. All of which means saving around 360 million USD.CONCLUSION
Compared with the current clinical standard, the use of MRF T1 and T2 maps alone or combined with conventional ADC for biopsy selection significantly reduced the number of unnecessary prostate biopsies, while maintaining optimal detection of csPCa in MRI-negative patients with clinically-indicated biopsies. The prospective validation of these findings is crucial to reduce overdiagnosis as well as reduce the cost and harm of unnecessary biopsies in patients with negative prostate MRIs.Acknowledgements
No acknowledgement found.References
1. Barrett T, Turkbey B, Choyke PL. PI-RADS version 2: What you need to know. Clinical Radiology. 2015;70(11):1165–76.
2. Barrett T, Rajesh A, Rosenkrantz AB, Choyke PL, Turkbey B. PI-RADS version 2.1: one small step for prostate MRI. Clinical Radiology. 2019;74(11):841–52.
3. Wei JT, Barocas D, Carlsson S, Coakley F, Eggener S, Etzioni R, et al. Early Detection of Prostate Cancer: AUA/SUO Guideline Part II: Considerations for a Prostate Biopsy. Journal of Urology. 2023;210(1):54–63.
4. Shiradkar R, Panda A, Leo P, Janowczyk A, Farre X, Janaki N, et al. T1 and T2 MR fingerprinting measurements of prostate cancer and prostatitis correlate with deep learning–derived estimates of epithelium, lumen, and stromal composition on corresponding whole mount histopathology. European Radiology. 2021;31(4):2644.
5. Yu AC, Ponsky LE, Dastmalchian S, Rogers M, Mcgivney D, Griswold MA. Development of a Combined MR Fingerprinting and Diffusion Examination for Prostate. Radiology. 2017;283(3):729–38.
6. Panda A, Obmann VC, Lo WC, Margevicius S, Jiang Y, Schluchter M, et al. MR fingerprinting and ADC mapping for characterization of lesions in the transition zone of the prostate gland. Radiology. 2019;292(3):685–94.
7. Panda A, O’connor G, Lo WC, Jiang Y, Margevicius S, Schluchter M, et al. Targeted Biopsy Validation of Peripheral Zone Prostate Cancer Characterization With Magnetic Resonance Fingerprinting and Diffusion Mapping. Investigative Radiology. 2019;54(8):485–93.
8. Vickers AJ, van Calster B, Steyerberg EW. A simple, step-by-step guide to interpreting decision curve analysis. Diagnostic and Prognostic Research. 2019 Oct 4;3(1):18.
9. Loeb S, Carter HB, Berndt SI, Ricker W, Schaeffer EM. Complications after prostate biopsy: data from SEER-Medicare. J Urol. 2011 Nov;186(5):1830–4.
10. Weiner AB, Manjunath A, Kirsh GM, Scott JA, Concepcion RD, Verniero J, et al. The Cost of Prostate Biopsies and their Complications: A Summary of Data on All Medicare Fee-for-Service Patients over 2 Years. Urol Pract. 2020 Mar;7(2):145–51.
Figures