3337
Testing diagnostic quality after speeding up prostate MRI by reducing the number of echo-trains in T2-weighted TSE.1Magnetic Detection and Imaging, University of Twente, Enschede, Netherlands, 2Department of Radiology, University Medical Center Groningen, Groningen, Netherlands, 3Robotics and Mechatronics, University of Twente, Enschede, Netherlands, 4Minimally Invasive Image-Guided Interventions Center, Radboud University Medical Center, Nijmegen, Netherlands, 5Department of Radiology, Netherlands Cancer Institute, Amsterdam, Netherlands, 6Department of Nuclear Medicine and Molecular Imaging, University Medical Center Groningen, Groningen, Netherlands, 7Department of Applied Mathematics, University of Twente, Enschede, Netherlands
Synopsis
Keywords: Prostate, Prostate, Undersampling, PI-RADS
Motivation: Increasing prostate cancer cases are leading to a rising demand for prostate MRI, which is a time-consuming protocol. Speeding up of this protocol will help relieve the rising pressure on the healthcare system.
Goal(s): To speed up the T2W TSE by undersampling the data, while maintaining the diagnostic outcome.
Approach: Echo-trains with center-lines farthest from the k-space center are removed, to undersample the data semi-incoherently , followed by a Compressed Sense reconstruction.
Results: Up to 17% time gain can be achieved while the diagnostic outcome remains unaffected.
Impact: The scan time of T2W TSE can be reduced by selectively removing echo-trains based on their center-line distance to the k-space center, without affecting the diagnostic outcome, defined by the PI-RADS score and qualitative parameter ratings.
INTRODUCTION
Globally, prostate cancer (PCa) cases are projected to increase from 1.4 million in 2020 [1] to 2.4 million cases by 2040 [2], thus, increasing the demand for prostate MRI, which takes 15-30 minutes scan time depending on if contrast is injected or not. T2-weighted (T2W) turbo spin echo (TSE) is the most time-consuming sequence [3], requiring 4-5 minutes, recommended in at least two planes. Faster mpMRI acquisition could reduce the strain on current resources.This study aimed to shorten the T2W TSE scan time without impacting the prostate MRI evaluation. In the TSE sequence, k-space is sampled using multiple echo-trains. We propose reducing the acquisition time by undersampling k-space semi-incoherently by leaving out echo-trains and retaining image quality by using Compressed Sensing (CS) reconstruction [4]. For CS reconstructions the k-space undersampling should give rise to incoherent noise-like artifacts in the image. Hence increasing incoherence in the undersampling may permit higher undersampling factors.
METHODS
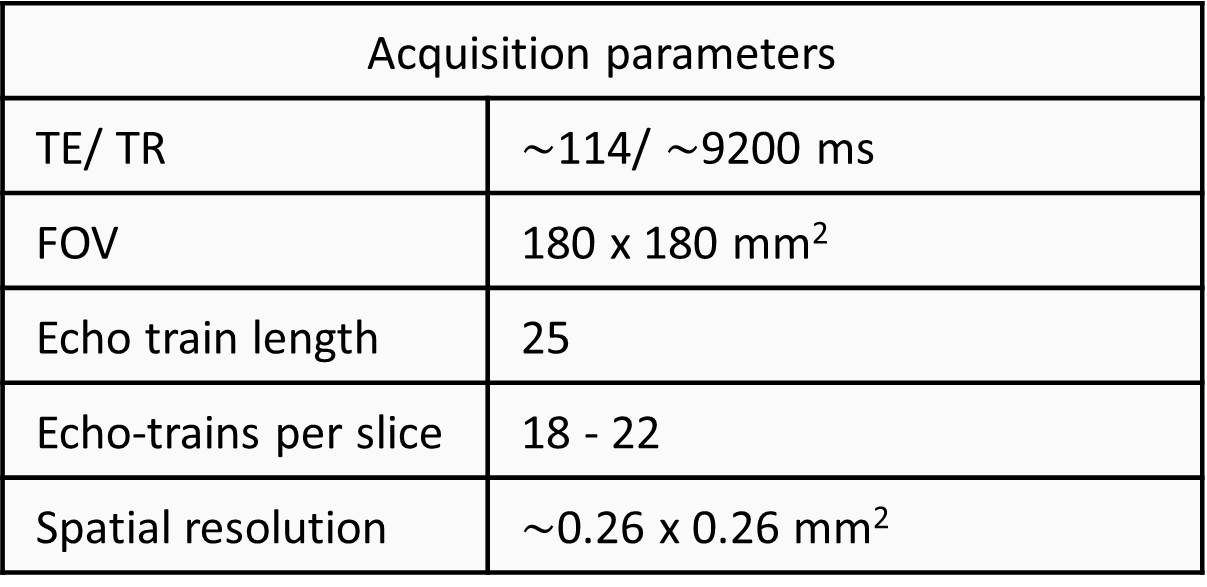
The dataset included T2W TSE from 5 subjects, acquired as per the PI-RADS guidelines at University Medical Center Groningen using a 3T scanner (Skyra, Siemens Healthineers, Erlangen, Germany), with acquisition parameters listed in Table 1. Only cases with a PI-RADS score of ≥ 4 were included to avoid ambiguity in lesion presence and ensure higher certainty of lesion diagnosis, for evaluating the impact of undersampling on diagnostic accuracy.Retrospective undersampling involved removing 2-7 echo-trains with their center lines farthest from the k-space center (Figure 1). CS-based reconstruction (λ= 0.01) was performed using the Berkley Advanced Reconstruction Toolbox [5]. Two radiologists (with > 10 years of experience) evaluated the images by scoring qualitative parameters: sharpness, lesion conspicuity, zonal distinction, capsule delineation, overall image quality, noise levels, and artifacts, with ratings ranging from 1 (poor) to 5 (excellent). Each parameter was evaluated relative to a fully sampled dataset. Additionally, all patients were assigned PI-RADS scores.
The mean of both radiologists’ ratings was calculated for each parameter, at all undersampling levels. Quality was considered satisfactory if the radiologists’ mean rating was ≥ 4. When the PI-RADS score fell below 3, this was defined as a significant negative impact on the diagnostic outcome.
RESULTS
Figure 2 displays both radiologists’ scores for all patients with increasing undersampling. With 3 echo-trains removed, evaluated parameters received a mean score ≥ 4, with an exception seen in artifacts where the mean score was 3.8.Figure 3 illustrates that the PI-RADS scores remain unchanged when up to 3 echo-trains are removed, relative to a fully sampled image.
Removing 4 echo-trains altered 2 out of 10 PI-RADS scores, with only one decreasing to PI-RADS 3. Further undersampling resulted in an increasing number of PI-RADS 3 assignments. For higher levels of undersampling, the radiologists’ PI-RADS score agreement decreased. With 6 and 7 echo-trains removed, two cases were assigned a score of 2 by one radiologist and 4 by the other, indicating a drastic difference in the diagnostic outcome.
Figure 4 demonstrates decreased lesion conspicuity on removing 5 echo-trains.
DISCUSSION
Removing 3 echo-trains resulted in mean scores ∼4 for the evaluated parameters, yielding a time gain of ∼14-17% with minimal impact on PI-RADS score assignment relative to the ground truth. Further undersampling led to decreased PI-RADS scores, which could be attributed to the blurring of margins, inconspicuity of lesions, and degradation in the quality of parameters crucial for prostate MRI evaluation, shown in Figure 3.With 5 echo-trains removed, 2 cases with PI-RADS ≥ 4 were misclassified as PI-RADS 3, indicating less certainty compared to the clearer categorizations of PI-RADS 4 and 5. However, since PI-RADS 3 also warrants biopsy, no lesions could be missed in such cases. On the contrary, a transition from PI-RADS 3-5 to 1-2 would lead to omission of biopsies for lesions that require biopsy, consequently resulting in undertreatment, since PI-RADS 1-2 do not necessitate biopsies. Except for a single outlier, eliminating four or more echo-trains during undersampling resulted in a maximum downgrade to a PI-RADS 3 score.
This study was limited by the diagnostic reliance on T2W images alone. In practice, the addition of DWI scans could enhance certainty and may help maintain accurate PI-RADS scores of 4-5, while T2W imaging remains crucial for extra-prostatic extension evaluation and staging.
CONCLUSION
An easily implementable technique of removing echo-trains can speed up T2W TSE acquisition by up to 17%, while maintaining the diagnostic outcome in form of the PI-RADS score and parameters critical for prostate MRI evaluation. In clinical practice, adding information from DWI may allow further undersampling without underdiagnosing, and help further speed up the T2W acquisition.Acknowledgements
No acknowledgement found.References
1.Sung HA-O, Ferlay J, Siegel RA-O, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. (1542-4863 (Electronic)).
2. Ferlay JA-O, Colombet M, Soerjomataram I, Parkin DA-O, Piñeros M, Znaor AA-O, et al. Global Cancer Observatory: Cancer Tomorrow. Lyon, France: International Agency for Research on Cancer. Available from: https://gco.iarc.fr/tomorrow, accessed [20 April 2023]. (1097-0215 (Electronic)).
3. Prostate Imaging–Reporting and Data System Version 2.1. 2019. https://www.acr.org/-/media/ACR/Files/RADS/PI-RADS/PIRADS-V2-1.pdf. Accessed on 06-11-2023
4. Lustig M, Donoho D, Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2007;58(6):1182-95
5. BART Toolbox for Computational Magnetic Resonance Imagingdoi:10.5281/zenodo.592960.
6. N.Mir et al., Shortening T2-weighted TSE for prostate MRI by reducing the number of echo-trains and using CS reconstruction, Proc. Intl. Soc. Mag. Reson. Med. 31 (2023) 2075
7. Fast MRI in prostate cancer (2021).
Figures
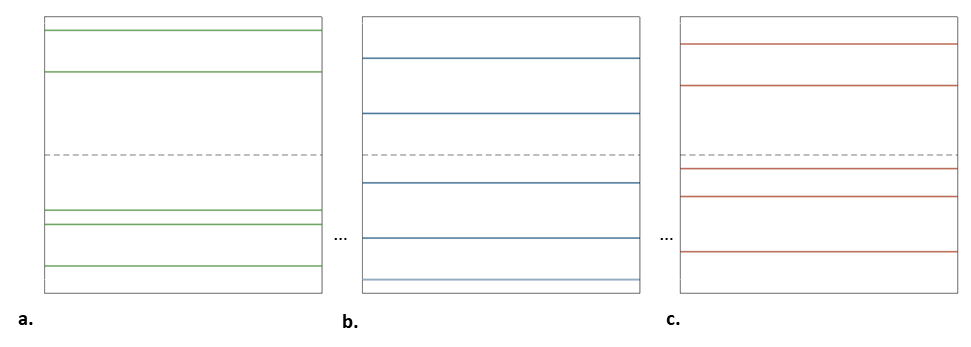
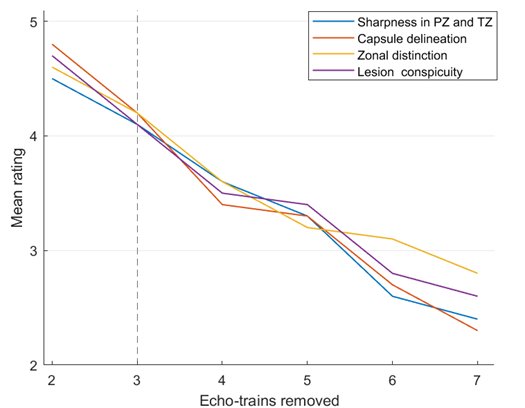
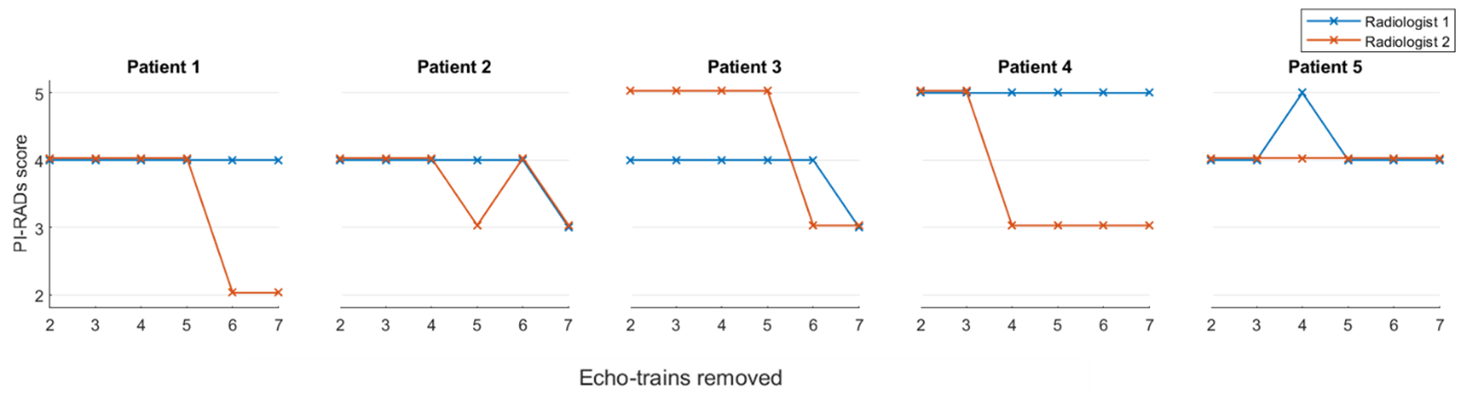
Figure 3: Mean of PI-RADS scores of radiologists 1 and 2, with increasing undersampling. The PI-RADS score remains unaffected by undersampling when 3 echo-trains are removed.
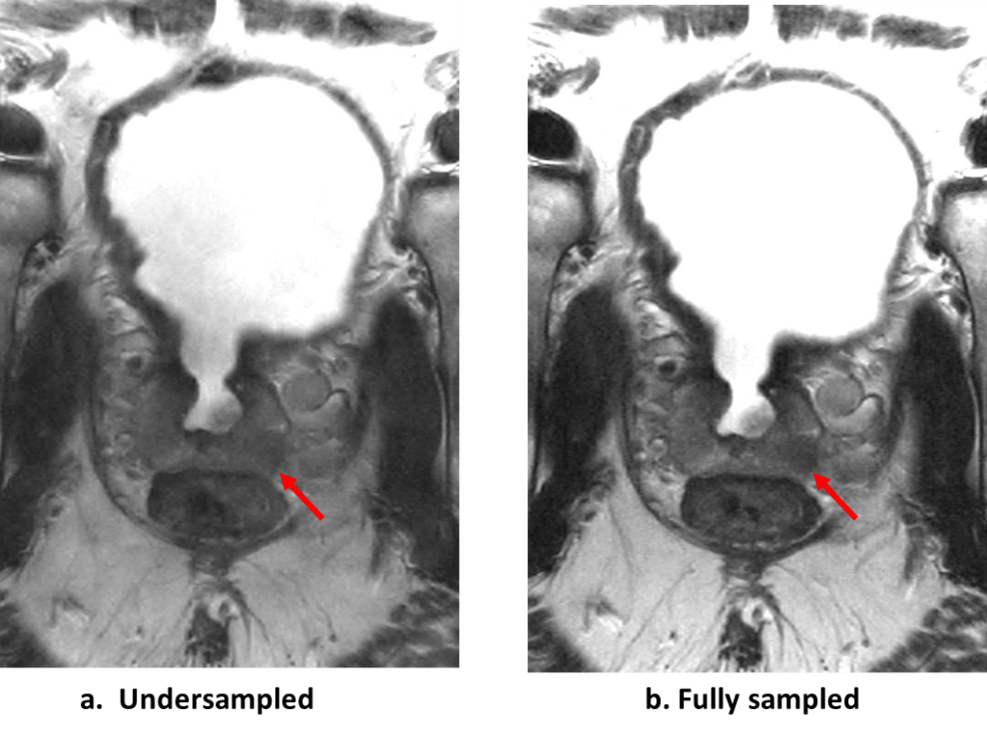
Figure 4: Lesion conspicuity being affected by undersampling. The figure shows a. lower conspicuity of the lesion (mean score = 2.5) due to undersampling by removing 5 echo-trains, b. lesion as seen when fully sampled.