3336
PSMA PET/CT and mpMRI discrepancies in prostate cancer detection with whole-mount histopathology gold standard1Radiology, UCLA, Los Angeles, CA, United States, 2Statistics, UCLA, Los Angeles, CA, United States, 3Pathology, UCLA, Los Angeles, CA, United States, 4Urology, UCLA, Los Angeles, CA, United States, 5Molecular and Medical Pharmacology - Nuclear Medicine, UCLA, Los Angeles, CA, United States
Synopsis
Keywords: Prostate, Prostate
Motivation: In prostate cancer (PCa), multiparametric MRI (mpMRI) and PSMA-PET aid pre-surgical assessment. This study evaluates parameters linked to the agreement/disagreement of PSMA-PET and mpMRI with histopathology.
Goal(s): To evaluate the concordance between PSMA-PET, mpMRI, and histopathology in PCa lesion identification.
Approach: Patients with PSMA-PET, mpMRI, and histopathology data were analyzed. Imaging lesions were contoured independently. Sensitivity and agreement were assessed. Logistic regression models examined factors affecting concordance.
Results: Among 114 patients, PSMA-PET and mpMRI identified 170 and 138 lesions, respectively. Tumor aggressiveness and size impacted agreement. Higher SUVmax on PSMA-PET and higher ISUP grade and size on pathology were associated with concordance.
Impact: This work improves prostate cancer diagnosis by identifying key factors influencing the agreement between PSMA-PET, mpMRI, and histopathology, offering valuable insights for more precise pre-surgical assessments.
Background
Multiparametric MRI (mpMRI) and PSMA-PET are complementary imaging modalities used in the pre-surgical evaluation of patients with prostate cancer (PCa). The aim of this analysis was to evaluate the imaging and pathology parameters associated with PSMA-PET and mpMRI agreement/disagreement with each other and with gold standard whole mount histopathology (WMHP).Methods
We screened for inclusion in this retrospective analysis patients undergoing radical prostatectomy (RP) with pre-surgical PSMA-PET and mpMRI. Included patients had the two imaging scans done less than 3 months apart, and WMHP slides available, with ISUP grade group classification and a detailed description of the lesion location (level and clockface). Two nuclear medicine physicians and 2 radiologists blindly and independently contoured PCa lesions on PSMA-PET and mpMRI, respectively. We used a majority rule (2:1) with a third reader for each modality in case of discordant findings among the two readers. We extracted quantitative measures on a lesion-level and patient-level on PSMA PET (SUVmean, SUVmax, lesion volume) and mpMRI (PI-RADS, prostate volume). We fused the PET and MRI using a fusion workflow on MIM software, and assessed for agreement/disagreement visually, based on the overlapping lesion contours. Three readers in consensus used the WMHP slides and the lesion location description to establish the agreement/disagreement of imaging-identified lesions with the gold standard pathology. In case this was deemed difficult by the readers, a genito-urinary pathologist was consulted facilitate the consensus decision. We used independent samples t-test and one-way ANOVA to assess group differences. We used univariable and multivariable logistic regression models to assess the association of clinical, pathological, and imaging variables with PSMA-PET and mpMRI agreement/disagreement with each other and with pathology.Results
The cohort included 114 patients, and 175 pathology lesions were identified (ISUP 3, n=22; ISUP>3, n=153). mpMRI and PSMA PET identified 138 and 170 lesions, respectively. Sensitivity for ISUP>3 lesions was 79% and 87% for mpMRI and PSMA-PET, respectively. 115/153 (76%) ISUP> 3 lesions were correctly identified, and 14/153 (9%) were missed by both imaging modalities, respectively. 5/153 (3%) were correctly identified by mpMRI and missed by PSMA-PET, 17/153 (11%) were correctly identified by PSMA-PET and missed by mpMRI. Lesion’s ISUP grade group and size on pathology were significantly lower in mpMRI- compared to mpMRI+ and in PET- compared to PET+ lesions. SUVmax and SUVmean were significantly higher in PET+/MRI+ than PET+/MRI- lesions. Lesion’s ISUP grade group and size were significantly correlated to PSMA-PET and mpMRI agreement, whereas PSMA-PET metrics were not. Logistic regression model showed that lesions with lower ISUP, smaller size, and lack of aggressive prostate cancer features on pathology (cribriform pattern and intraductal carcinoma) havehigher likelihood of being missed by PET and mpMRI and of PET/MRI disagreement.Conclusions
Higher SUVmax, SUVmean, and tumor volume on PSMA-PET were associated with a TP finding on PSMA-PET, higher ISUP grade group and size on pathology were associated with a TP finding on both PSMA-PET and mpMRI, and with agreement between PSMA-PET and mpMRI.Acknowledgements
No acknowledgement found.References
No reference found.Figures
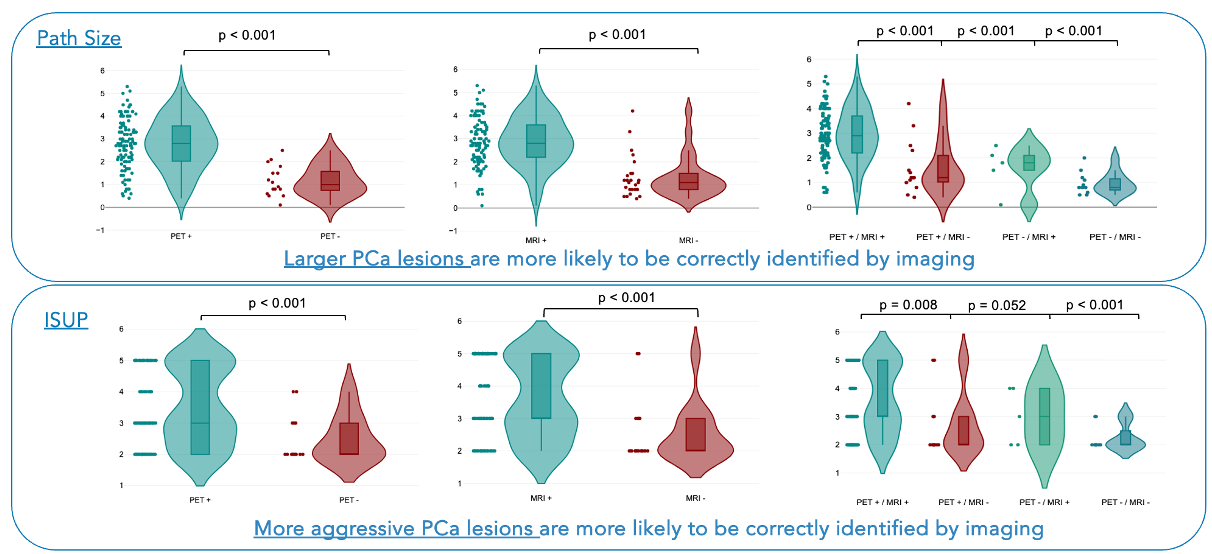
Correlation of pathology parameters (lesion size and ISUP grade group) and imaging findings: Larger PCa lesions and those with higher ISUP grade group were more likely to be correctly identified by both PET and MRI.
Lesions correctly identified by both PET and MRI had larger size than any other group (FN lesions on both or lesions missed by one of the two imaging modalities). Lesions correctly identified by both PET and MRI had higher ISUP grade group than those missed by both and those missed by MRI only.