3334
Accuracy of PIRADS 2.1 scoring system to Screen Prostate Cancer in a Ugandan population1ECUREI, Kampala, Uganda
Synopsis
Keywords: Prostate, Screening, PIRADS
Motivation: Prostate cancer is highly incident in Africa. Early screening and detection is recommended to lower this rate. BpMRI and PIRADS are used to detect, stage prostate cancer. The accuracy of PIRADS in an African population hasn’t been determined
Goal(s): Determine the accuracy of PIRADs to screen Prostate cancer in an African population
Approach: We assessed the accuracy of PIRADS alone, PIRADS and PSAD, PIRADS and ADC, PIRADS, PSAD and ADC using the AUC to discriminate a positive histological prostate case
Results: PIRADS had AUC 0.70, combination of PIRADS V2.1 and PSAD had AUC 0.73, combination of PIRADS, PSAD and ADC had AUC 0.72
Impact: PIRADS accurately predicts PCa satisfactorily AUC 70%. It may be used in an African population in combination with clinical information and history. This is because they were some cases graded as PIRADS 2 and yet had a high gleason score.
Introduction
Prostate Cancer (PCa) has been shown to be highly incident (29.7 per 100,000 population) in Africa1. In an effort to lower such a rate, early screening and detection especially among the risky population has been shown to be effective, especially in low-resource settings like Uganda2. BpMRI has been noted as a safe and valuable imaging modality in PCa detection, staging, and active surveillance and it matches the detection rates3. To facilitate global standardization and to reduce variation in the acquisition, interpretation, and reporting of prostate MRI, the Prostate Imaging Reporting and Data System(PIRADS) has been introduced4. Upgraded in 2019 to version 2.1, PIRADS and Bp MRI have been shown to have good accuracy in screening for clinically significant prostate cancer. The PIRADS scoring system is intended to be a living document, informed by, and building on clinical experience and research worldwide. It should therefore be tested and validated for different healthcare settings. There is hardly any literature on the applicability and accuracy of the PIRADS 2.1 scoring system in screening for PCa in sub-Saharan Africa and thus this study.Methods
We retrospectively reviewed prostate imaging requisitions, prostate bpMRI images, prostate MRI reports, and prostate histology reports including the Gleason score at facility A, in Kampala Uganda between 2017 July and December 2021. The inclusion criteria were patients presenting for MRI prostate screening within the study period, for whom the required clinical, laboratory, histology, and MRI data was available. Patients had been referred based on one or more of the following; high PSA, suspicious DRE, positive family history, and suspicious nodule on TRUS were consecutively selected. BpMRI using a Phillips 1.5 Tesla Achieva was done using surface body coils. The Diffusion Weighted Imaging employed a b-value of 1500-2000s/mm2. Images stored in the PACS system were retrieved, re-read, and graded using a PIRADS V2.1 by two radiologists with three to five years’ experience of PIRADS application and agreed by consensus to the PIRADS scores. Biopsy results were reviewed and the Gleason score was documented. Biopsy had been performed using TRUS guidance based on the MRI reports. Clinical, demographic, and laboratory information was abstracted from the patients’ imaging requisitions which included demographic data, PSA, prostate volume, the histopathological diagnosis, and the Gleason score. We assessed the ability of PIRADS alone, PIRADS and prostate-specific antigen density (PSAD), PIRADS and Apparent Diffusion Coefficient (ADC), and PIRADS, PSAD, and ADC-combination in predicting a positive histological cancer prostate case. The PSA density (PSAD) was categorized into 3 as <0.07, 0.08-0.15, and >0.15. The evaluation of PIRADS V 2.1 as a screening test for PCa was done using logistic regression analysis, the Receiver Operating Characteristic (ROC) curve, and the Area Under the Curve (AUC)7.Results
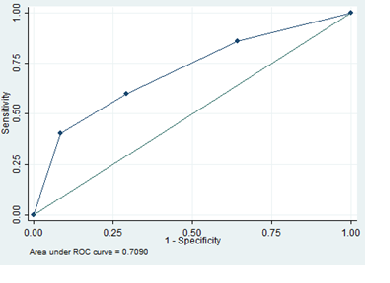
In our study, we reviewed a total of 234 patient records and of these majority (99) were aged between 65-74 years. Out of the total number, 48.7%(117) were PCa histology-confirmed cases. Of these, 33.3% had cancer located in both transitional and peripheral zone and 46 had a PIRADS score 5 while 16 had a PIRADS score 2Accuracy of PIRADS- the AUC was 0.70 with 95% CI (0.64-0.77) implying that PIRADS V2.1 as a screening tool has a satisfactory predictive ability to discriminate PCa from normal participants in Uganda.
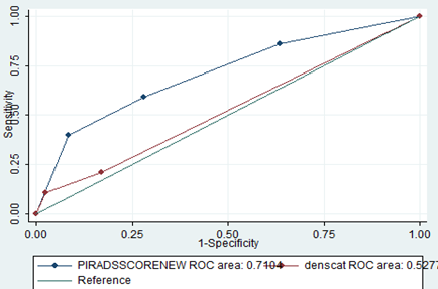
Combining PIRADS V2.1 and PSAD- the AUC score of 0.71 implies that it has a satisfactory predictive ability to discriminate PCa from normal participants in Uganda.
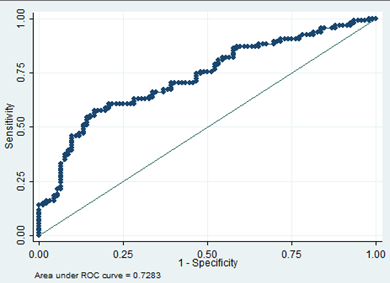
Combining PIRADS V2.1 and ADC for discriminating PCa- AUC score of 0.73 implies that it has a good predictive ability to discriminate PCa from normal participants in Uganda.
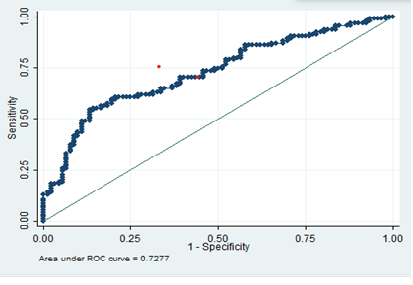
Combining PIRADS V2.1, PSAD, and ADC to discriminate PCa- that the logistic model had a good predictive ability (AUC 0.72) to discriminate PCa from normal participants in Uganda
A comparison of the 3 models' results indicates that the equality of the area under the curve using the Chi-square test yielded a P-value of 0.26, suggesting that there is no statistically significant discrimination ability among these three models as further emphasized by the area under the curve.
Discussion
The AUC for PIRADS alone was 0.70. This score is lower than in other studies. A study done by Moritz et al in a cohort of 82 patients found an AUC score of 0.836 while Guan et al found 0.9357. This finding may be explained by the fact that the majority of the cases had a Gleason score of 6 and were localized in the peripheral zone. Some of such localized tumors have been shown to be infiltrative tumors and are frequently missed on MRI 8Acknowledgements
We acknowledge Ernest Cook Ultrasound Research and Education Institute for the resources provided to support this studyReferences
1. Wang L, Lu B, He M, Wang Y, Wang Z, Du L. Prostate cancer incidence and mortality: global status and temporal trends in 89 countries from 2000 to 2019. Front Public Health. 2022;10:811044. 2. Okuku F, Orem J, Holoya G, De Boer C, Thompson CL, Cooney MM. Prostate cancer burden at the Uganda cancer institute. J Glob Oncol. 2016;2(4):181-185.
3. Pesapane F, Acquasanta M, Meo RD, et al. Comparison of sensitivity and specificity of biparametric versus multiparametric prostate mri in the detection of prostate cancer in 431 men with elevated prostate-specific antigen levels. Diagnostics. 2021;11(7):1223.
4. Weinreb JC, Barentsz JO, Choyke PL, et al. PI-RADS prostate imaging–reporting and data system: 2015, version 2. Eur Urol. 2016;69(1):16-40.
5. Hajian-Tilaki K. Receiver operating characteristic (ROC) curve analysis for medical diagnostic test evaluation. Casp J Intern Med. 2013;4(2):627.
6. Kasel-Seibert M, Lehmann T, Aschenbach R, et al. Assessment of PI-RADS v2 for the detection of prostate cancer. Eur J Radiol. 2016;85(4):726-731.
7. Cai GH, Yang QH, Chen WB, Liu QY, Zeng YR, Zeng YJ. Diagnostic Performance of PI-RADS v2, Proposed Adjusted PI-RADS v2 and Biparametric Magnetic Resonance Imaging for Prostate Cancer Detection: A Preliminary Study. Curr Oncol. 2021;28(3):1823-1834.
8. Hötker AM, Blüthgen C, Rupp NJ, Schneider AF, Eberli D, Donati OF. Comparison of the PI-RADS 2.1 scoring system to PI-RADS 2.0: Impact on diagnostic accuracy and inter-reader agreement. Plos One. 2020;15(10):e0239975.
Figures