3333
Development of preoperative nomograms to predict the risk of overall and multifocal positive surgical margin after radical prostatectomy1Peking Union Medical College Hospital, Beijing, China
Synopsis
Keywords: Prostate, Prostate
Motivation: Preoperative prediction of the risk of positive surgical margin (PSM) is important for optimal treatment decision-making in patients with prostate cancer.
Goal(s): To develop preoperative nomograms using risk factors based on clinicopathological and MRI for predicting the risk of PSM after radical prostatectomy.
Approach: Preoperative clinicopathological factors and MRI-based features were recorded for analysis. The presence or absence of PSM (oPSM) at pathology and the multifocality of PSM (mPSM) were evaluated.
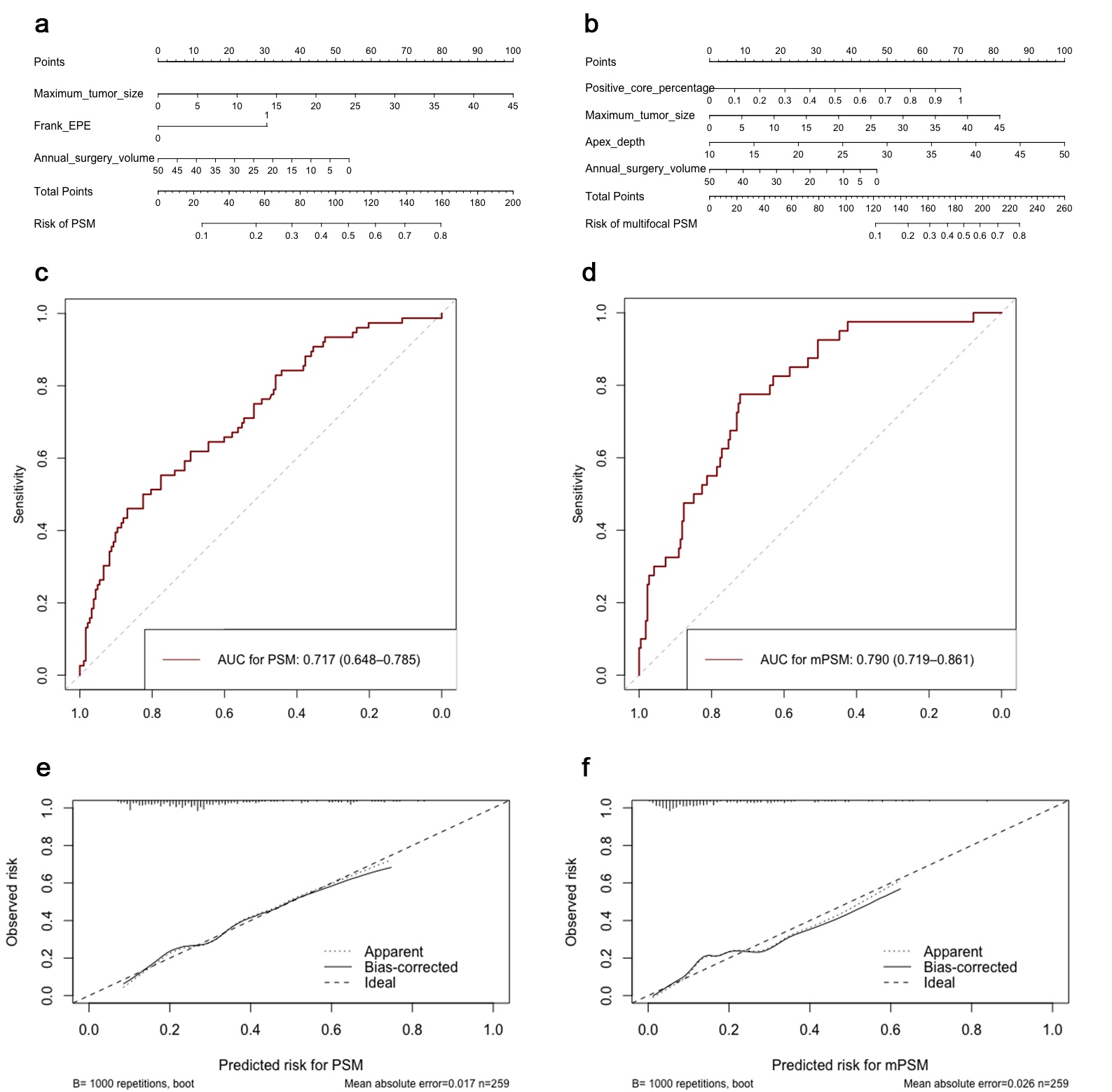
Results: The nomogram for oPSM reached an AUC of 0.717 in development and 0.716 in internal verification. The AUC of the nomogram for mPSM was 0.790 in both development and internal verification.
Impact: The proposed nomograms showed good performance and were feasible in predicting oPSM and mPSM. The evaluation of risk factors and the application of nomograms preoperatively might facilitate individualized management of prostate cancer.
Introduction
Positive surgical margin (PSM) in radical prostatectomy (RP) specimens usually indicates an unfavorable prognosis [1-3]. Multifocality, one of the characteristics of PSM, indicates a poorer prognosis with an even higher risk for biochemical recurrence [4, 5]. Therefore, preoperative prediction of the risk of PSM is important for optimal treatment decision-making and selection of the surgical procedure in patients with PCa [6, 7]. Presently, some studies have attempted to propose algorithms or nomograms to facilitate individualized risk prediction of PSM [8, 9]. However, these models have usually been based solely on clinicopathological data or certain imaging features, and a more comprehensive preoperative model including clinicopathological data and MRI features is needed. Therefore, in this study, we aimed to construct a preoperative nomogram using clinicopathological and MRI-based risk factors for predicting the risk of PSM after RP in patients with PCa, and a nomogram for the adverse characteristic of PSM—the multifocality—to facilitate the individual management of PCa.Methods
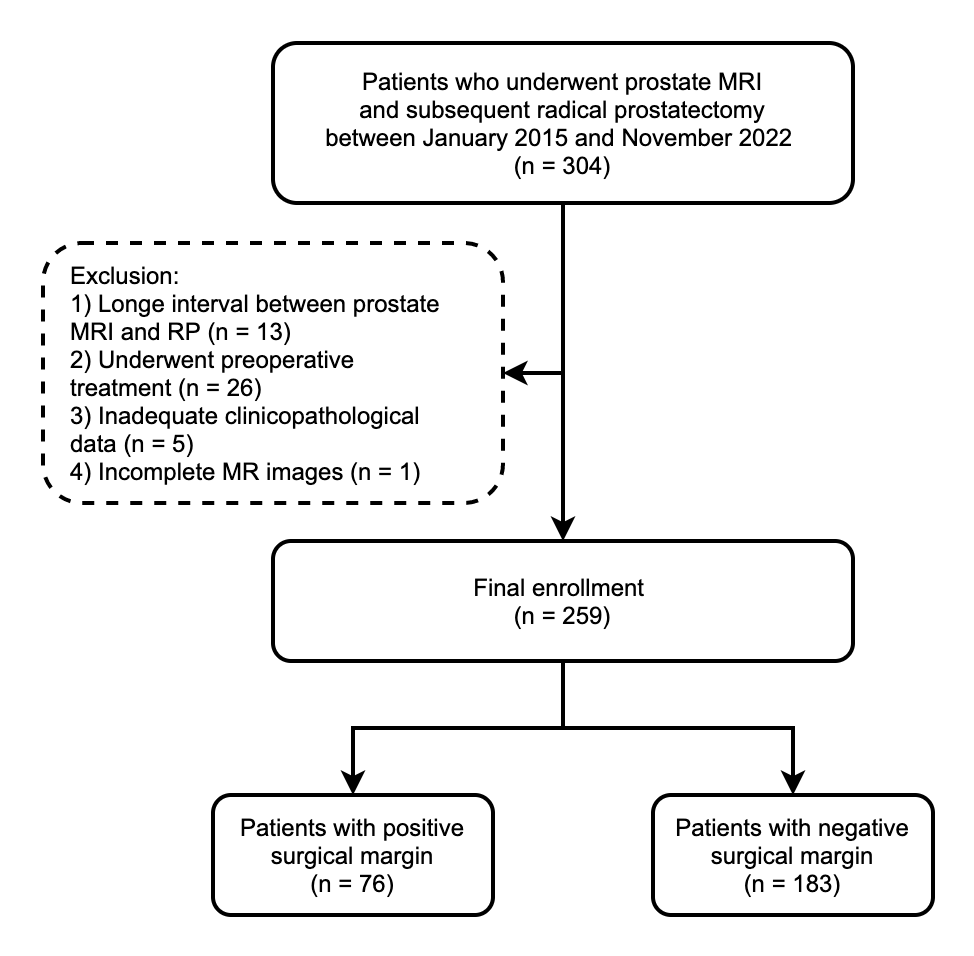
The IRB approved this retrospective study. Consecutive patients who had undergone preoperative prostate multiparametric MRI (mpMRI) followed by laparoscopic RP at our facility between January 2015 and November 2022 were included retrospectively. Figure 1 displays the flow diagram of patient recruitment in this study. Potential predictors were selected based on a literature search and clinical experience. Clinicopathological variables, including patient’s age, prostate-specific antigen (PSA) level, International Society of Urological Pathology (ISUP) grade of biopsy, and clinical T stage, were obtained from medical records. The radiologist evaluated the following predictive factors: (1) prostate volume and prostate apex depth; (2) PI-RADS category of the index lesions, maximum tumor diameter on MRI, capsule contact length (CCL) of the lesions [10], frank EPE visible at MRI, and tumor’s distance to the proximal membranous urethra (UD). The presence or absence of PSM (overall PSM [oPSM]) at pathology and the multifocality of PSM (mPSM) were evaluated by experienced pathologists. First, binary logistic regression was used for univariate analysis to select candidate risk factors. Then, the LASSO method was used for the subsequent screening of variables [11]. The nomogram was used to calculate and visualize the risk probability of individual patients. The area under the receiver operating characteristic curve (AUC) values of the nomograms were recorded. P values < 0.05 were considered significant. All analyses were performed using the R software (version 4.2.1).Results
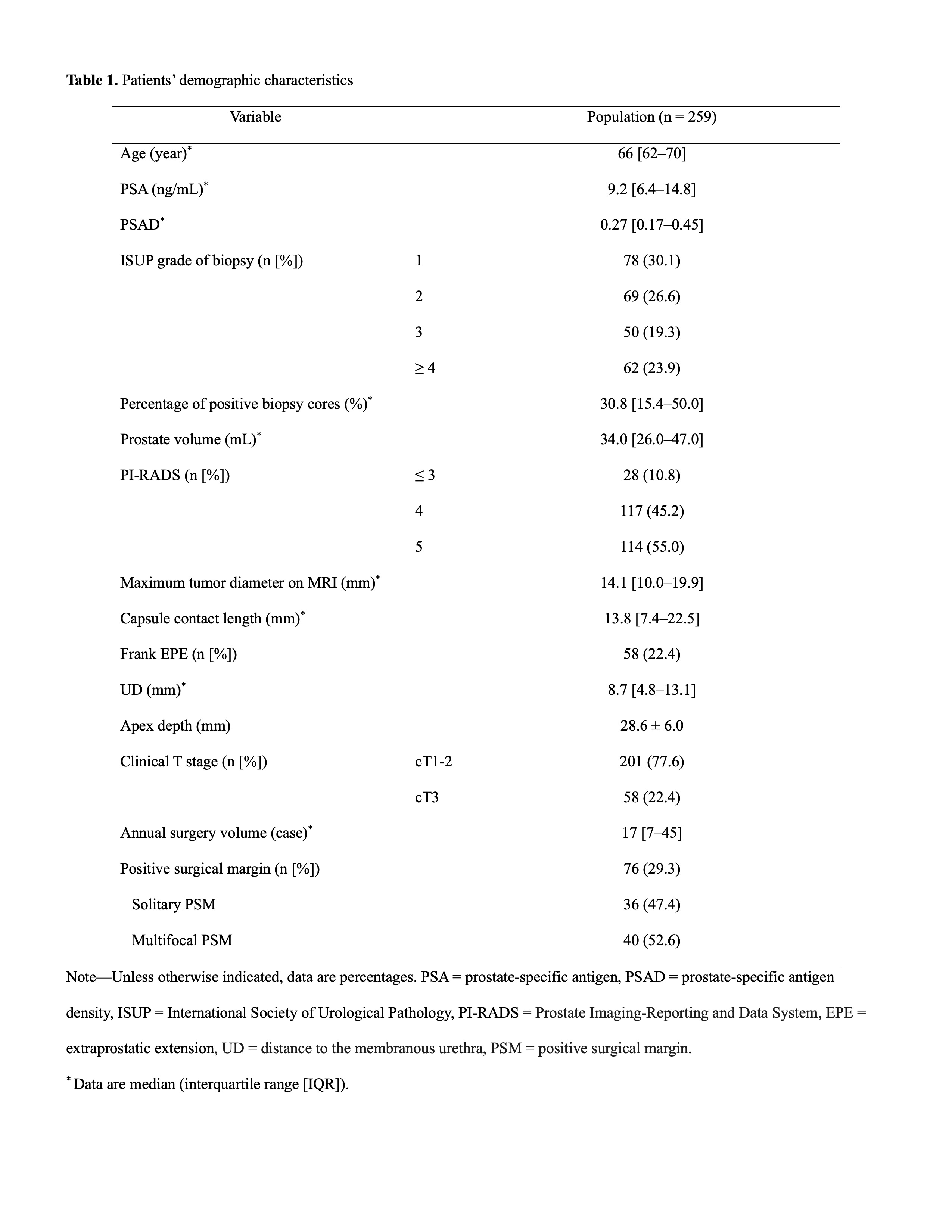
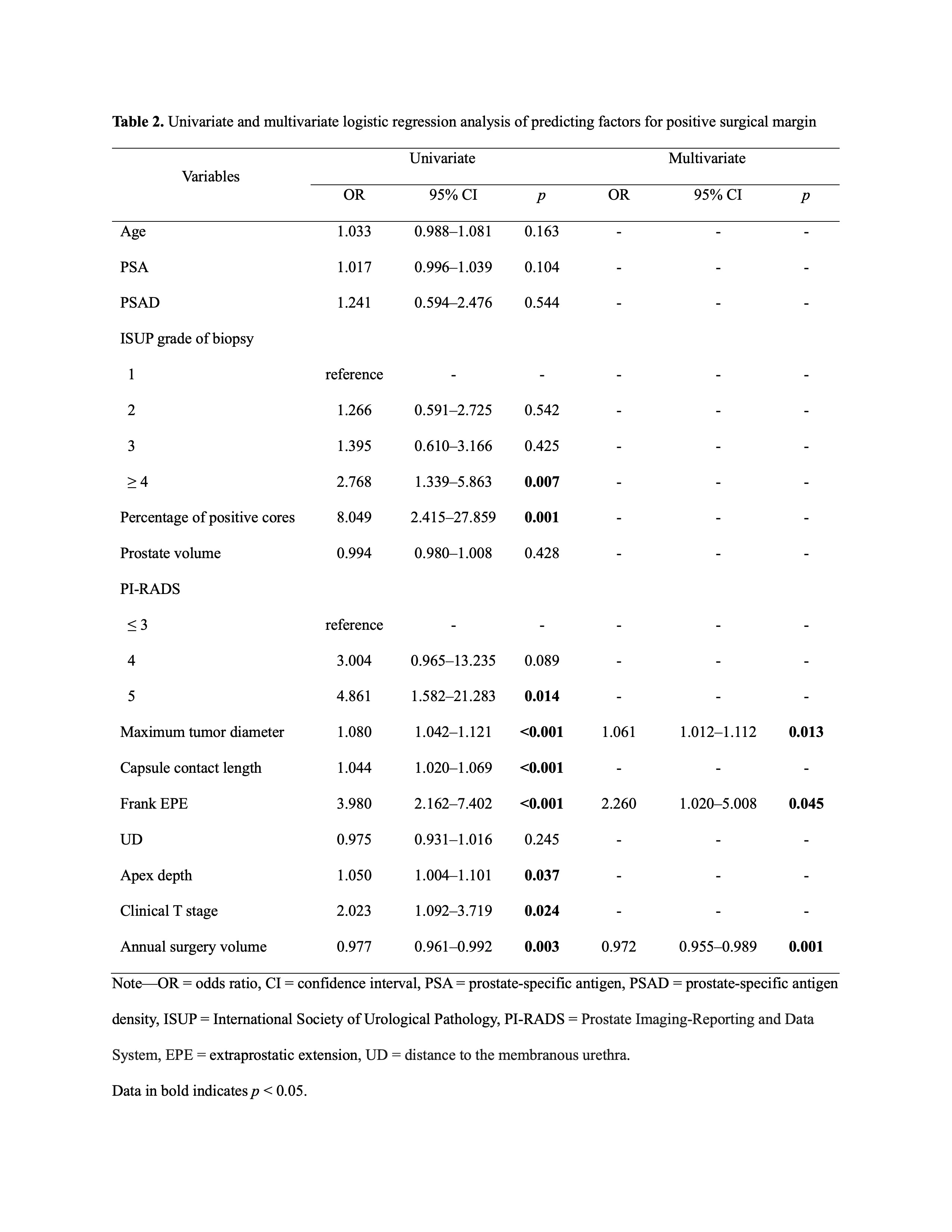
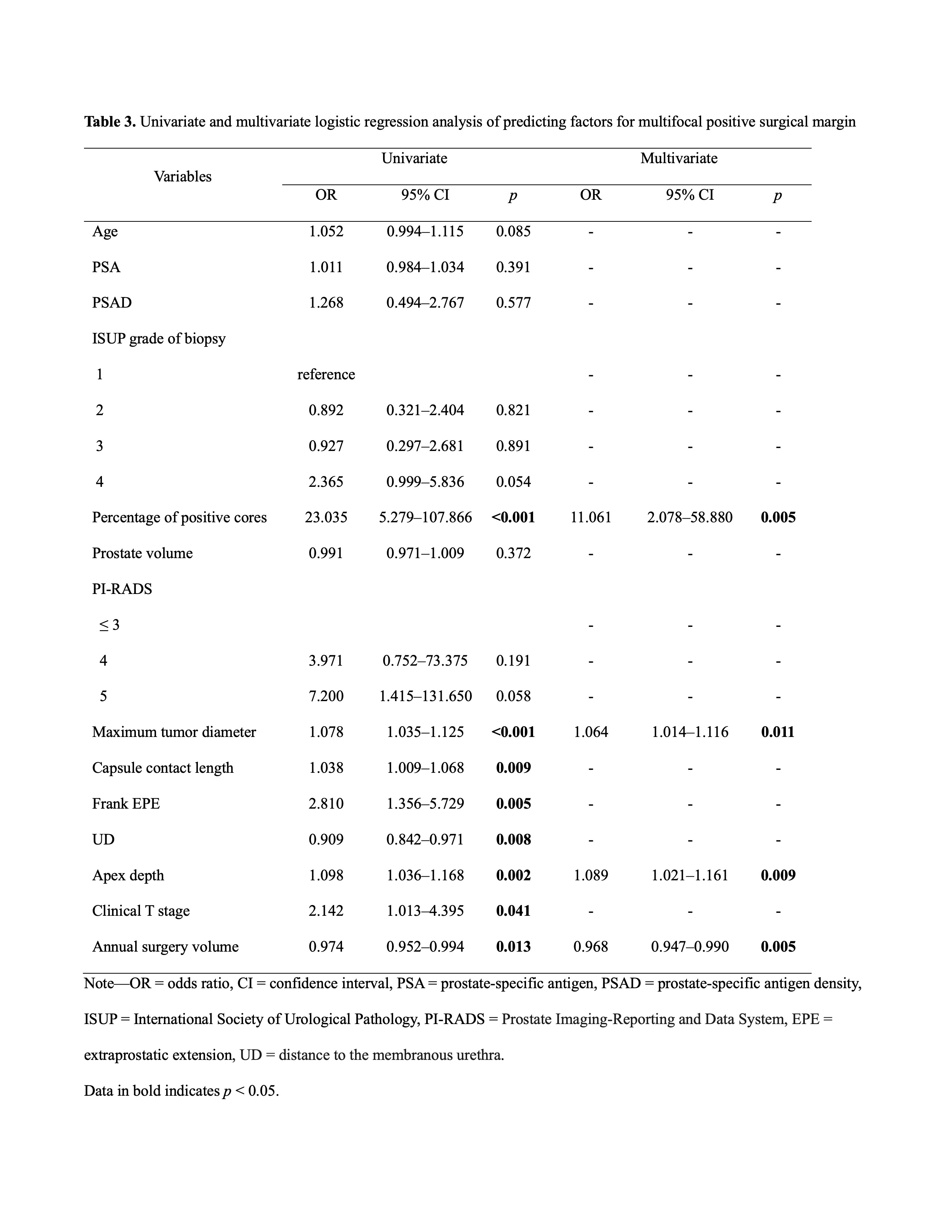
In total, 259 patients were included in this study. PSM was identified in 29.3% (76/259) of patients; 40 (52.6%) of them had multifocal PSM and 36 (47.4%) had solitary PSM (Table 1). In the univariate analysis, nine variables were significantly associated with oPSM (all p < 0.05). After the LASSO regression, three prediction factors were finally obtained, including the maximum tumor diameter, frank EPE, and annual surgery volume (all p < 0.05) (Table 2). The AUC of the model was 0.717 (95% CI: 0.648–0.785) (Figure 2c), and after 1000-bootstrap internal verification, the AUC value of the model was 0.716 (95% CI: 0.714–0.718). Moreover, the calibration of the model was good with a mean absolute error of 0.017 and p = 0.972 by the Hosmer–Lemeshow test (Figure 2e). In the univariate analysis, eight variables were found to be associated with mPSM (all p < 0.05). After LASSO regression, the final model included the percentage of positive cores, maximum tumor diameter, apex depth, and annual surgery volume (all p < 0.05) (Table 3). The AUC of the model was 0.790 (95% CI: 0.719–0.861), and after 1000-bootstrap internal verification, the AUC value was 0.790 (95% CI: 0.788–0.793) (Figure 2d). The nomogram for mPSM is depicted in Figure 2b. The calibration curve of the model showed a good calibration with a mean absolute error of 0.026 and p = 0.914 by the Hosmer–Lemeshow test (Figure 2f).Discussion
In this study, we found a difference in the independent risk factors for oPSM and mPSM. The maximum tumor diameter and frank EPE observed on MRI, and the surgeon’s annual surgery volume were the independent risk factors for oPSM. As for predicting mPSM, the percentage of positive cores in the biopsy, maximum tumor diameter and prostate apex depth measured on MRI, and surgeon’s annual surgery volume were the independent risk factors. Based on the selected risk factors, the preoperative prediction models for oPSM and mPSM were constructed, with AUC of 0.717 and 0.790, respectively.Conclusion
In conclusion, this study developed individual nomograms to predict the risks of oPSM and mPSM. Both nomograms showed good diagnostic performance for preoperative evaluation of the risk of PSM and might facilitate more individualized management of PCa patients who are candidates for surgery.Acknowledgements
No acknowledgement found.References
1 Zhang L, Zhao H, Wu B, Zha Z, Yuan J, Feng Y (2020) Predictive Factors for Positive Surgical Margins in Patients With Prostate Cancer After Radical Prostatectomy: A Systematic Review and Meta-Analysis. Front Oncol 10:539592
2 Yossepowitch O, Briganti A, Eastham JA, et al (2014) Positive surgical margins after radical prostatectomy: a systematic review and contemporary update. Eur Urol 65:303-313
3 Matti B, Reeves F, Prouse M, Zargar-Shoshtari K (2021) The impact of the extent and location of positive surgical margins on the risk of biochemical recurrence following radical prostatectomy in men with Gleason 7 prostate cancers. Prostate 81:1428-1434
4 Carbonell E, Matheu R, Muni M, et al (2022) The Effect of Adverse Surgical Margins on the Risk of Biochemical Recurrence after Robotic-Assisted Radical Prostatectomy. Biomedicines 10
5 Martini A, Gandaglia G, Fossati N, et al (2021) Defining Clinically Meaningful Positive Surgical Margins in Patients Undergoing Radical Prostatectomy for Localised Prostate Cancer. European Urology Oncology 4:42-48
6 Devos G, Devlies W, De Meerleer G, et al (2021) Neoadjuvant hormonal therapy before radical prostatectomy in high-risk prostate cancer. Nat Rev Urol 18:739-762
7 Ravi P, Kwak L, Xie W, et al (2022) Neoadjuvant Novel Hormonal Therapy Followed by Prostatectomy versus Up-Front Prostatectomy for High-Risk Prostate Cancer: A Comparative Analysis. J Urol 208:838-845
8 Hao Y, Zhang Q, Hang J, Xu L, Zhang S, Guo H (2022) Development of a Prediction Model for Positive Surgical Margin in Robot-Assisted Laparoscopic Radical Prostatectomy. Current oncology 29:9560-9571
9 Tian X-J, Wang Z-L, Li G, et al (2019) Development and validation of a preoperative nomogram for predicting positive surgical margins after laparoscopic radical prostatectomy. Chinese medical journal 132:928-934
10 Xu L, Zhang G, Zhang X, et al (2021) External Validation of the Extraprostatic Extension Grade on MRI and Its Incremental Value to Clinical Models for Assessing Extraprostatic Cancer. Front Oncol 11:655093
11 Zhang Z, Tian Y, Bai L, Xiahou J, Hancock E (2017) High-order covariate interacted Lasso for feature selection. Pattern Recognition Letters 87:139-146
Figures