3332
Advanced Prostate Cancer Characterization: Enhanced Tissue Compartment Estimation with Extended Grid Sampling and HM-MRI1Radiology, University of Chicago, Chicago, IL, United States, 2Pathology, University of Chicago, Chicago, IL, United States
Synopsis
Keywords: Prostate, Prostate
Motivation: Introduction of Extended Grid Sampling (EGS) to overcome the limitations of Hybrid Multidimensional MRI (HM-MRI) in prostate cancer (PCa) detection.
Goal(s): Our primary goal is to assess the effectiveness of EGS in improving the accuracy of PCa detection and lesion extension using HM-MRI.
Approach: Integrate EGS data with standard HM-MRI, utilizing biexponential fits for short and long T2 component estimation, followed by joint analysis, and risk map generation to enhance the precision of prostate cancer detection and characterization.
Results: EGS integrated with HM-MRI can provide more accurate delineation of prostate tissue compartments, notably improving the detection of prostate cancer lesions.
Impact: By enhancing prostate cancer (PCa) detection accuracy with Extended Grid Sampling (EGS) integrated into Hybrid Multidimensional MRI (HM-MRI), we empower clinicians to make more precise diagnoses and treatment decisions, directly benefiting patients.
Introduction
The Hybrid Multidimensional MRI (HM-MRI) has emerged as an effective tool for prostate cancer (PCa) detection. HM-MRI is an innovative approach to quantifying the composition of epithelium, stroma, and lumen non-invasively1. It has been validated against histological data2 and it outperformed expert radiologists in a clinical trial 3. Despite these advances, HM-MRI faces challenges in detecting cancers with inherently low T2 and ADC values, leading to a significant loss of cancer signal. To overcome these limitations, we propose Extended Grid Sampling (EGS). EGS collects additional data points for short and long TE values at a b-value of 0.Methods
EGS data were obtained for eight patients who underwent clinical MRI with an endorectal coil (ERC MRI) and a 16-channel pelvic array coil on a Philips 3.0 T Ingenia scanner. A series of T2-weighted images in axial, coronal, and sagittal views were acquired, alongside ADC maps at different b-values. The HM-MRI scanning produced a 4×4 matrix of hybrid measurements across distinct b and TE combinations. EGS data points were extracted by sampling from TE=9 ms to 300 ms with a 9 ms gap for b = 0 to complement the HM-MRI data. EGS data points were fit with a biexponential function to estimate a long T2 and short T2 component. The amplitude and value of the short T2 component were used to constrain the fit parameters for the epithelium and stroma in subsequent HM-MRI analysis. The lumen compartment was considered equivalent to the amplitude of the long T2 component. The EGS data points were combined with HM-MRI data points with proper normalization, and a fit to estimate the three compartments was performed. This provided a 2D map of epithelium, stroma, and lumen across different prostate MRI slices. Finally, a risk map was generated by selecting voxels with high epithelium and low lumen density, in addition to applying a size criterion. We determined whether the risk map was consistent with T2W images and the results of biopsy.Results
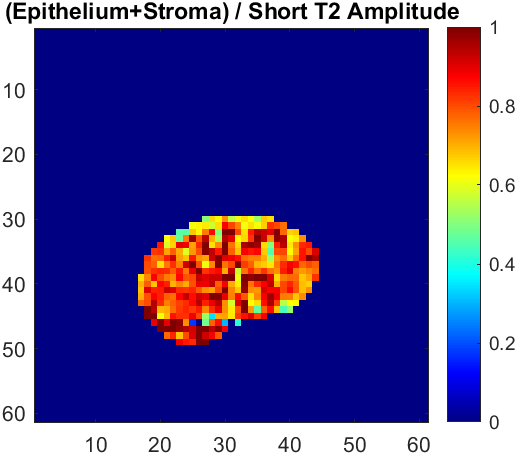
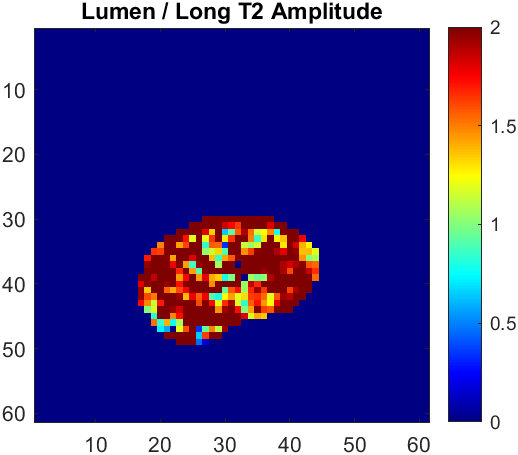
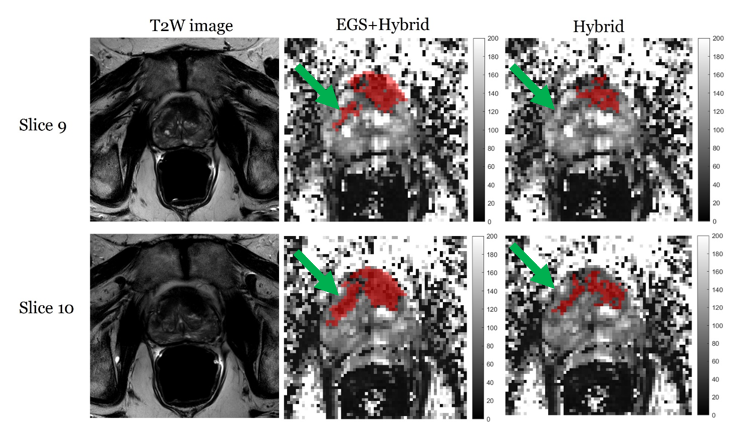
Lumen volumes derived from the standard HM-MRI fit were consistently larger than the long T2 component amplitudes obtained from the biexponential EGS data fit (Figure 2). Conversely, the combined epithelium and stroma volumes from standard HM-MRI were smaller than the amplitude of the short T2 component from EGS data fit (Figure 1). The EGS data merged with HM-MRI matrix (EGS+hybrid) analysis provides a more accurate description of a lesion, as exemplified in Figure 3. The biopsy for this case confirmed a Gleason Score (GS) 3+4 lesion in the TZ. The EGS+hybrid fit method provided a more accurate delineation of lesion extent, while the standard HM-MRI fit missed the smaller component of the lesion in the transition zone on slice 9 (green arrow).Discussion
Standard HM-MRI fit tends to overestimate the volume fraction of the lumen compartment, as evidenced by the larger lumen volumes measured from the long T2 component amplitudes of EGS data (Figure 2). This overestimation likely results from stroma being incorrectly classified as lumen. This is a critical factor since PCa is typified by reduced volume fraction of lumen. Additionally, the sum of epithelium and stroma volume fractions from HM-MRI fits is smaller than the amplitude of the short T2 component from EGS fits. The combination of EGS + Hybrid accounts for the rapidly decaying signal from PCa that is missed by standard Hybrid (and conventional DWI). As a result, EGS+Hybrid increases sensitivity to PCa. The broader TE range of EGS data allows for a more accurate assignment of signals to their respective tissue compartments, with long TE data points serving as reliable estimators of lumen, and short TE points allowing to separate epithelium and stroma signals. This distinction is important for reliably detection of PCa and highlights the role of EGS data in improving the HM-MRI technique. Finally, the results represented in Figure 3 emphasize the role of EGS data in complementing HM-MRI for more accurate PCa predictions.Conclusion
Extended Grid Sampling (EGS) has potential to overcome some of the intrinsic limitations of HM-MRI. It results in more accurate identification of prostate tissue compartments, and accounts for the large component of signal from PCa that is missed by standard hybrid and clinical DWI. By integrating EGS into the HM-MRI analysis, we enhance the precision of prostate cancer (PCa) predictions and the delineation of lesion extent. EGS+Hybrid is likely to improve diagnostic performance when signal-to-noise ratio is low because it increases sensitivity to PCa. This will be very helpful as an increasing number of prostate MRI scans are performed without an endorectal coil (ERC).Acknowledgements
We would like to express our sincere gratitude to the Radiology Department at the University of Chicago for their support and resources that made this research possible.References
1. A. Chatterjee et al. “Diagnosis of Prostate Cancer with Noninvasive Estimation of Prostate Tissue Composition by Using Hybrid Multidimensional MR Imaging: A Feasibility Study”. Radiology (2018).
2. A. Chatterjee et al. “Histological validation of prostate tissue composition measurement using hybrid multi-dimensional MRI: agreement with pathologists’ measures”. Abdominal Radiology 47 (2021), pp. 801–813.
3. G. Lee, A. Chatterjee, I. Karademir, et al. “Comparing Radiologist Performance in Diagnosing Clinically Significant Prostate Cancer with Multiparametric versus Hybrid Multidimensional MRI”. Radiology 305.2 (2022), pp. 399–407.
Figures