3331
The relationship between preoperative PI-RADS version 2.1 and Gleason score change after radical prostatectomy1Department of Radiology, Peking Union Medical College Hospital, Beijing, China, 2Peking Union Medical College Hospital, Beijing, China
Synopsis
Keywords: Prostate, Cancer
Motivation: If reliable preoperative risk factors to predict Gleason score (GS) upgrading after radical prostatectomy (RP) are identified, such could be helpful to reduce the risk of misclassification of PCa patients.
Goal(s): To investigate the relationship between Prostate Imaging Reporting and Data System version 2.1 (PI-RADS v2.1) and GS change after RP.
Approach: Multivariate analyses were performed to analyse the factors influencing GS change after RP.
Results: Multivariate regression analysis showed positive biopsy cores of ≥ 4, biopsy Gleason score of <7 and PI-RADS v2.1 score of 4–5 were independent predictors of GS upgrading after RP (all P < 0.05).
Impact: Combining the number of positive biopsy cores, biopsy Gleason score and PI-RADS v2.1 score could significantly improve the diagnostic efficiency for Gleason score upgrading after radical prostatectomy.
Introduction
Prostate cancer (PCa) is the most common malignant tumour in men living in Europe or the United States1. Multi-parametric MRI (mpMRI) has emerged as a valuable tool for PCa detection and invasiveness evaluation. The Prostate Imaging Reporting and Data System (PI-RADS) was first revealed in 2012 and revised in 2019 (PI-RADS version 2.1 [v2.1]) to ensure standardisation in obtaining and reporting mpMRI data2,3.The treatment strategy of PCa usually depends on the biopsy Gleason score (bGS)4. However, the rates of discordance between bGS and Gleason score after radical prostatectomy (pGS) have been reported to range from 20% to 60% 5. Identification of more reliable preoperative risk factors to predict Gleason score (GS) upgrading and downgrading after radical prostatectomy (RP) would not only reduce the risk of misdiagnosis, but also provide advice to patients about treatment decisions. Therefore, in this study, we investigated the relationship between GS change after RP and preoperative PI-RADS v2.1, and the influencing factors of GS upgrading after RP.Methods
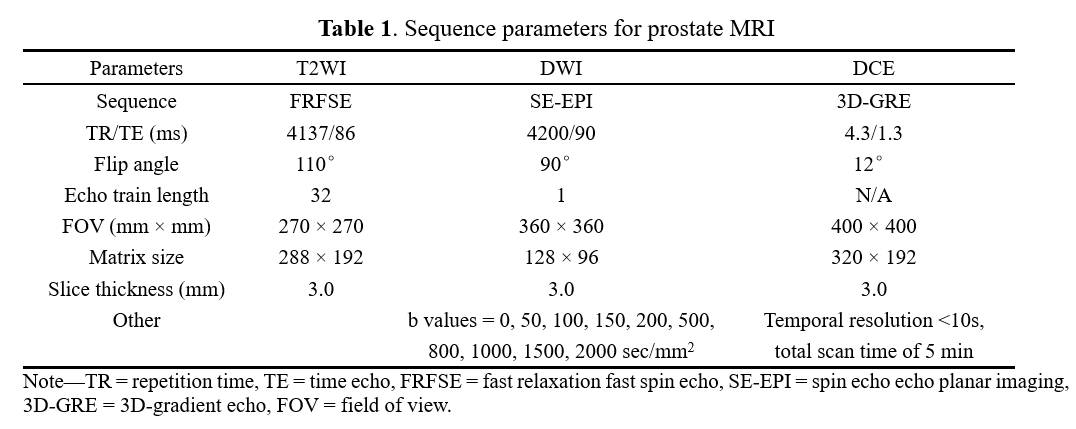
The following patients were included: (1) diagnosis confirmed by systematic transperineal ultrasound-guided prostate biopsy and RP after MRI; (2) performance of a complete MRI examination; (3) performance of a complete laboratory examination, including total PSA (tPSA), free PSA (fPSA) and PSA density (PSAD); and (4) no therapies before prostate biopsy and RP. In total, 225 patients were enrolled between January 2015 and December 2021. Clinicopathologic factors were derived from patient medical records. Patients who were biopsied all underwent a 11 + X-core systematic transperineal ultrasound-guided prostate biopsy performed by a single urinary specialist. The radiologist matched the lesions with the highest PI-RADS v2.1 scores on the MRI images with the biopsy and prostatectomy pathology report. MRI scanning was performed using a GE750 3.0T scanner (GE Healthcare, Milwaukee, WI, USA). The scan sequence included axial T1WI and T2WI, coronal and sagittal T2WI, DWI and DCE. We used ADC graph for evaluation when the b-value was 100 and 1000 sec/mm2. The MRI image-acquisition parameters are shown in Table 1. The chi-squared test was used to compare differences among PCa location, bGS and PI-RADS v2.1 score. The factors influencing GS upgrading after RP were analysed by logistic regression. The area under curve (AUC) for prediction of GS upgrading was estimated by receiver operating characteristic curve (ROC) . P < 0.05 was considered statistically significant.Results
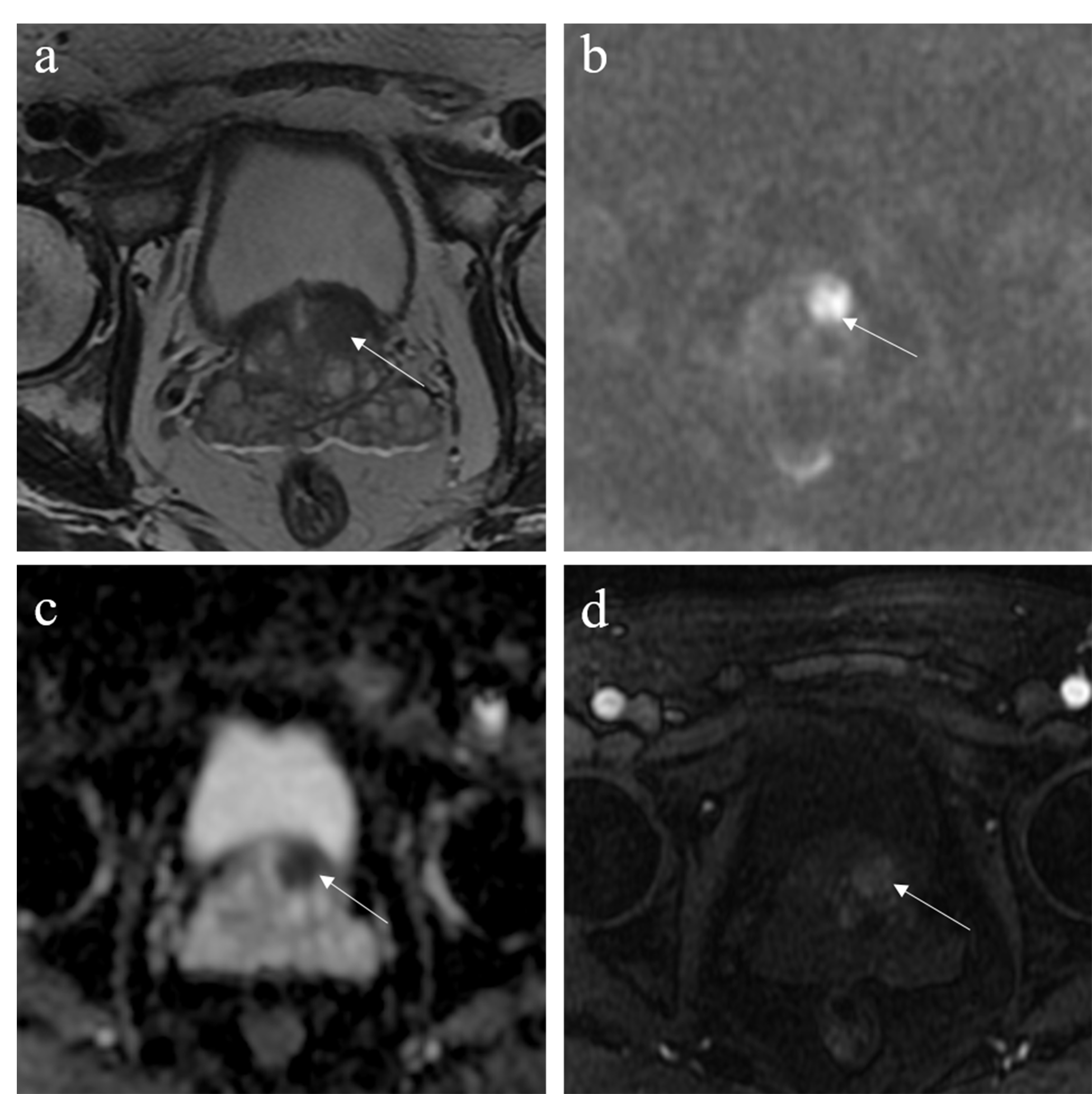
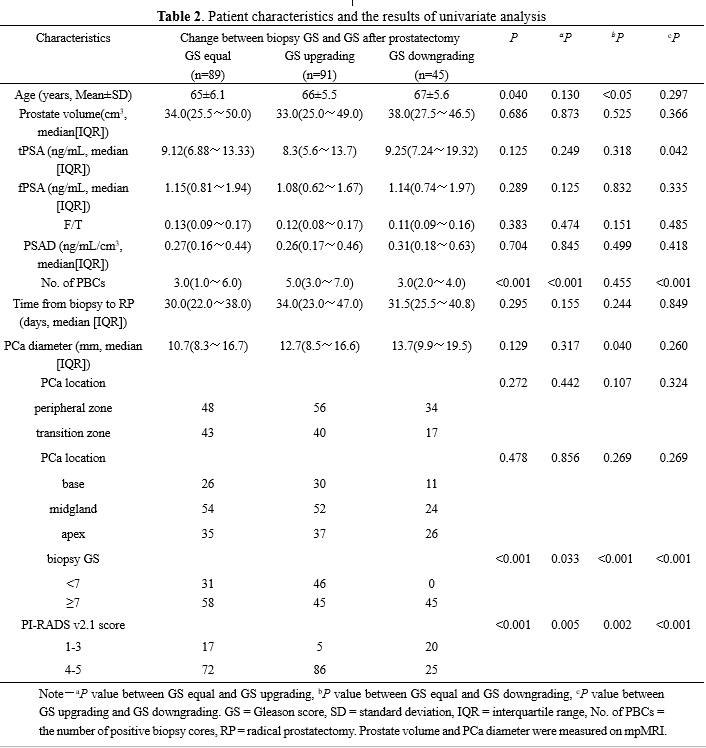
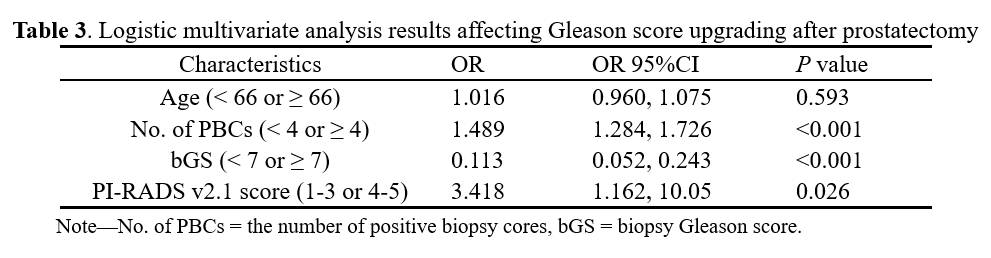
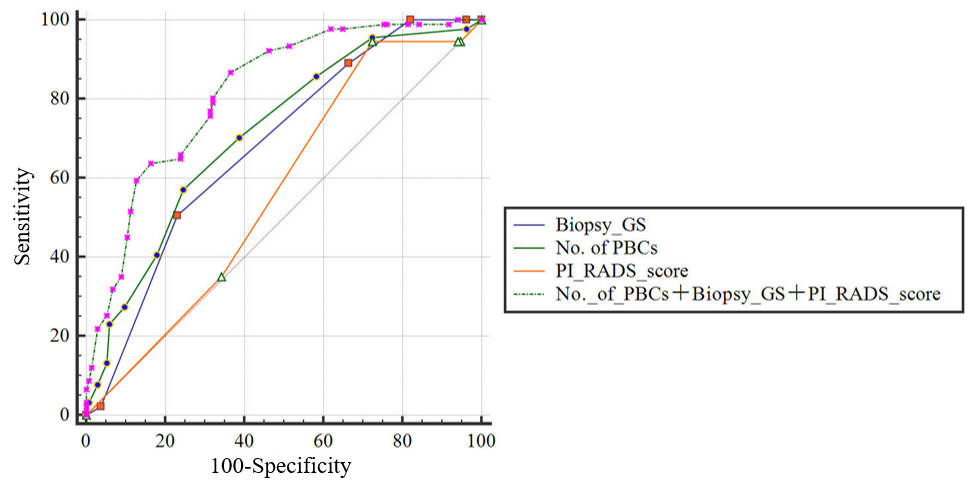
Figure 1 shows a 68-year-old man with pathological upgrading of GS from 6 at biopsy to 7 (4 + 3) after RP. Univariate analysis showed that age, positive biopsy cores (No. of PBCs), bGS and PI-RADS v2.1 score were factors driving postoperative GS changes (all P < 0.05), which was shown in Table 2. Further, multivariate logistic regression analysis showed that No. of PBCs, bGS and PI-RADS v2.1 score were independent predictors of GS upgrading after RP (all P < 0.05), which was shown in Table 3. The AUCs of No. of PBCs, bGS and PI-RADS v2.1 score were 0.713, 0.637 and 0.611, respectively (Fig. 2). The AUC of the combined diagnosis model was 0.817, which was larger than those of the three aforementioned variables alone (all P < 0.001).Discussion
The PI-RADS scoring system integrated T2WI, DWI and DCE-MRI scan information to perform quantitative grading according to their imaging manifestations. In this study, we found that patients with PI-RADS v2.1 score of ≥4 were more likely to have GS upgrading after RP. Meanwhile, the risk of GS upgrading after RP was 3.4 times higher in the high PI-RADS score group (4–5 points) than in the low PI-RADS score group (1–3 points). That could explain which patients in the high-grade PI-RADS v2.1 group (4–5 points) had lower bGS values than pGS values in our study. Patients harbouring high-risk PCa are at great risk for adverse pathologic outcomes, and causes high rates of metastatic diseas. Therefore, accurate prediction of bGS upgrading has always been important. The predictive performances of No. of PBCs, bGS and PI-RADS v2.1 score for GS upgrading after RP were moderate, with AUCs of <0.72 across all three cohorts. By integrating three independent predictors, the diagnostic efficiency of the combined model for GS upgrading after RP was significantly improved, with an AUC of 0.817.Conclusions
GS is more likely to be upgraded after prostatectomy for PCa patients with ≥ 4 PBCs, bGS of <7, and PI-RADS v2.1 score of 4–5. Combining three independent predictors could significantly improve the diagnostic efficiency for GS upgrading after RP, which could minimise the possibility of PCa undertreatment.Acknowledgements
We sincerely thank the participants in this study.References
1. Siegel R L, Miller K D, Wagle N S, et al. Cancer statistics, 2023. CA Cancer J Clin. 2023;73:17-48.
2. O'Shea A, Harisinghani M. PI-RADS: multiparametric MRI in prostate cancer. MAGMA. 2022;35:523-532.
3. Gupta R T, Mehta K A, Turkbey B, et al. PI-RADS: Past, present, and future. J Magn Reson Imaging. 2020;52:33-53.
4. Mottet N, van den Bergh RCN, Briers E, et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur Urol. 2021;79:243-262.
5. Song W, Bang S H, Jeon H G, et al. Role of PI-RADS Version 2 for Prediction of Upgrading in Biopsy-Proven Prostate Cancer With Gleason Score 6. Clin Genitourin Cancer. 2018;16:281-287.
Figures