3330
Implementation of mpMRI Habitat Risk Scoring System in Prostate Cancer Biopsy Acquisition Improves the Yield of Significant Cancer.1Radiation Oncology, Sylvester Comprehensive Cancer Center, Miami, FL, United States, 2Desai Seth Urology Institute, Miami, FL, United States
Synopsis
Keywords: Prostate, Data Analysis, Biopsy Targeting, Lesion Identification, Risk Categorization
Motivation: The accurate localization and assessment of aggressiveness in patients with prostate cancer is key to appropriate treatment, especially radiation therapy (RT) planning.
Goal(s): To evaluate the performance of a Habitat Risk Scoring (HRS) system in MRI/Ultrasound-fused biopsy of prostate cancer at the time of the fiducial marker placement prior to RT.
Approach: The yield of significant prostate cancer biopsy findings under HRS guidance was compared with alternative standard techniques.
Results: Patients from the Miami BLaStM trial were analyzed with and without HRS guidance. The biopsies obtained through HRS guidance yielded more clinically significant cancer.
Impact: The implementation of the Habitat Risk Scoring (HRS) system in transperineal platform for MRI-US biopsies significantly improved the delineation of aggressive cancer. These volumes are integral to the safe delivery of focal escalated radiation doses.
Purpose
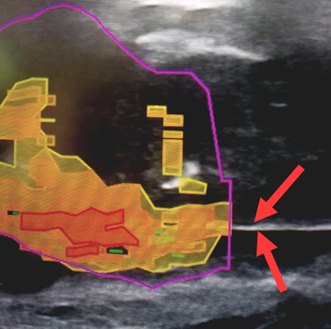
The accurate localization and assessment of aggressiveness in patients with prostate cancer is key to radiation therapy (RT) planning. During the fiducial marker placement, a limited number of biopsy cores were obtained. We have implemented the Habitat Risk Score (HRS) in transperineal platform for MRI/Ultrasound-fused (MRI-US) biopsies. HRS is a per-pixel quantitative mpMRI analysis technique that combines perfusion (Dynamic Contrast Enhanced (DCE)) and diffusion mpMRI sequences to identify distinct pathophysiologic regions, or “habitats” as heat maps on imaging1. The aim of this study is to evaluate the utility of the HRS for accurately sampling aggressive cancer when used as a guidance in MRI-US fusion biopsy procedures for prostate cancer.Methods
The Miami BLaStM trial (NCT02307058; PI: Pollack) is a Phase II randomized study that compares two methods for increasing dose to the mpMRI-defined imaging tumor volume(s). Patients diagnosed with prostate cancer are enrolled in the trial and undergo fiducial marker placement with a concurrent biopsy to verify location and volume of the cancer. This is performed on one of two MRI-US fusion biopsy platforms: (i) transrectally using the Phillips UroNav platform with external tracking; or (ii) transperineally using the bkMedical bkFusion platform with stepper tracking. We have implemented the HRS in the bkMedical bkFusion platform which is interfaced with MIM (MIM Software Inc., Cleveland, USA) as demonstrated in Figure 1. We hypothesize that HRS guidance will increase the precision of fusion biopsy while simultaneously reducing the overall amount of biopsy cores taken from each patient.Results
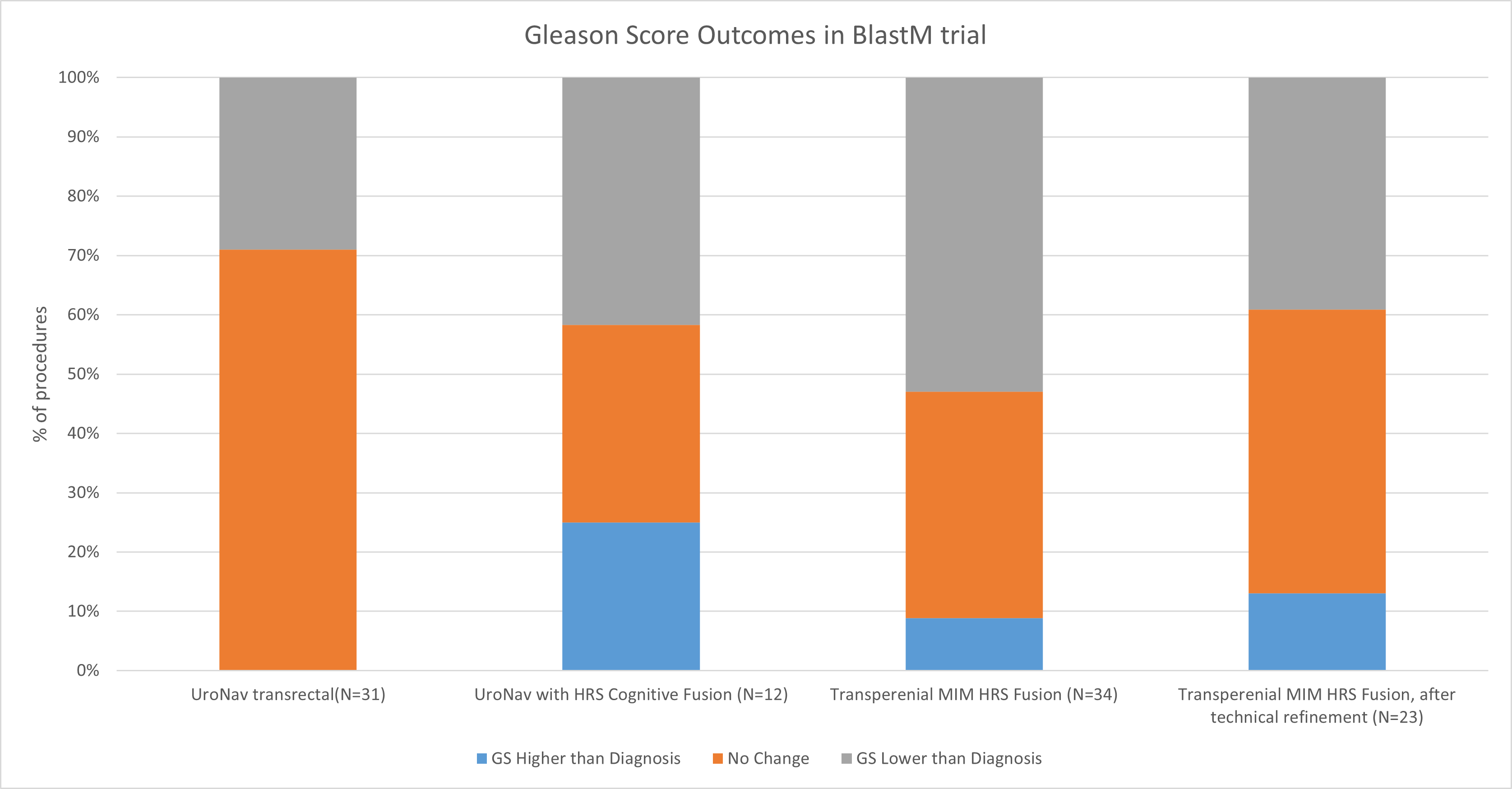
A total of 77 BLaStM patients were analyzed: bkFusion (n=34) and UroNav control group (n=43). For 12 UroNav patients, the HRS maps were generated and discussed with the physician conducting the biopsy. We will refer to this cohort as the “UroNav transrectal procedure with “cognitive” HRS-guidance”.The resulting biopsy Gleason scores (GS) were compared to the original diagnostic biopsy per-session and per-lesion. On a per-session basis, the highest GS obtained from the HRS-guided biopsy was compared to the GS from the diagnostic biopsy. The results were classified into 3 categories: Fusion biopsy GS higher than diagnostic GS, no GS change from diagnostic, and fusion biopsy GS lower than diagnostic GS. On the per-core basis, the number of cores taken from each procedure were compared against the number of cores with histopathologic indication for cancer (GS6 or higher). For each fusion biopsy technique, the percentage of total positive cores was compared to the control group. Four methods were assessed:
· the control UroNav transrectal procedure
· the UroNav transrectal procedure with “cognitive” HRS-guidance
· the transperineal bkFusion HRS-guided fusion biopsy
· the bkFusion HRS-guided fusion biopsy after a technical refinement period (corresponding to application of the method to the first 20 patients).
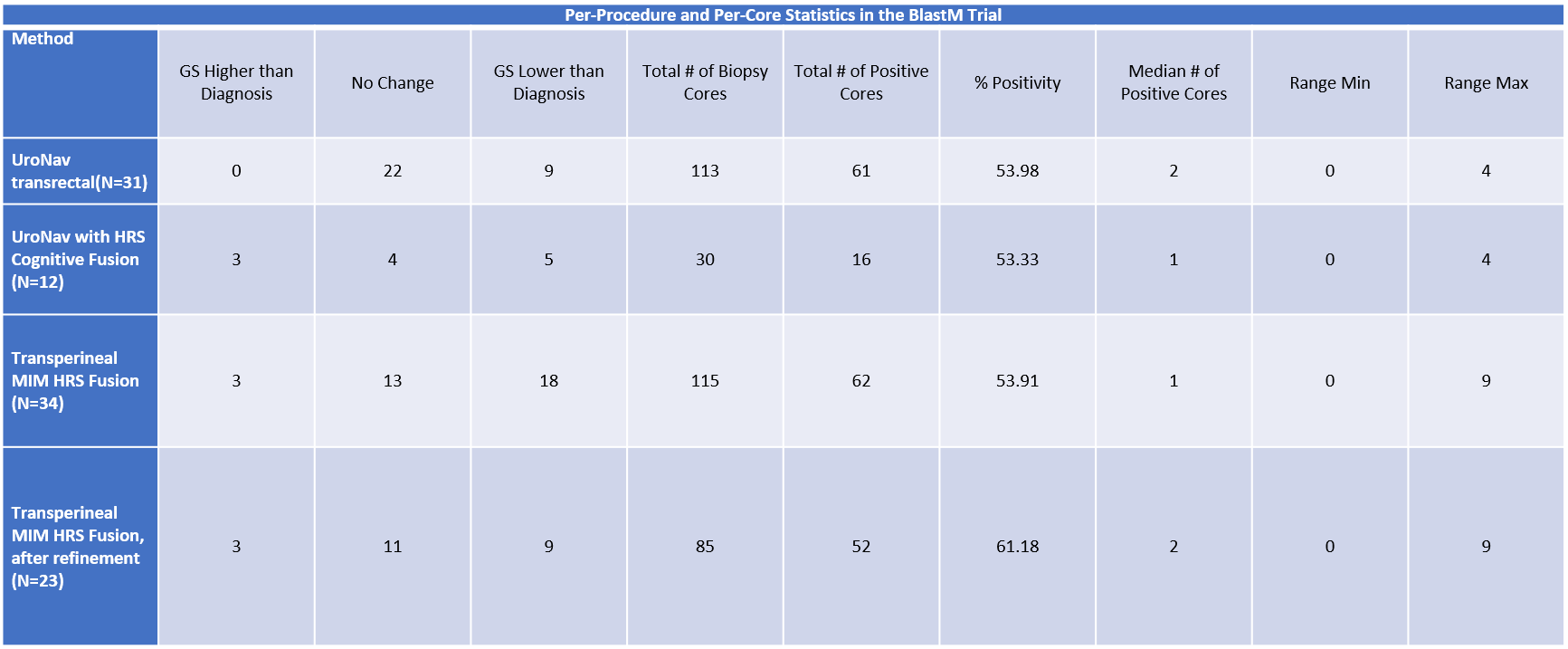
The per-session results are shown in Figure 2 and the per-session and per-core statistics are shown in Table 1. The control result without/with HRS cognitive fusion yielded a 53.98%/53.33% positivity rate from biopsy cores taken, and a result of and 9/5 sessions with highest GS lower than diagnosis. and 0/3 sessions with GS higher than peak diagnostic GS. The transperineal method before/after the learning period yielded a 53.91%/61.18% positivity rate, and a result of 3/3 sessions with GS higher than diagnostic, and 18/9 GS lower than diagnosis. In all experimental cases, the use of HRS resulted in detection of higher GS than in diagnostic biopsy, increasing sensitivity of biopsy. After technical refinement, HRS-guidance enabled less cores to be taken per-session to confirm the diagnostic result yielding an overall higher positivity rate.
Discussion
The technical refinement period in the bkFusion platform included adaptation of the HRS workflow to the ultrasound unit, familiarization with the stepper unit, and familiarization with the transperineal procedure in-clinic. The % positivity of the transperineal biopsies without technical refinement were within 0.1% of the control method establishing that both methods have a similar baseline of accuracy even accounting for non-positive biopsy cores. While there was higher incidence of lower GS biopsied than diagnosis in the transperineal cohort, this is directly related to the adoption of a new technology and methodology in clinic.With the technical refinement period applied, the MRI-ultrasound fusion in the bkFusion platform resulted in a much larger yield of positive cores than other methods.
Acknowledgements
The research was supported by the National Cancer Institute of the National Institutes of Health under Award Number P30CA240139, RO1CA189295, R01CA190105, and U01CA239141.
References
1. Stoyanova R, Chinea F, Kwon D, et al. An Automated Multiparametric MRI Quantitative Imaging Prostate Habitat Risk Scoring System for Defining External Beam Radiation Therapy Boost Volumes. Int J Radiat Oncol Biol Phys. 2018;102: 821-829.
Figures