3299
fMRI in Patients with Implanted Electrodes: Understanding and Mitigating Imaging Artifacts1Biomedical Engineering, University of Calgary, Calgary, AB, Canada, 2Radiology, University of Calgary, Calgary, AB, Canada
Synopsis
Keywords: fMRI Analysis, Epilepsy, Implanted Electrodes, intracranial EEG, fMRI, Susceptibility
Motivation: Model susceptibility-induced signal degradation in fMRI in patients with implanted electrodes and reduce imaging artifacts across electrodes.
Goal(s): Develop a model to understand and mitigate susceptibility effects due to implanted electrodes in fMRI.
Approach: Model electrode (platinum sphere) and brain activation contrast (cylinders representing blood vessels) at 3T. Calculate intravoxel dephasing and assess the impact of the electrode on signal amplitude and activation contrast. Investigate the impact of echo times on signal loss.
Results: Key findings reveal signal enhancement with increased distance from the electrode and reduced contrast loss with shorter echo times.
Impact: This research could redefine future functional diagnostics in patients with implanted electrodes such as epilepsy or Parkinson’s disease patients, leading to more precise surgical interventions and improved patient care. Mitigating susceptibility-induced image artifacts will impact neuroscience research and clinical applications.
INTRODUCTION
Many patients with neurological disorders such as epilepsy or Parkinson’s disease may benefit from implanted intracerebral electrodes for brain activity monitoring or brain stimulation. In these patients, functional MRI (fMRI) can provide valuable insights into brain activity. However, this presents challenges, primarily associated with image degradation due to susceptibility artifacts introduced by the electrodes1,2. The objective of this study is to generate a biophysical model of these artifacts and to quantify the potential for artifact mitigation by multi-echo imaging approaches3.METHODS
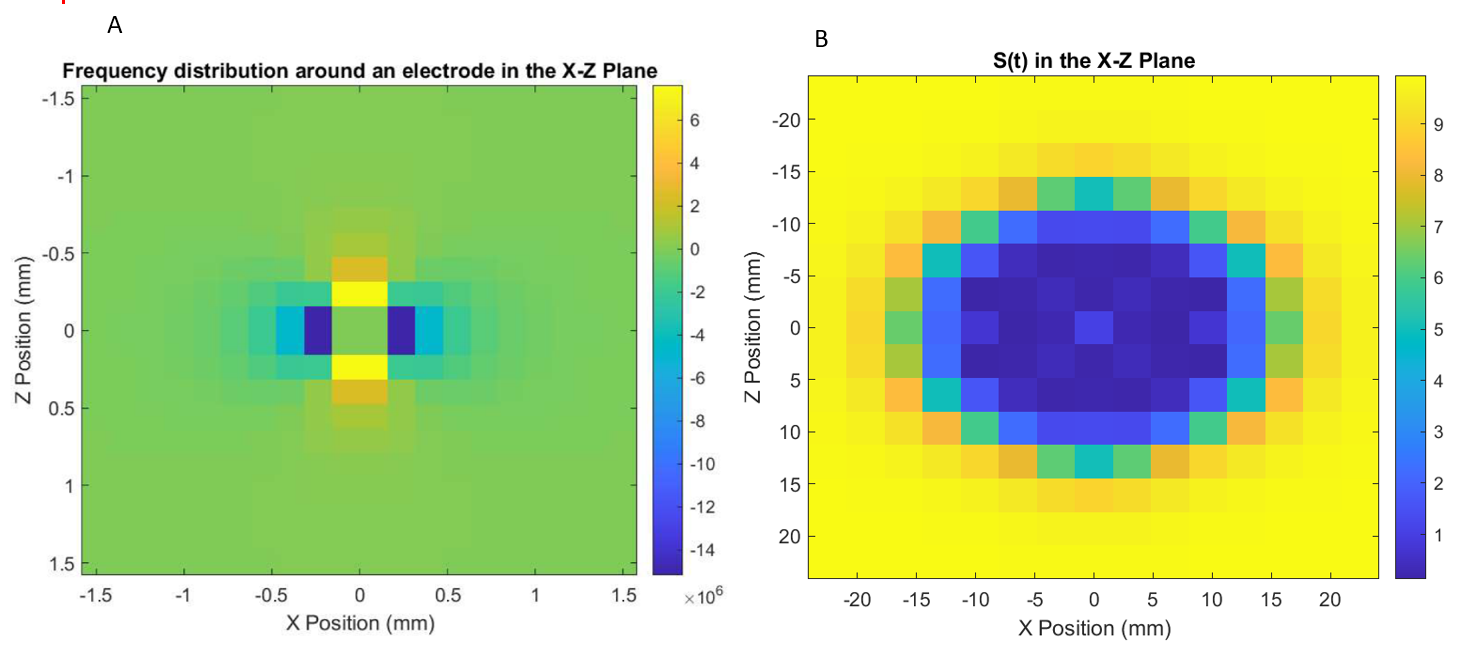
We have established a physical model that accounts for the susceptibility effects introduced by an implanted electrode and blood vessels during brain activation at 3T. To model the susceptibility artifacts in fMRI, we represented the electrodes as platinum spheres with diameter 0.56mm (matching clinical Ad-Tech electrodes), with a magnetic susceptibility of 2.65x10-4. The blood vessels were modeled as randomly distributed cylinders, each with a susceptibility of -6.93x10-6. T2* values at rest and during brain activation were calculated using the following parameters: oxygenation fraction during resting brain state (0.6), oxygenation fraction during active brain state (0.7), susceptibility difference between oxygenated and deoxygenated blood (0.8x10-7), volume fraction during the resting brain state (0.05) and the volume fraction during the active brain state (0.06) for a 5ml blood volume per 100ml brain volume. To assess signal degradation, we quantified intravoxel dephasing by subdividing 3x3x3mm3 voxels (typical for fMRI) into 10 sub voxels along each spatial dimension. For each sub voxel, we calculated the local magnetic field from the model described above. The corresponding local Larmor frequency information (fig 1.A) was then used to derive the MRI signal within each voxel (fig 1.B).RESULTS
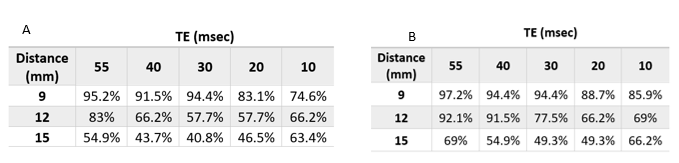
In the presence of the electrode, the main observable effect is a large loss in signal. At a distance of 3, 4, and 5 voxels (9, 12, and 15 mm respectively) away from the electrode, the signal loss was 95.1%, 81.3%, and 53.7%, respectively. This suggests that useful fMRI signal may only be measured at least 15mm away from the electrode. However, in the fMRI context, it is the contrast between rest and activation that is relevant, rather than the absolute signal magnitude. We thus calculated this loss in contrast and found it to be similarly large (95.2%, 83%, and 54.9% at locations 3, 4, and 5 voxels away from the electrode in a direction parallel to Bo, respectively, and 97.2%, 92.1%, and 69% in a direction perpendicular to Bo). Nevertheless, this loss in signal contrast may be partially recoverable by optimizing the echo time. Figure 2 shows the calculated loss in BOLD activation contrast at echo times of 55, 40, 30, 20, and 10 milliseconds. We can see that despite the previously reported large signal loss close to the electrodes, there may still be sufficient BOLD contrast to quantify fMRI activations. For example, at a location 3 voxels away from the electrode along B0, where signal loss is 95%, the corresponding BOLD contrast loss is only ~75% when using a TE of 10 ms. The optimal TE is spatially variable and depends on the distance between a voxel and the electrode.CONCLUSION
Our research endeavors to address a critical issue when using fMRI in patients with implanted electrodes. The modeled signal loss is consistent with previously reported values that were measured experimentally at 3T1. However, in fMRI, the strength of the MRI signal is less relevant than the amplitude of the MRI signal change during brain activation. We have determined that despite the significant loss of MRI signal in the vicinity of the electrode, the loss in MRI contrast was less pronounced and could be partially recovered by optimizing TE. As the optimal TE was spatially variable, this presents an opportunity for the implementation of multi-echo fMRI approaches in the future, which will provide optimal signal contrast at every brain location. This avenue holds promise for enhancing our understanding of susceptibility-induced effects and improving the sensitivity of fMRI in patients with implanted electrodes.Acknowledgements
This work was supported by NSERC Discovery Grant RGPIN-2021-02797 and CIHR grant PJT-183825.References
1. Boucousis, S. M., Beers, C. A., Cunningham, C. J., Gaxiola-Valdez, I., Pittman, D. J., Goodyear, B. G., & Federico, P. Feasibility of an intracranial EEG-fMRI protocol at 3T: risk assessment and image quality. NeuroImage, 2012; 63(3), 1237–1248.
2. Alexandre Boutet, Tanweer Rashid, Ileana Hancu, Gavin J. B. Elias, Robert M. Gramer, Jürgen Germann, Marisa Dimarzio, Bryan Li, Vijayashankar Paramanandam, Sreeram Prasad, Manish Ranjan, Ailish Coblentz, Dave Gwun, Clement T. Chow, Ricardo Maciel, Derrick Soh, Eric Fiveland, Mojgan Hodaie, Suneil K. Kalia, Alfonso Fasano, Walter Kucharczyk, Julie Pilitsis, and Andres M. Lozano, Functional MRI Safety and Artifacts during Deep Brain Stimulation: Experience in 102 Patients. Radiology 2019 293:1, 174-183
3. Posse, S., Wiese, S., Gembris, D., Mathiak, K., Kessler, C., Grosse-Ruyken, M. L., Elghahwagi, B., Richards, T., Dager, S. R., & Kiselev, V. G: Enhancement of BOLD-contrast sensitivity by single-shot multi-echo functional MR imaging. Magnetic resonance in medicine, 1999;42(1), 87–97.
Figures