3292
Fast and Motion-Robust Non-Contrast MR Angiography using Centric ky–kz Trajectory.1Radiology, UC San Diego, La Jolla, CA, United States, 2VA San Diego Healthcare System, San Diego, CA, United States, 3Canon Medical, Ōtawara-shi, Japan, 4Radiology, Kyoritsu Tobata Hospital, Fukuoka, Japan
Synopsis
Keywords: New Trajectories & Spatial Encoding Methods, Blood vessels, FBI, Non-contrast
Motivation: The purpose of this study is to develop a fast, motion-robust fresh blood imaging (FBI) technique using a centric ky–kz k-space trajectory (cFBI) and an exponential refocusing flip angle (eFA) scheme.
Goal(s): Investigate scan time reduction and image quality of cFBI and compare it with the standard FBI technique.
Approach: Advancement of the cFBI sequences with eFA and optimized cardiac trigger delays on a 3-T MR imager, aiming to reduce the scan time and maintaining the image quality.
Results: cFBI outperforms standard FBI in scan time reduction with good image quality with less motion-related artifacts and Nyquist N/2 artifacts.
Impact: A two-fold reduction in scan time is achieved with the non-contrast FBI technique, while still maintaining image quality and reducing motion and N/2 artifacts.
Introduction
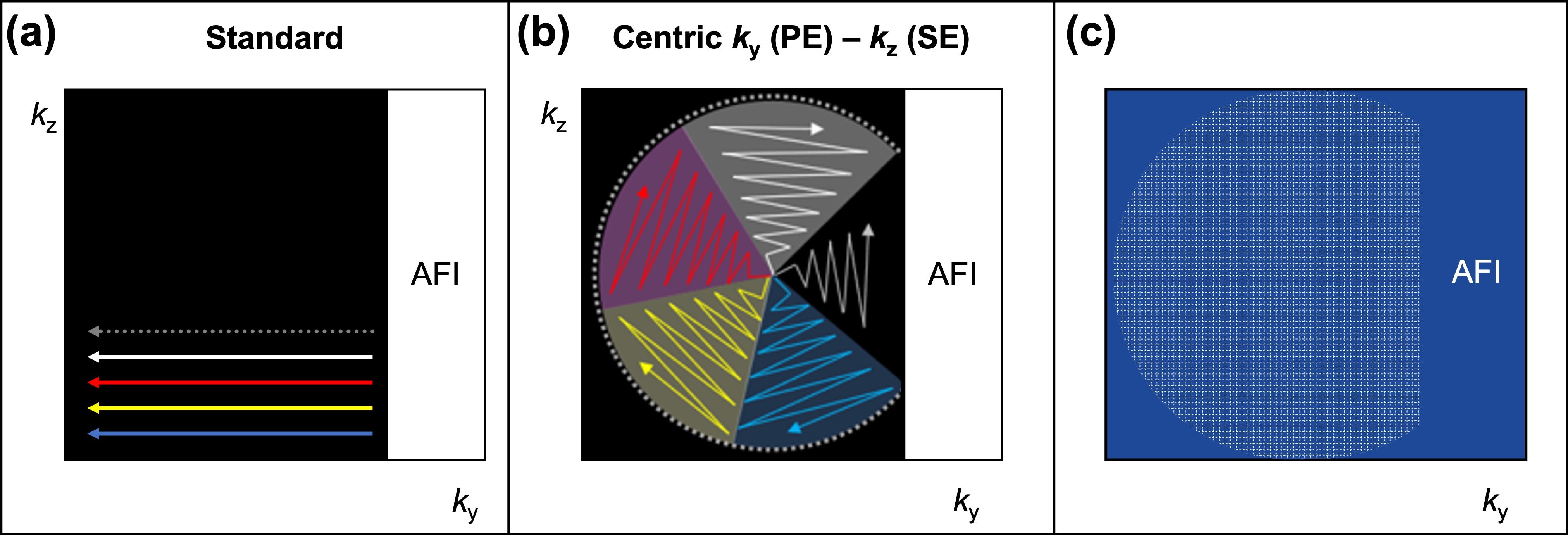
Fresh blood imaging (FBI), non-contrast MR angiography, relies on physiological blood signal difference between systole and diastole and requires both systolic and diastolic acquisitions [1-5]. Thus, standard FBI (sFBI) has intrinsic drawbacks of motion artifacts, owing to long acquisition time for two systolic and diastolic acquisitions and often seen Nyquist N/2 artifacts in the phase encoding (PE) direction due to inappropriate readout (RO) dephasing spoiler pulses.Methods
The study was approved by the Institutional Review Board. All MR imaging data were obtained with a clinical 3T MR imager (Vantage Galan 3T, Canon Medical Systems, Japan) in 8 healthy subjects without peripheral artery disease (PAD) or cardiovascular disease (CAD) (4 males and 4 females; mean age 46.6 ± 22.6 years; range, 24 – 65 years). Before the experiments, various eFA schemes were studied in two healthy subjects. All 8 subjects were involved in the optimization of trigger delays for systole and diastole for cFBI due to a longer acquisition window. After optimization, the 8 subjects and 2 patients with PAD or CAD were enrolled to compare sFBI with cFBI. Figure 1 shows the k-space filling of standard and centric ky–kz acquisitions.Results
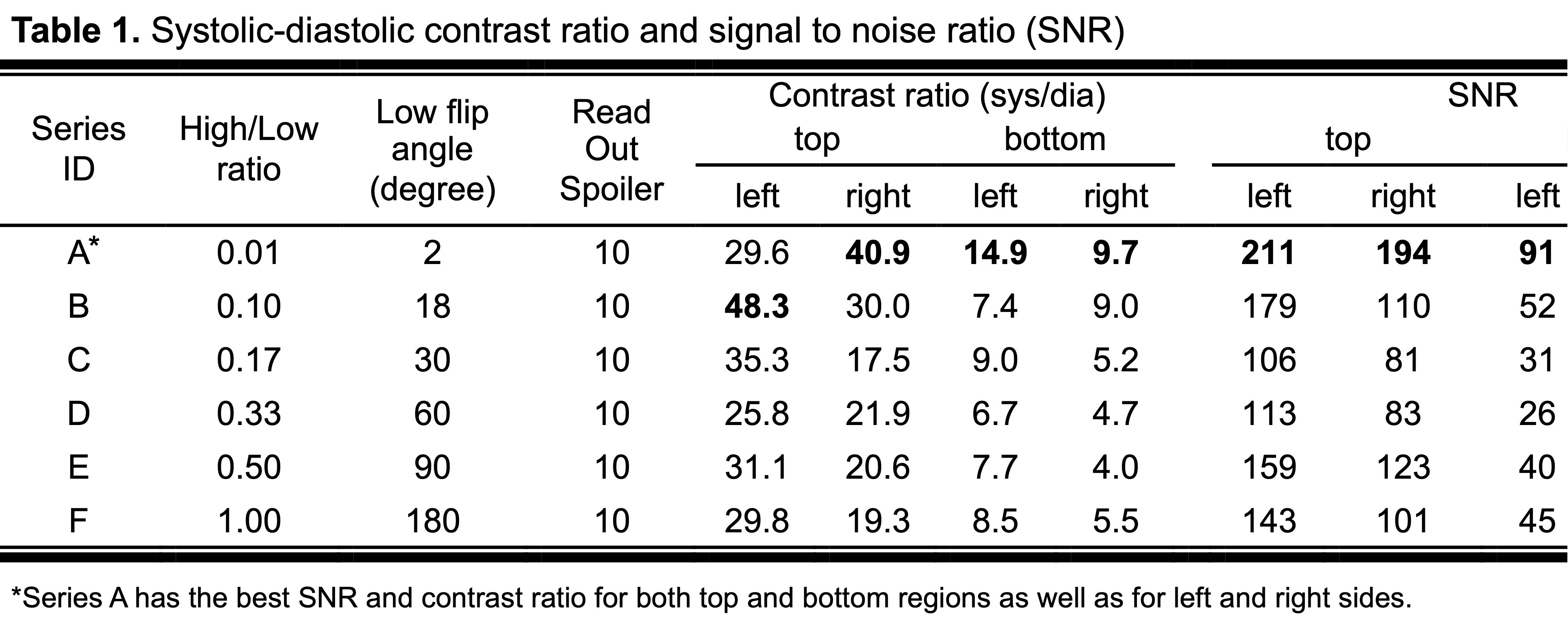
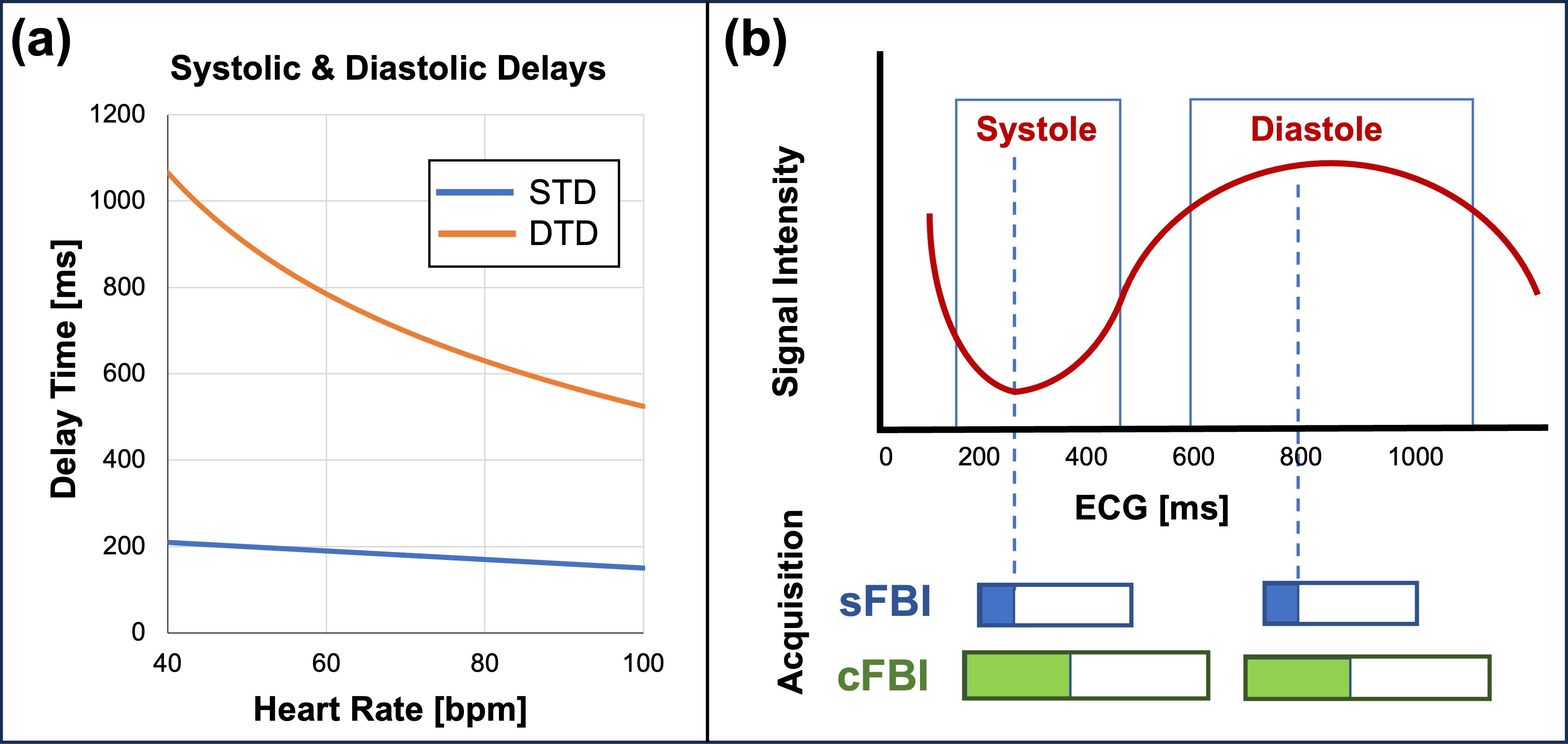
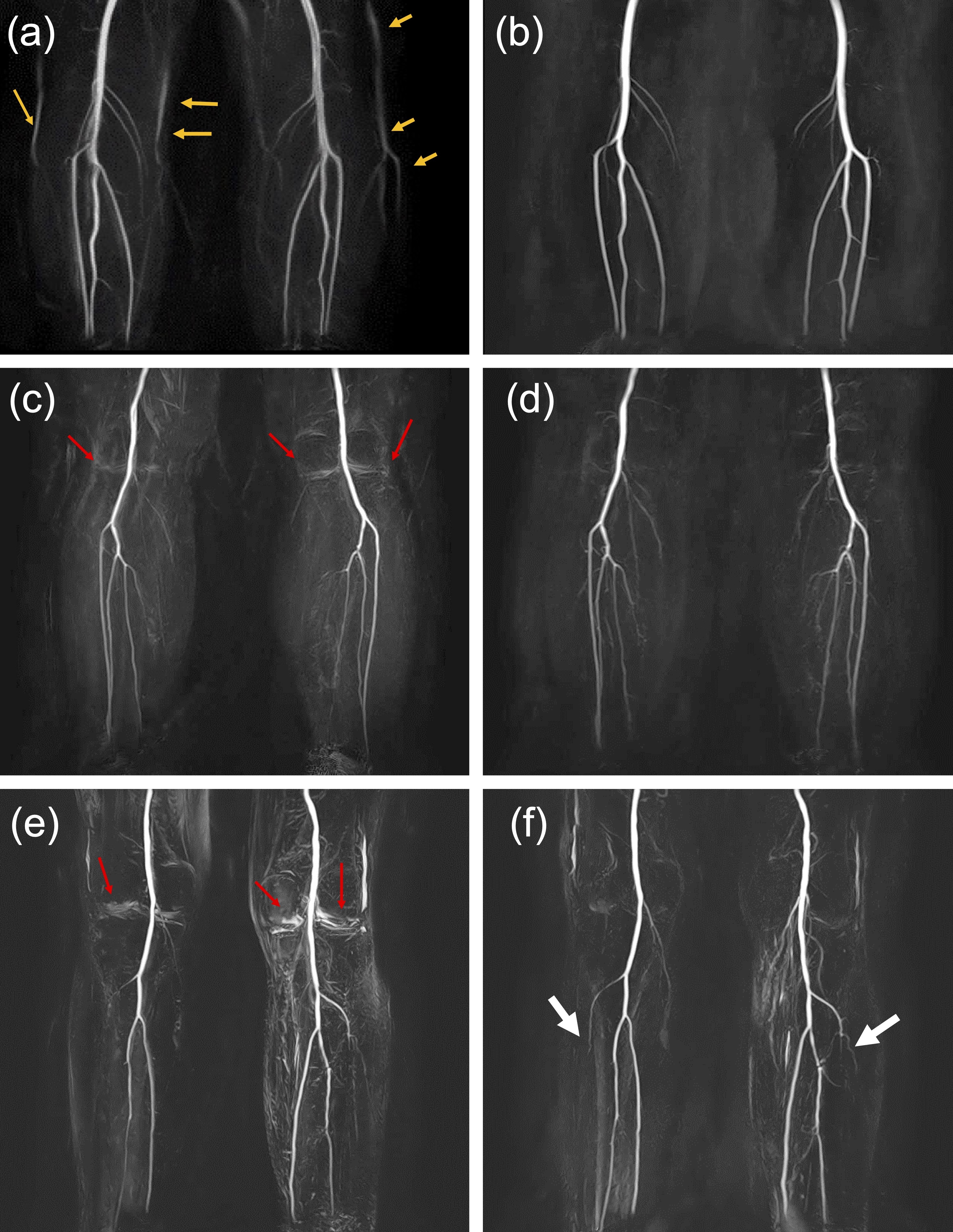
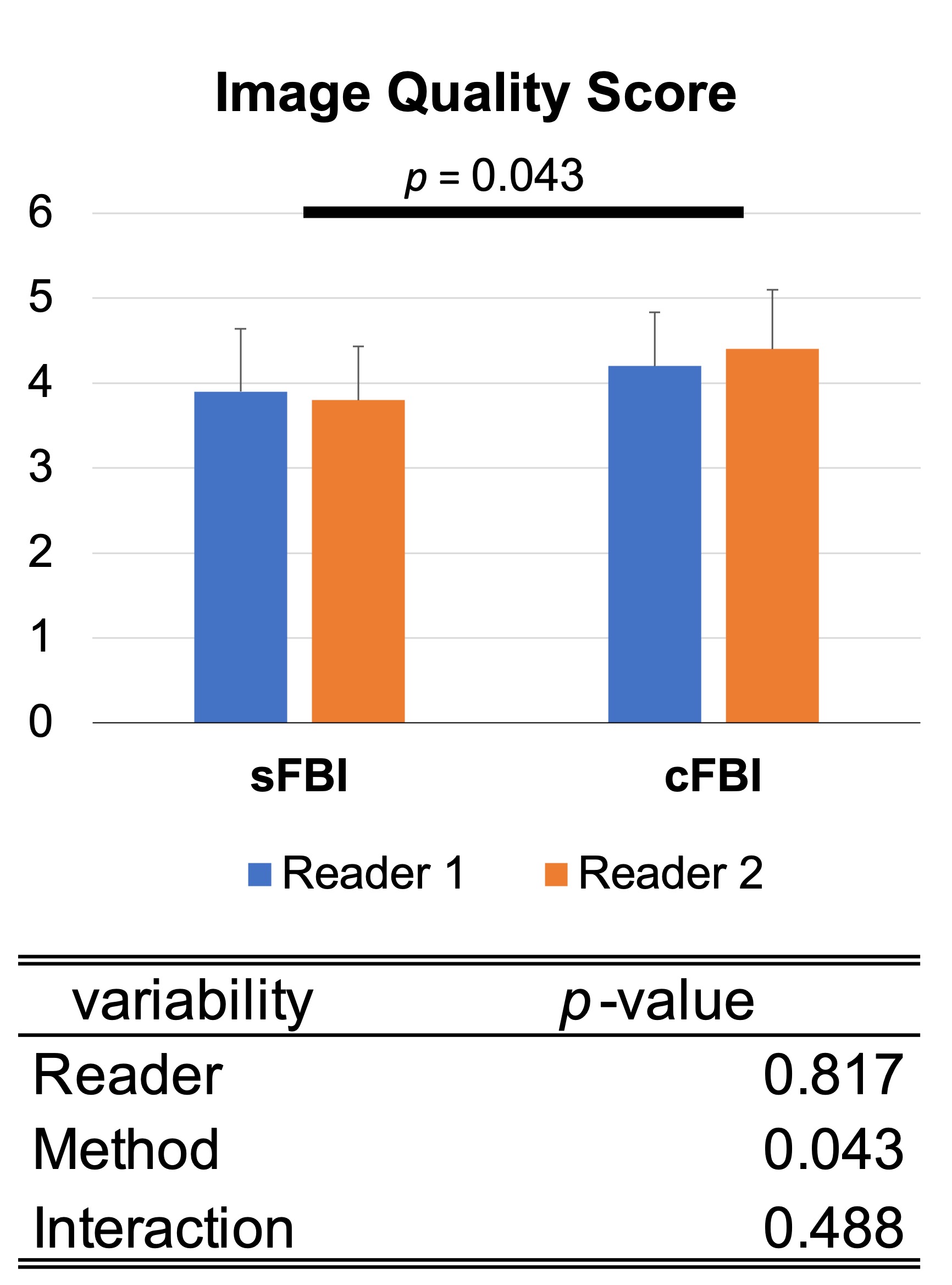
cFBI with eFA achieved a nearly 50% reduction in scan time compared to sFBI. Table 1 presents the eFA with a high/low refocusing flip angle scheme. A high/low flip angle of 180/2 degrees exhibits less saturation effect and yields the highest blood signals, but it is sensitive to background signals. Simulation results of eFA indicated that the saturation effect decreases with lower high/low flip angles. Overall, images with 180/30 degrees show reasonable blood signal recovery while minimizing background signal artifacts. Optimization of systolic and diastolic triggering delays (STD and DTD), calculated from the heart rate, indicated trigger delays of -30 to -50 ms relative to those in sFBI due to cFBI's longer acquisition window with a zigzag ky–kz acquisition (Figure 2). After optimizing the trigger delays in cFBI, the maximum intensity projection (MIP) images after systole-diastole subtraction demonstrate fewer motion artifacts and N/2 artifacts compared to sFBI, as depicted in Figure 3. The sFBI images on the left exhibit N/2 and motion artifacts, whereas the images on the right with cFBI have minimized those artifacts. The reduced motion artifacts in cFBI may be attributed to both the ky–kz k-space trajectory and the shorter acquisition time. Furthermore, the cFBI MIP image in Figure 3f shows clearer visualization of bilateral occlusions of the anterior tibial arteries than the sFBI MIP image in Figure 3e. Image quality evaluation of eight subjects and two patients indicates that the image quality of cFBI is compatible with that of sFBI, as shown in Figure 4, while still achieving a two-fold reduction in scan time.Discussion
We have developed fast, non-contrast cFBI MRA that achieves a two-fold reduction in scan time without significant artifacts. This longer acquisition window is required to fit within systole and diastole periods. Thus, we have optimized trigger delays for cFBI using heart rate and compared with the those of sFBI. In FBI, the correct trigger delays of systolic and diastolic periods determined the outcome contrast after subtraction and MIP process. This eliminates the need for preparation scans to set the triggering delays, leading to a shorter overall examination time with fewer N/2 and motion artifacts.Conclusion
We have developed fast non-contrast cFBI MRA using diastolic-systolic subtraction imaging with a two-fold reduction in scan time without major artifacts. Furthermore, we have optimized the trigger delays for cFBI eliminating the need for preparatory scans and consequently allowing for a shorter overall examination time.Acknowledgements
This work was supported by an NIH grant R01HL154092 (M.M.) and a grant by Canon Medical Systems, Japan (35938).References
[1] Miyazaki M., et al., J. Magn Reson Imaging, 12:776-783. (2000)
[2] Miyazaki M., et al., Radiology, 227:890-896. (2003)
[3] Nakamura K., et al., Magn Reson Med., 65:595-602. (2011)
[4] Miyazaki M., et al., Radiology, 248:20-43. (2008)
[5] Miyazaki M., et al., J. Magn Reson Imaging, 35:1-19. (2012)
Figures