3262
Echo time optimization of 2HG-edited MRS and T2 determination of tumor metabolites at 3T1The University of Texas Southwestern, Dallas, TX, United States, 2Biomedical Engineering, University of Texas Dallas, Dallas, TX, United States, 3Department of Internal Medicine, The University of Texas Southwestern, Dallas, TX, United States, 4Department of Neurology, University of Texas Southwestern Medical Center, Dallas, TX, United States, 5Department of Neurological Surgery, The University of Texas Southwestern, Dallas, TX, United States, 6Max Planck Institute for Biological Cybernetics, Tübingen, Germany
Synopsis
Keywords: Pulse Sequence Design, Cancer, MRS, editing, 2HG, brain, tumor
Motivation: 2HG is an important oncometabolite which is commonly detected using J-difference editing.
Goal(s): Here, we determined the optimal echo time for J-difference editing of 2HG at 3T.
Approach: This was done by evaluating the echo time dependence of the 2HG-edited signal using simulations and in vivo experiments. We also quantified the T2 relaxation of 2HG as well as the co-edited glutamate and glutamine signals
Results: A TE of 90 ms was found to produce the highest signal, however, a TE of 70 ms was found to provide the best separation between 2HG and Glx in poor shimming conditions.
Impact: This optimized J-difference edited sequence could improve MRS measurements of 2HG. This would take MRS one step closer towards clinical applicability which could aid in the diagnosis and treatment monitoring of glioma patients.
Purpose
2-hydroxyglutarate (2HG) is a MRS-detectable oncometabolite with important implications for diagnostic and prognostic purposes. Due to the overlap between 2HG and other metabolites such as creatine and phosphocreatine, 2HG is commonly detected using J-difference editing to remove overlying signals from stronger signals and selectively detect 2HG. The choice of echo time (TE) for optimal detection of J-difference edited metabolites is important1, however, no study has performed such an investigation for 2HG. Thus, 2HG-edited studies to date have been acquired with a variety of TEs including 68 ms2,3 and 75 ms4. In theory, the 4.02 ppm should be optimally detected at TE of ~1/2J, (where J is the scalar coupling constant) or ~75 ms4. Strong coupling makes this estimation uncertain, however. Additional signal weightings from T2 relaxation, which biases the signal curves towards shorter TEs, also needs to be taken into consideration when determining the optimal TE. This value, however, is unknown for 2HG.As such, the goal of this study was to investigate the TE dependence of the 2HG-edited signal at 3T using both simulations and in vivo data acquired at multiple TEs. We also quantified the T2 relaxation time of 2HG as well as co-edited glutamate (Glu) and glutamine (Gln).
Methods
2HG-edited data were acquired in 4 low-grade glioma patients (3 female, 1 male age 44.5±6.1 years) with suspected IDH mutations on a Philips Achieva 3T with a 32-channel receive head coil. MRS parameters included a TR=2s, edit-ON/edit-OFF=1.9/7.5 ppm, 15-ms editing pulses, 352 transients, 2kHz spectral width and 2048 points. The voxel varied in location and was (3.5 cm)3 or (3 cm)3 depending on the tumor size and data were acquired with TEs of 70, 90, and 120 ms for each participant. Data were preprocessed using Gannet5 with retrospective phase and frequency correction in the time domain6.Spatial-resolved simulations were performed using FID-A7 across a 19x19 matrix spanning 3.6x3.6 cm2 in the two refocusing pulse directions with TEs that ranged from 70-160 ms. Basis sets were also constructed from these simulations for fitting the in vivo spectra, which was performed with ProFit-1D8. Metabolite T2s were estimated by fitting the simulated edited metabolite integrals as a function of TE to the in vivo data9.
Results
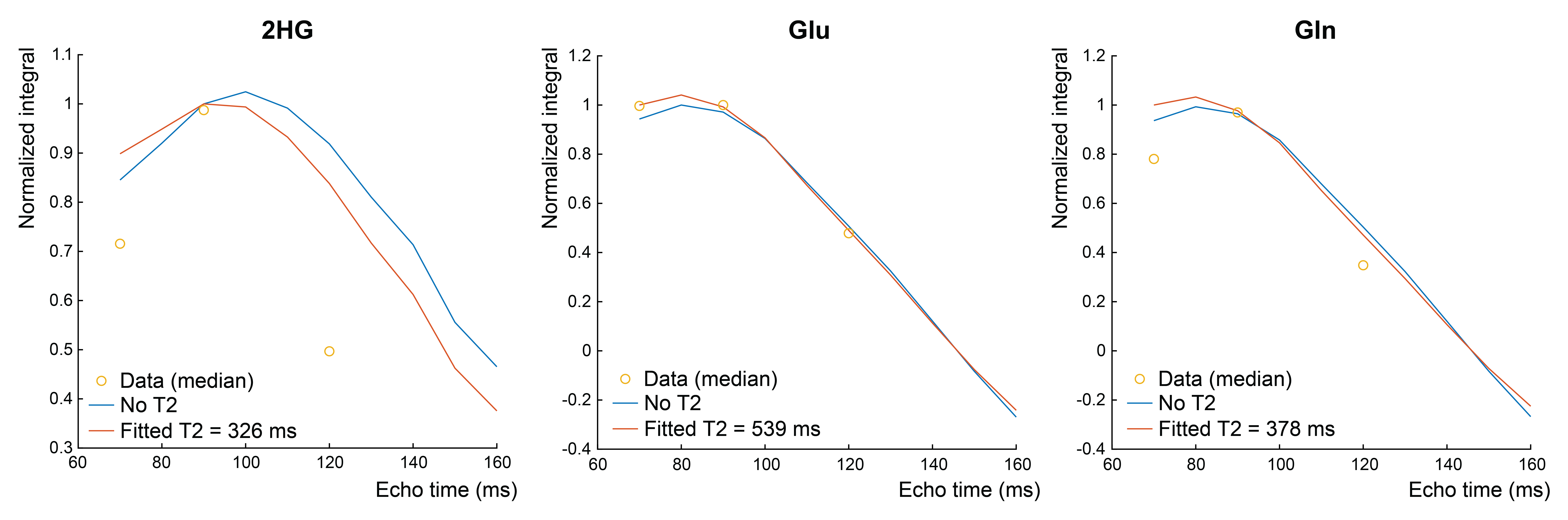
Spatial simulations are shown in Figure 1. In the horizontal direction (first refocusing pulse), no spatial dependency of the 2HG multiplet was seen. In the vertical direction (2nd refocusing pulse), two regions can be seen in the OFF spectra where the multiplets are negative as desired in the green region and positive in the red region. Conversely, the ON multiplets are positive across the entire voxel. Thus, subtracting the two results in positive signal in the green region but none in the red region. Figure 2a shows the evolution of the ON, OFF, and DIFF spectra as the TE is changed where it can be seen that the edited 2HG resonance reaches a maximal value when the TE is 90ms. This is confirmed in Figure 2b where it can be seen that the maximal 2HG-edited integral is at 90-100ms. Figure 3 shows the edited 2HG peak and the adjacent Glu+Gln (Glx) peak with 8-Hz and 14-Hz line broadening. At 14-Hz line broadening, 2HG and Glx are better separated at TE 70ms. Figure 4a shows high-quality in vivo spectra at all TEs with good fits while Figure 4b shows the normalized integrals for 2HG, Glu, and Gln which is highest at TE 90ms. The fitted T2s for 2HG, Glu, and Gln were 326 ms, 539 ms, and 378 ms, respectively. Figure 5 shows the normalized integrals as a function of TE with and without the fitted T2 relaxation constants. Thus, the optimal TE did not change significantly when taking T2 into consideration.Discussion
Both simulations and in vivo experiments showed that 2HG is generally better detected at a TE of 90ms than at TE 70ms or 120ms. Compared with the commonly used TE of 70ms, a TE of 90ms resulted in ~38% higher signal. It should be noted, however, that the optimal TE for 2HG-editing varied significantly between patients. This might be due to differences in tissue composition such as varying amounts of edema which has been shown to significantly alter metabolite T2s10. Although TE=90ms provided the highest 2HG signal, TE 70ms resulted in somewhat reduced overlap between 2HG and the co-edited Glx signal at higher linewidths. Thus, a TE of 70ms might be a better choice in situations where the shimming is poor such as the presence of a nearby metal implant from a prior surgical resection.Acknowledgements
This work was funded by the Cancer Prevention and Research Institute of Texas (CPRIT) (Grant Number: RR180056, Principal Investigator: Anke Henning, PhD).References
1. Chan et al., Magn Reson Med. 2016
2. Branzoli et al., Neuro Oncol. 2018
3. Juskanič et al., MAGMA. 2022
4. Andronesi et al., Sci Transl Med. 2012
5. Edden et al., J Magn Reson. Imaging. 2014
6. Near et al., Magn Reson Med. 2015
7. Simpson et al., Magn Reson Med. 2015
8. Borbath et al., Magn Reson Med. 2021
9. Edden et al., J Magn Reson Imaging. 2012
10. Sijens and Oudkerk, Eur Radiol. 2002
Figures