3252
Rapid, motion robust T2w and T2FLAIR imaging1GE Healthcare, Munich, Germany, 2Karolinska Institute, Stockholm, Sweden, 3Karolinska University Hospital, Stockholm, Sweden
Synopsis
Keywords: Pulse Sequence Design, Multi-Contrast, Rapid imaging
Motivation: The T2w and T2FLAIR are extremely versatile MRI contrasts and paramount to asses a wide range of pathologies in neuroimaging.
Goal(s): A highly efficient acquisition strategy is proposed that jointly acquires T2w and T2FLAIR full brain data in a little more than half a minute.
Approach: Single shot FSE readouts, inversion pulses and saturation bands are strategically interleaved to maximize sampling efficiency and avoid dummy TRs. Prospective motion correction is added to increase robustness.
Results: Volunteer results comparing different protocols, a motion experiment and a pediatric scan are presented. Acceptable image quality was achieved even under severe motion.
Impact: A half minute, motion robust, whole brain T2w and T2FLAIR scan is very interesting for clinical neuroimaging. It is potentially very useful for acute MR, pediatric imaging, screening, disease progression or treatment monitoring.
Introduction
The T2w and T2FLAIR are among the most important clinical MRI contrasts and are part of many neuroimaging protocols. Here we propose a highly efficient acquisition strategy that jointly acquires T2w and T2FLAIR single shot FSE (SSFSE) images with full brain coverage in half a minute. Even for motion-robust SSFSE readouts, through-plane motion remains challenging for T2FLAIR where a spatial mismatch of the inversion slice and readout slice (played 3 s apart) can lead to unsuppressed CSF signal [1]. To address this issue, we add low-latency prospective motion-correction (PMC) [2] to our sequence to further increase utility in the case of non-cooperative patients.Methods
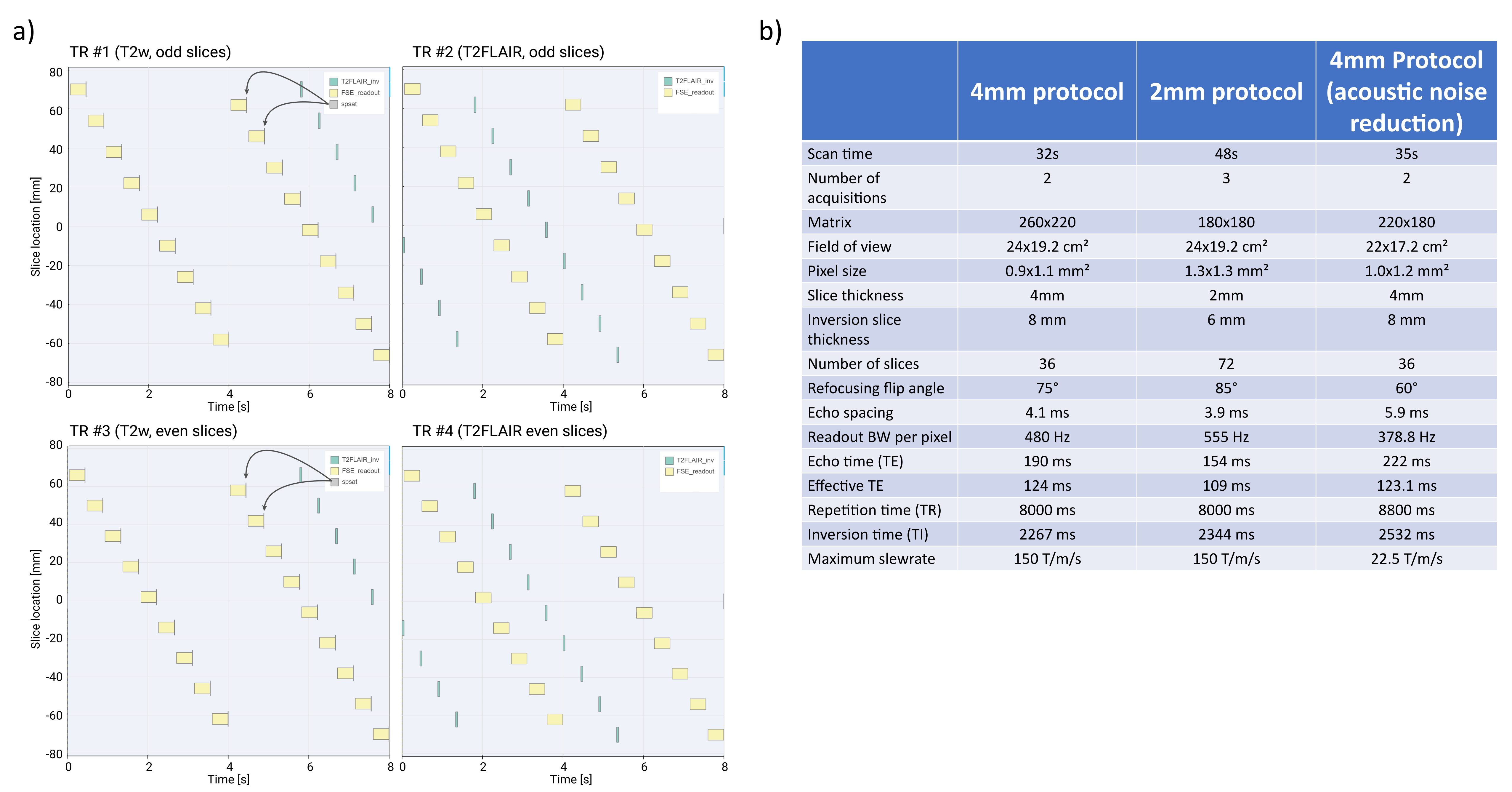
T2FLAIR’s ability to fully suppress free water is sensitive to slice crosstalk and the magnetization history. Consequently, the scan is usually split in two acquisitions (odd and even slices) and a dummy TR is required at the beginning of each acquisition.In this work, these dummy TRs were replaced with T2w SSFSE acquisitions that serve as a preparation for the subsequent inversion pulses (Fig. 1a). The saturation effect of each T2w SSFSE readout was enhanced by applying a complex slice-selective saturation RF pulse immediately afterwards, which was also made with a wider slice thickness for increased efficiency. The interleaving of readout sequences and inversion sequences enabled continuous sampling of the T2w (Fig. 1a TRs 1 and 3) and the T2FLAIR (Fig. 1a TRs 2 and 4) contrast with nearly zero “non-acquisition time”.
Prospective motion correction was setup using the WRAD [2], which was placed on the subject’s forehead. Corresponding WRAD-navigator modules (not shown in Fig. 1 for simplicity, see [2]) are played prior to the inversion pulse resulting in an update latency of about 14 ms for the inversion pulse and 24 ms for the SSFSE readout [3].
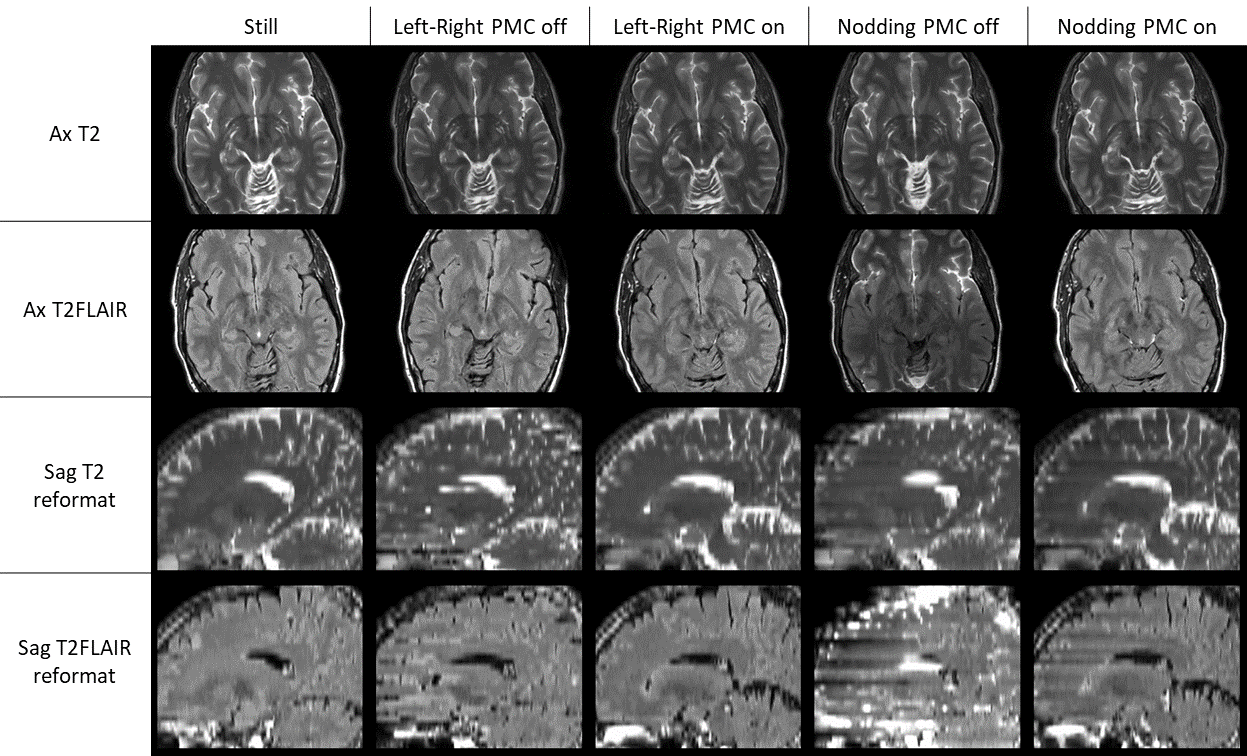
All experiments were run on a GE Healthcare 3T SIGNA™ Premier with a 48ch head coil. A healthy volunteer was asked to perform; a) no motion, b) left-right head motion, c) nodding motion, the latter two with and without PMC. For a pediatric patient scan, the sequence was run with acoustic noise reduction (Fig. 1c). All images were denoised with level “high” using the vendor-provided reconstruction software AIR™ Recon DL.
Results
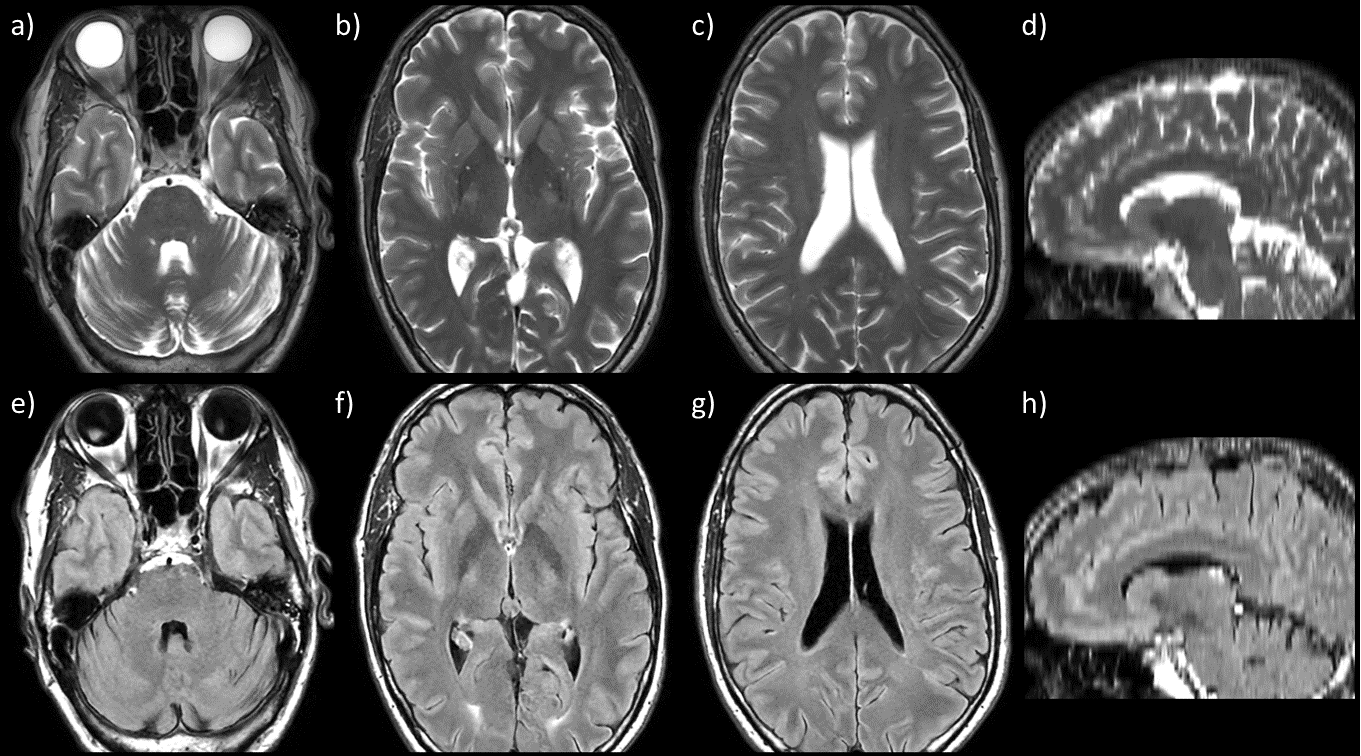
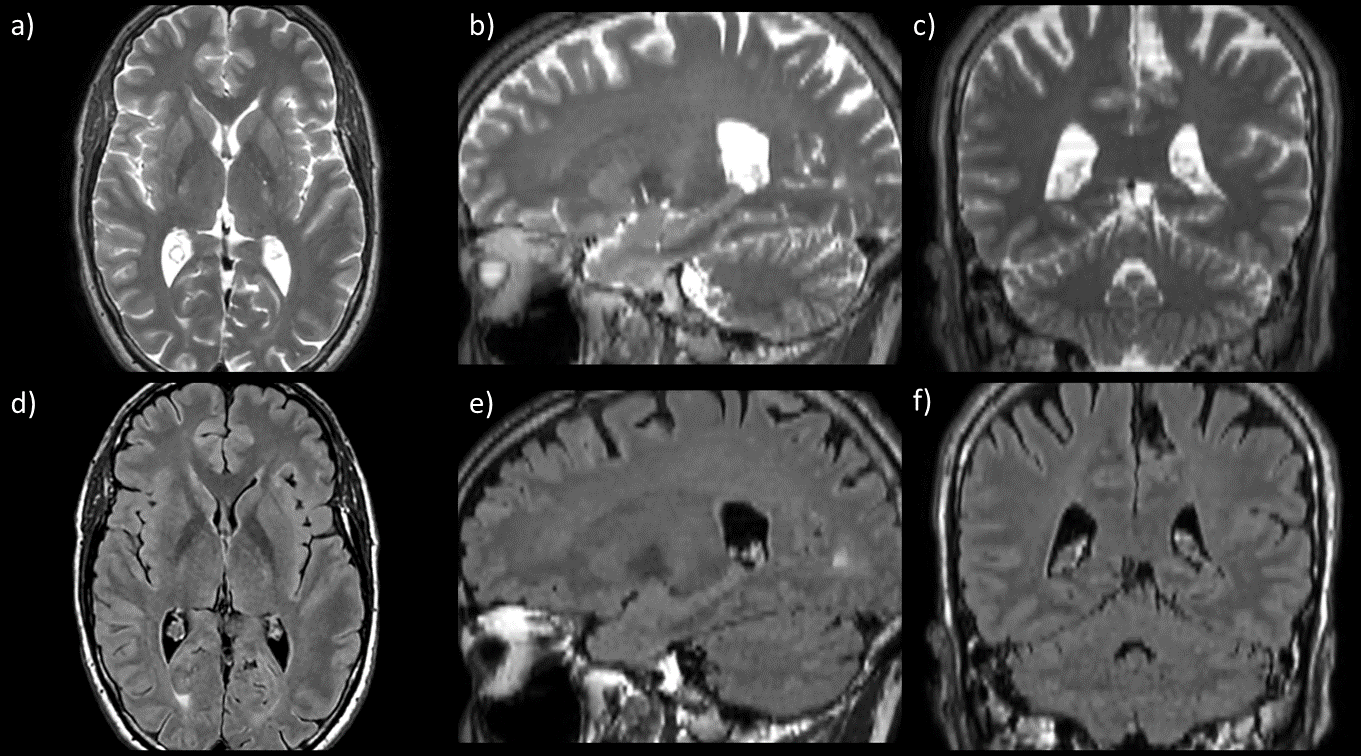
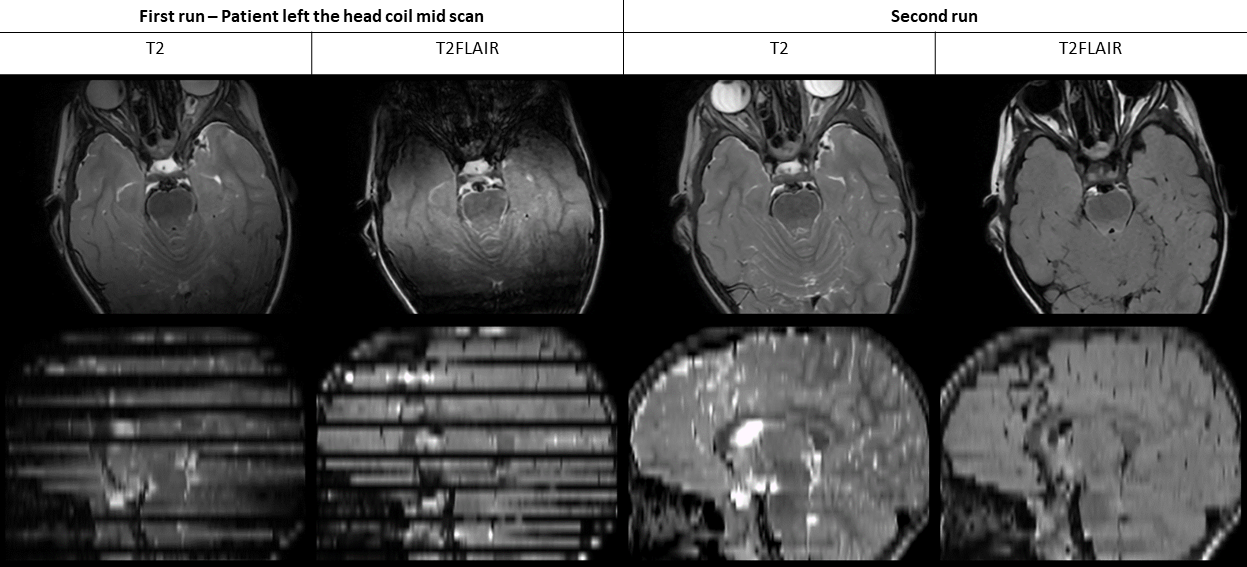
The parameters of three different experiments are overviewed in Fig. 1c. Volunteer results of the 4 mm protocol and the 2 mm protocol are depicted in Fig. 2-3. A comparison of the native plane images (Fig. 2a-f vs. 3a-b) reveals the higher in plane resolution of the 4 mm protocol but the far higher slice resolution of the 2mm protocol is apparent in the reformats (Fig. 2g-h vs. 3c-f). The CSF suppression of the T2FLAIR contrast was sufficient for both protocols. The motion experiments (Fig. 4) show generally usable images for left-right motion but sagittal reformats of that data reveals discontinuities without PMC. Under left-right motion with PMC, the sagittal reformats appear artifact free. For nodding motion, the T2FLAIR contrast without PMC suffered from strong hyperintense CSF signal due to the out-of-plane motion. Nodding motion with PMC resulted in images with good CSF suppression with few exceptions. The pediatric patient moved its head completely outside the head coil during the scan, which cannot be addressed with PMC. Nevertheless, a repeated scan resulted in sufficient image quality (Fig. 5).Discussion
The proposed joint T2 and T2FLAIR sequence may be a fast and motion-robust alternative for uncooperative patients. Three protocols were investigated with scan times ranging from 32 s and 48 s. A comparison of diagnostic value between the thin slice 2 mm protocol (48 s) and the high resolution 4 mm protocol (32 s) is subject of future work. For uncooperative patients, such as young children that are scanned without sedation, adding PMC was important, especially for T2FLAIR. The very short scan time also made it easy to rerun the sequence in case the scan had to be interrupted. We also implemented a 4 mm protocol with acoustic noise reduction as an option for certain patient cohorts.The proposed acquisition technique lends well for acute MR, pediatric imaging, screening, disease progression or treatment monitoring, both with and without PMC.
Acknowledgements
This project received research support through GE Healthcare.References
[1] Sprenger, T, Kits, A, Norbeck, O, et al. NeuroMix—A single-scan brain exam. Magn Reson Med. 2022; 87: 2178–2193. doi:10.1002/mrm.29120
[2] van Niekerk A, Meintjes E, van der Kouwe A. A Wireless Radio Frequency Triggered Acquisition Device (WRAD) for Self-Synchronised Measurements of the Rate of Change of the MRI Gradient Vector Field for Motion Tracking. IEEE Trans Med Imaging. 2019 Jul;38(7):1610-1621. doi: 10.1109/TMI.2019.2891774. Epub 2019 Jan 10. PMID: 30629498; PMCID: PMC7192240.
[3] Norbeck, O, van Niekerk, A, Avventi, E, et al. T1-FLAIR imaging during continuous head motion: Combining PROPELLER with an intelligent marker. Magn Reson Med. 2020; 85: 868–882. https://doi.org/10.1002/mrm.28477
Figures