3246
Novel method of Ultrashort TE 4D MR Angiography – Continuous Acquisition Variable TR (CAVTR) with View Sharing.1Department of Radiology, Graduate School of Medicine, University of Tokyo, Tokyo, Japan, 2Department of Radiology, Juntendo University Graduate School of Medicine, Tokyo, Japan, 3Department of Radiology, Juntendo University Hospital, Tokyo, Japan
Synopsis
Keywords: Pulse Sequence Design, Arterial spin labelling, UTE, 4D MRA
Motivation: The conventional multi-phase Pulsed ASL UTE 4D MRA sometimes provides insufficient signal intensity to visualize hemodynamic flow characteristics in late phases.
Goal(s): Our goal is to improve the visibility of multi-phase Pulsed ASL UTE 4D MRA.
Approach: We developed a novel method, Continuous Acquisition Variable TR (CAVTR) UTE 4D MRA pulse sequence which utilizes continuously increasing TR. This new pulse sequence has less signal fluctuation and can avoid late phase signal reduction. We combined CAVTR with view sharing and improved late phase image quality without detriment to temporal resolution.
Results: This novel method can improve clinical usability of non-contrast ASL based UTE 4D-MRA.
Impact: The novel method, Continuous Acquisition Variable TR pulse sequence with View Sharing achieved both high temporal resolution and good visibility of arteries in late phases. This novel method can improve clinical usability of non-contrast ASL based UTE 4D-MRA.
INTRODUCTION
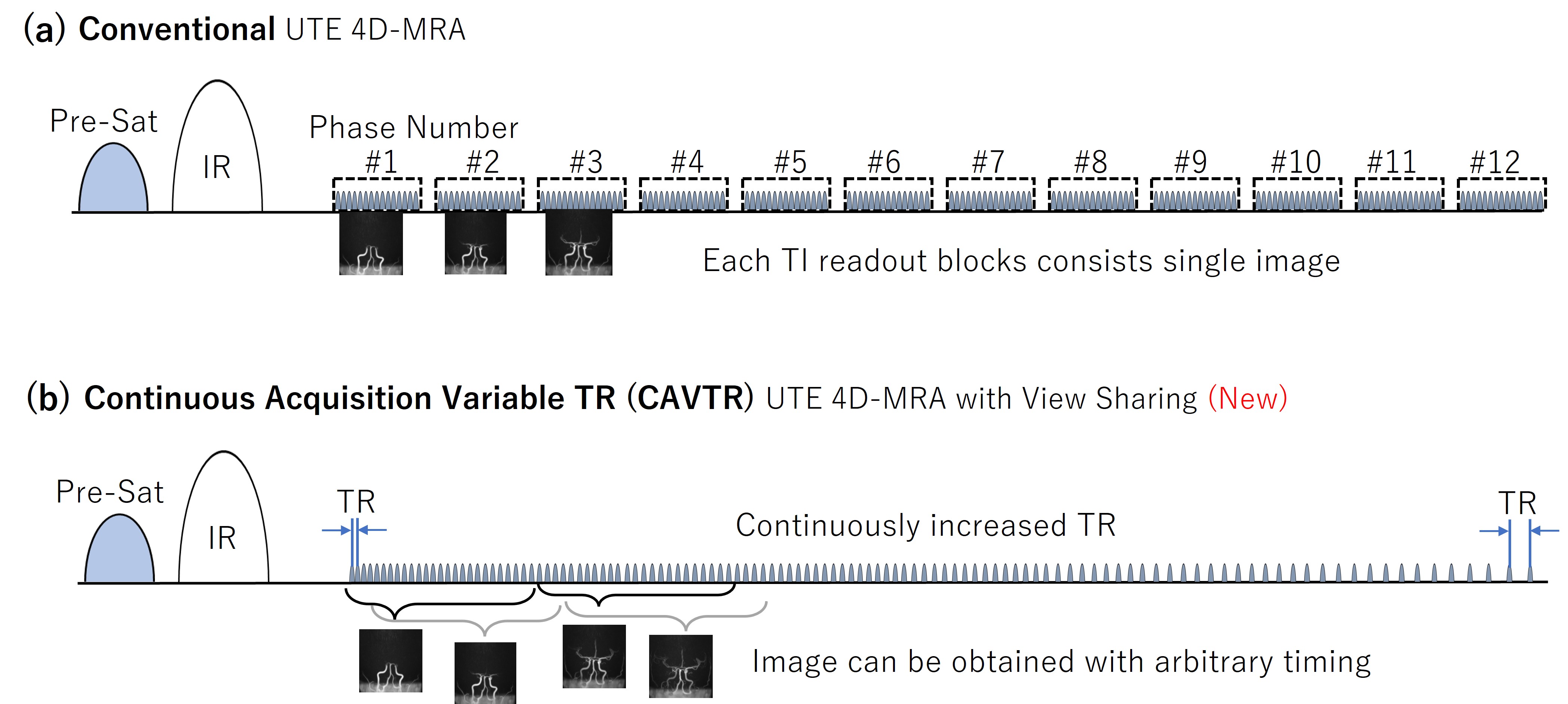
The Arterial Spin Labeling (ASL) based 4D ultrashort TE (UTE) MR angiography (MRA) has been applied to visualize hemodynamic information. However, the conventional multi-phase Pulsed ASL UTE 4D MRA sometimes provides insufficient signal intensity to visualize hemodynamic flow characteristics in late phases. The Pulsed ASL has high labeling efficiency but the signal from the blood reduces due to the relaxation of the longitudinal magnetization to the equilibrium. The conventional multi-phase acquisition method utilizes the Look-Locker acquisitions. In readout process, UTE radio frequency (RF) pulses were repeated with repetition time (TR) of typically 3 – 4 ms. This rapidly repeated UTE pulses accelerate the T1 relaxation. To overcome the late phase signal reduction, we developed Variable Inversion Time (VTI) method and reported in ISMRM2020 and ISMRM2021. It is certain that the VTI method could enhance signal intensity in late phases by increasing TI interval in late phases, but this method has the disadvantage with its blank time (longer wait time between each TIs in later phases) which reduced the temporal resolution in late phases. In this study, we implemented Continuous Acquisition Variable TR (CAVTR) method to overcome problems of both signal reduction and temporal resolution. We combined the CAVTR method with view sharing to reconstruct the image from arbitrary timing. We conducted numerical simulation and volunteer study, and confirmed that the both high signal intensity and temporal resolution were achieved with this new method.METHODS
The numerical simulations for ASL signal were performed with MatLab (R2022b, MathWorks, Natick, MA). All subjects were scanned on a 3 Tesla MRI scanner (Vantage Galan 3T ZGO, Canon Medical Systems Corporation, Japan) using a 32-channel head coil . The data acquisition was based on a 3D radial sampling, and ASL technique was used as a preparation pulse to visualize blood flow. The UTE readout used half sinc pulses with a duration of about 30 μs and flip angles up to 6°. Imaging parameters were as follows: FOV = 224 x 224 mm2, number of slices = 200, resolution = 1 x 1 x 1 mm3, TE = 0.1 ms, shot interval = 2800 ms, 7950 radial projections were acquired within 14 minutes. Conventional UTE 4D MRA utilized Look-Locker acquisition and the each readout consisted of a series of readout blocks, data from each block constructed a single image. The UTE pulse was continuously repeated with fixed TR of 3.7ms in conventional method. For CAVTR method, the first TR = 3.7ms and following TRs continuously increased in a manner of arithmetic progression with common difference of ⊿TR. All the acquisitions were performed using otherwise identical imaging parameters. Six healthy volunteers (3 males, 3 female; mean age, 38 years) without history of cerebrovascular diseases were scanned. For comparison, volunteers were scanned with the conventional and CAVTR method and evaluated for visibility of arteries.RESULTS
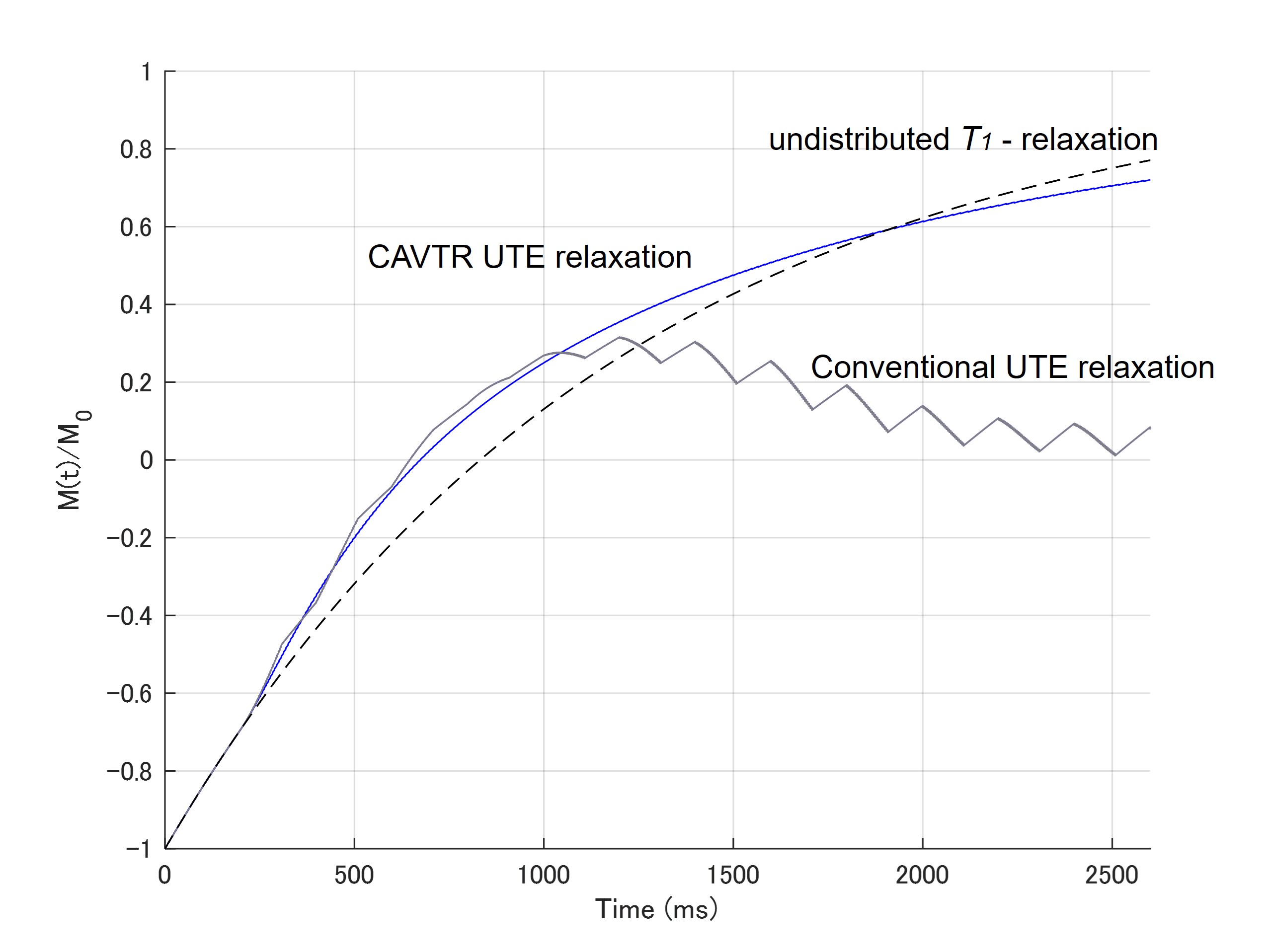
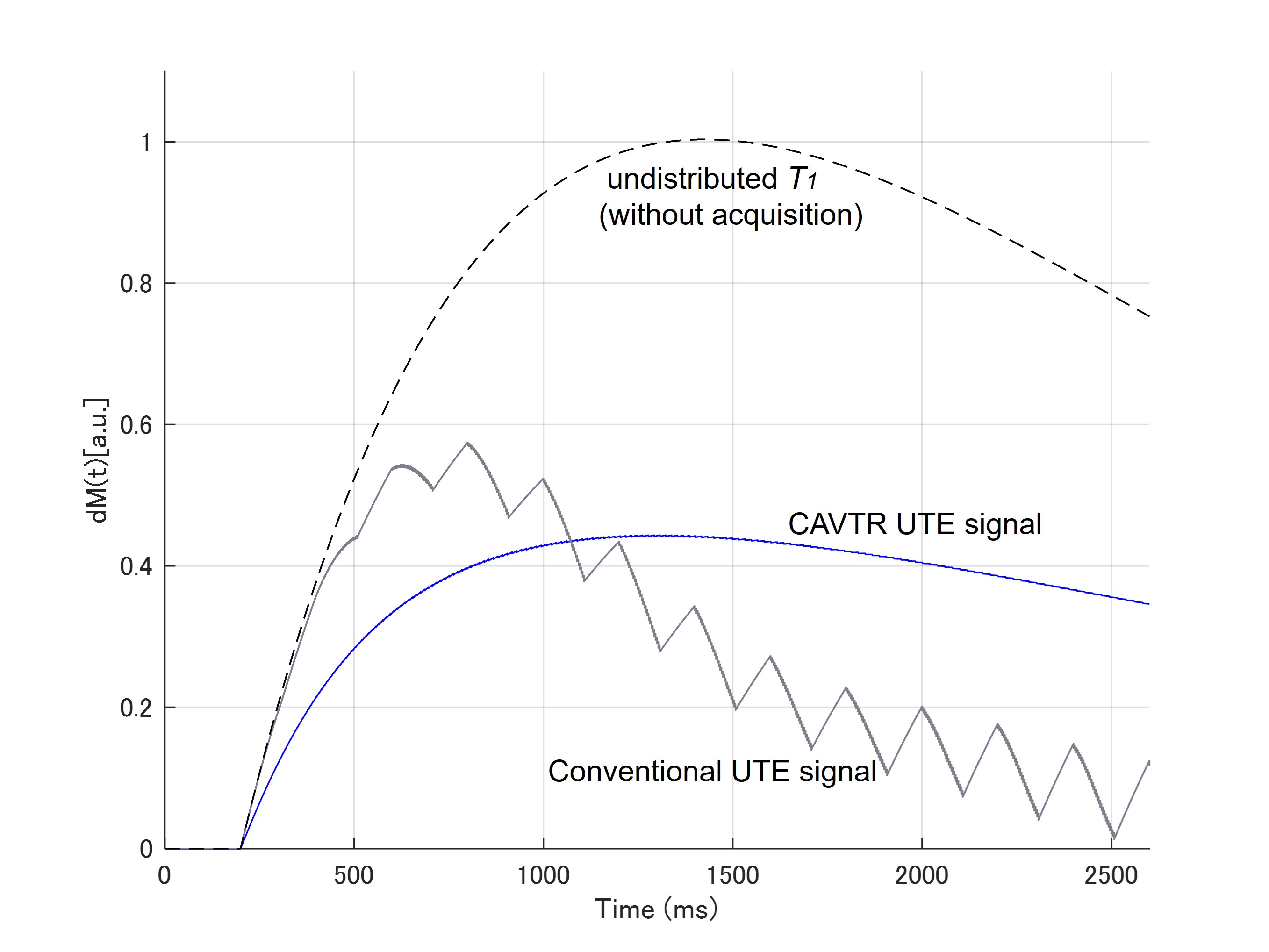
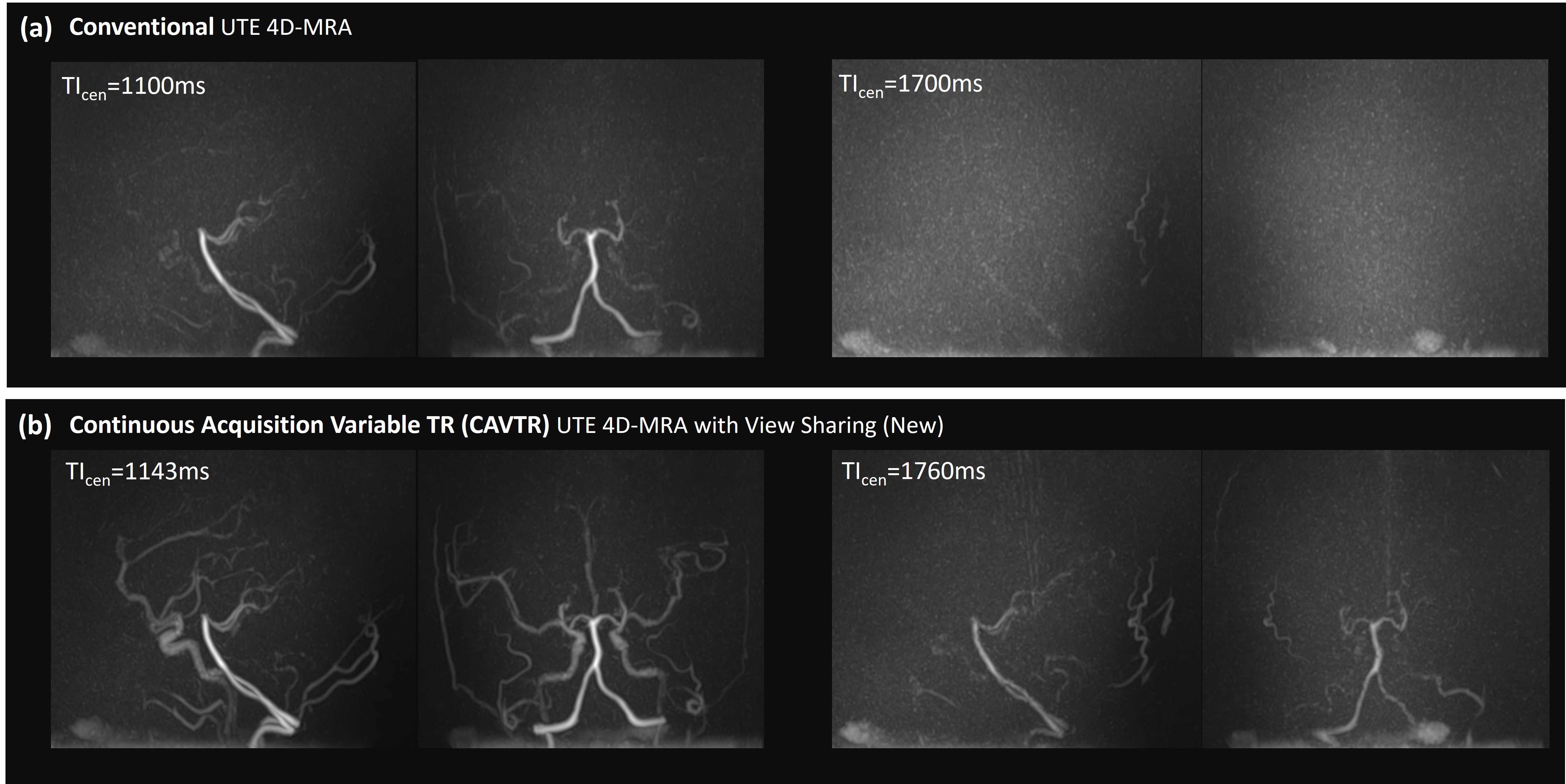
As shown in Figure 2, the conventional method saturated the magnetization rapidly. On the other hand, CAVTR method keeps the magnetization away from saturation. As shown in Figure 3, the signal intensity of conventional method rapidly decreased in repeated readout blocks and thus the signal reduced in late phases. On contrary, CAVTR method prevented the rapid signal reduction by TR modification. In the volunteer study, CAVTR method allowed improved visualization of the arteries. With view sharing, we can reconstruct the image with arbitrary timing without deterioration of image quality.DISCUSSION
From the numerical simulations, as shown in Figure 2, the longitudinal magnetization saturates rapidly in each readout blocks with the conventional method. On the other hand, the CAVTR method prevents the magnetization from saturation. The acquired signal in the ASL method is proportional to the difference between labeled and control measurement, thus saturation of the magnetization reduces the signal intensity. The CAVTR method prevents the longitudinal magnetization from saturation and prevents signal decay in late phases as shown in Figure 3. For conventional method, the rapid signal reduction during repetitive UTE acquisition is unavoidable. We changed the conventionally fixed TR to variable TR without compromising image quality nor any artifacts owing to the characteristic of UTE acquisition. By using CAVTR, the acquired signal intensity was stabilized, less fluctuated comparing to conventional method. This feature contributes to stable reconstruction with view sharing.CONCLUSION
In this study, we presented the ability of CAVTR UTE 4D MRA with View Sharing to visualize hemodynamic flow characteristics of cerebral veins. This new method can achieve both late phase signal intensity and high temporal resolution. The CAVTR technique have potential to be applied to other applications.Acknowledgements
None.References
- Tyler DJ, Robson MD, Henkelman RM, Young IR, Bydder GM. Magnetic resonance imaging with ultrashort TE (UTE) PULSE sequences: technical considerations. J Magn Reson Imaging 2007; 25: 279–289.
- Gönner F, Heid O, Remonda L, et al. MR angiography with ultrashort echo time in cerebral aneurysms treated with Guglielmi detachable coils. AJNR Am J Neuroradiol 1998;19:1324–28 pmid:9726477
- Nielsen HTC, Gold GE, Olcott EW, Pauly JM, Nishimura DG. Ultra-short echo-time 2D time-offlight MR angiography using a half-pulse excitation. Magn Reson Med 1999;41:591–599.
- Larson PEZ, Conolly SM, Pauly JM, Nishimura DG. Using adiabatic inversion pulses for long-T2 suppression in ultrashort echo time (UTE) imaging. Magn Reson Med. 2007;58(5):952–961.
- Takano N, Suzuki M, Irie R, et al. Usefulness of non-contrast-enhanced MR angiography using a silent scan for follow-up after Y-configuration stent-assisted coil embolization for basilar tip aneurysms. AJNR Am J Neuroradiol 2017;38:577–81.
Figures