3237
Practical sampling strategies for volumetric cardiac real-time MRI using stack-of-spirals at 0.55T1Ming Hsieh Department of Electrical and Computer Engineering, University of Southern California, Los Angeles, CA, United States, 2Cardiovascular Branch, National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, MD, United States
Synopsis
Keywords: Data Acquisition, Data Acquisition, Low-field MRI, Acquisition Methods, Cardiovascular
Motivation: Volumetric real-time MRI is desirable to accurately characterize beat-to-beat cardiac function in patients with arrythmia or heart failure.
Goal(s): To identify practical data sampling strategies for volumetric real-time MRI and evaluate cardiac volume measurements against gated reference scans.
Approach: We focus on stack-of-spirals bSSFP at 0.55T. We use simulations and in-vivo experiments to compare three sampling strategies that minimize eddy currents.
Results: A Gaussian distribution of the stack-of-spirals was found to provide the best real-time image quality and most accurate LV volumes, with under-estimation of end-diastolic volume by 7.44% and over-estimation of end-systolic volume by 18.33%.
Impact: Beat-to-beat cardiac function is important to measure in the context of arrhythmia, cardiac stress testing and in interventional MRI, where real-time volumetric coverage will facilitate assessment and monitoring of cardiac function.
Introduction
Cine MRI is the gold standard for the evaluation of cardiac ventricular function. Cine imaging typically requires the use of breath holds, which are not tolerated in roughly 10% of patients, and electrocardiogram (ECG) gating, which is not robust in patients with arrhythmia. Real-time MRI (RT-MRI)1 is an alternative that does not rely on breath-holds or external gating and can characterize beat-to-beat changes in cardiac function and regional wall motion. This capability is also useful in the evaluation of pressure-volume loops2. The obstacle to volumetric, or “3D”, RT-MRI is managing the trade-off between spatio-temporal resolution and image quality.We compare several data sampling strategies that could make 3D RT-MRI of the human heart possible. We limit our scope to the 0.55T field strength3, balanced steady-state free precession (bSSFP) contrast, stack-of-spirals (SoS) trajectories with golden-angle rotations, and a 3D spatio-temporally constrained reconstruction (STCR)4. We study several view-orders for 3D sampling in both simulation and in-vivo and investigate acquisition schemes that minimize aliasing to best estimate left ventricular (LV)5,6 volume.
Methods
This is a multicenter study between two institutions (NIH/USC). Experiments were performed on equivalent 0.55T systems (prototype MAGNETOM Aera, Siemens Healthineers, Germany) equipped with high-performance shielded gradients (45mT/m amplitude, 200T/m/s slew rate). RT-MRI sequences were implemented in IDEA (Siemens Healthineers) (NIH) and in the RTHawk system (Vista.AI, Palo Alto CA)7(USC). Three healthy volunteers were scanned under protocols approved by each Institutional Review Board.Data was acquired with SoS trajectory and a resolution of 2.5x2.5x8.0mm3, short-axis orientation, with whole LV coverage. We excite a 100mm slab (TBW=8) with 33% oversampling and 12 slice encodes. For comparison, prospectively gated 3D SoS cine (2.5x2.5x8mm3) and 2D multi-slice Cartesian cine (1.5x1.5x8mm3) were acquired using ECG gating. Prospective SoS cine data were resampled to simulate 4 heartbeats of real-time acquisition using three different kz sampling schemes as described below. Line profiles were used to compare the simulated real-time data to the prospectively sampled cines.
Figure 1 illustrates three sampling strategies considered to achieve a temporal resolution of 80ms/frame: 1) “linear” in kz with golden-angle rotation after every full stack of 16 slice encodes, 2) “half-linear” with golden-angle rotation after every 8 slice encodes and half-k z sampling (spreads under-sampling along the kz and kxy planes), and 3) “gaussian” density along kz (more densely sample in central kz) with a golden-angle rotation every TR.
Prospectively gated SoS cine images are reconstructed via gridding and optimal coil combination using the Walsh method8. Real-time images are reconstructed using STCR. The following cost function is minimized using non-linear conjugate gradient descent using a Dai-Yuan beta9.
$$argmin_x||\widehat{W}F_sCx-\widehat{W}y||_2^2+\lambda_{TFD}\psi(\nabla_tx)+\lambda_{TV}\psi(\nabla_{TV}x)+\lambda_{sTV}\psi(\nabla_{sTV}x)$$
$$\psi(x) := |x|*log(1+|\frac{x}{\delta}|)$$
Where x is the image, y is the k-space data, $$$\widehat{W}$$$ corresponds to the square-root of the density compensation function, $$$F_s$$$ is the non-Cartesian Fourier operator, C is the coil sensitivity operator, $$$\psi(x)$$$ approximates the L1 function, $$$\delta$$$ is a small smoothing parameter, $$$\lambda_*$$$ are regularization parameters, $$$\nabla_t$$$ is the temporal finite difference operator, $$$ \nabla_{TV} $$$ is a total variation operator, and $$$\nabla_{sTV}$$$ is a slice finite difference operator. All data are reconstructed using gradient impulse response function10 predicted trajectories.
Volume and ejection fraction measurements were made using semi-automatic cardiac segmentation software (suiteHEART NeoSOFT). The middle 8 slices of SoS data were segmented and compared against matched slices from the cartesian acquisition.
Results
Figure 2 shows results from simulated RT-MRI by re-sampling prospective SoS cine. Half-kz and gaussian kz sampling schemes show better temporal characteristics, compared to linear, particularly during systole.Figure 3 shows in-vivo volumetric RT-MRI compared to prospective cine. Gaussian sampling removes aliasing artifacts that occur in other view orders and resolves the most temporal dynamics when compared via temporal line profiles.
Figure 4 shows in-vivo volumetric RT-MRI with the gaussian sampling scheme, including all short-axis slices and segmentation results.
Table 1 compares volume estimation between a Cartesian reference scan, prospective SoS cine, and 3D RT-MRI with gaussian sampling using 8 matched slices. The agreement by RT-MRI was modest; RT-MRI underestimates end-diastolic volume by -7.44% and over-estimates end-systolic volume by 18.33%, perhaps due to temporal smoothing.
Discussion
We demonstrate real-time 3D acquisitions in humans with coverage of the LV and with comparable spatial and temporal resolution to previously published 2D approaches for dynamic assessment of contractility and compliance. We observed that a pseudo-gaussian kz distribution minimized aliasing. Future work will improve reconstruction to improve the accuracy of the dynamic volumetry and improve the slice profile to benefit segmentation of edge slices.Conclusion
Real-time volumetric cardiac MRI provides sufficient contrast and spatio-temporal resolution to resolve cardiac motion without aliasing.Acknowledgements
We acknowledge funding from the National Institutes of Health (U01-HL167613), and research support from Siemens Healthineers. We thank Justin Haldar for helpful discussions related to image reconstruction and Ecrin Yagiz for helpful discussions related to simulation.
References
1. Nayak KS, Lim Y, Campbell-Washburn AE, Steeden J. Real-Time Magnetic Resonance Imaging. Journal of Magnetic Resonance Imaging. 2022;55(1):81-99. doi:10.1002/jmri.27411
2. Seemann F, Bruce CG, Khan JM, et al. Dynamic pressure–volume loop analysis by simultaneous real-time cardiovascular magnetic resonance and left heart catheterization. Journal of Cardiovascular Magnetic Resonance. 2023;25(1):1. doi:10.1186/s12968-023-00913-4
3. Campbell-Washburn AE, Varghese J, Nayak KS, Ramasawmy R, Simonetti OP. Cardiac MRI at Low Field Strengths. Journal of Magnetic Resonance Imaging. n/a(n/a). doi:10.1002/jmri.28890
4. Adluru G, McGann C, Speier P, Kholmovski EG, Shaaban A, Dibella EVR. Acquisition and reconstruction of undersampled radial data for myocardial perfusion magnetic resonance imaging. J Magn Reson Imaging. 2009;29(2):466-473. doi:10.1002/jmri.21585
5. Zhao Z, Lim Y, Byrd D, Narayanan S, Nayak KS. Improved 3D real-time MRI of speech production. Magnetic Resonance in Medicine. 2021;85(6):3182-3195. doi:10.1002/mrm.28651
6. Levine E, Daniel B, Vasanawala S, Hargreaves B, Saranathan M. 3D Cartesian MRI with compressed sensing and variable view sharing using complementary poisson-disc sampling. Magnetic Resonance in Medicine. 2017;77(5):1774-1785. doi:10.1002/mrm.26254
7. Santos JM, Wright GA, Pauly JM. Flexible real-time magnetic resonance imaging framework. Conf Proc IEEE Eng Med Biol Soc. 2004;2004:1048-1051. doi:10.1109/IEMBS.2004.1403343
8. Walsh DO, Gmitro AF, Marcellin MW. Adaptive reconstruction of phased array MR imagery. Magnetic Resonance in Medicine. 2000;43(5):682-690. doi:10.1002
9. Dai YH, Yuan Y. A Nonlinear Conjugate Gradient Method with a Strong Global Convergence Property. SIAM J Optim. 1999;10(1):177-182. doi:10.1137/S1052623497318992
10. Campbell-Washburn AE, Xue H, Lederman RJ, Faranesh AZ, Hansen MS. Real-time distortion correction of spiral and echo planar images using the gradient system impulse response function. Magn Reson Med. 2016;75(6):2278-2285. doi:10.1002/mrm.25788
Figures
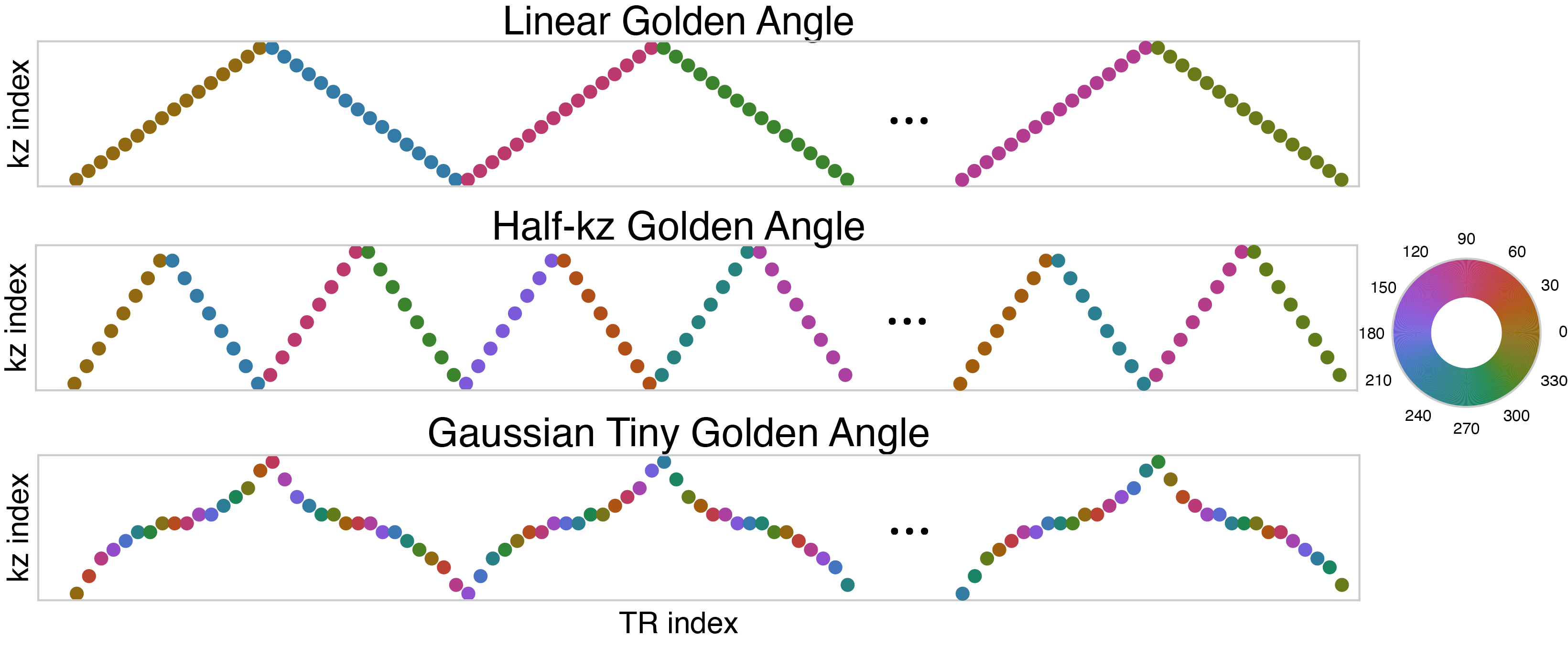
Figure 1: Sampling view orders for stack-of-spiral imaging. The linear view order keeps the same in-plane rotation for all 16 phase encoding steps before rotating by a golden angle increment. The half-kz golden angle rotation has a golden angle rotation after every stack but skips every other phase encode line. The gaussian view order increments by a tiny golden angle step every TR and samples kz in a “gaussian” manner, oversampling the center of k-space to resolve more dynamic motion.
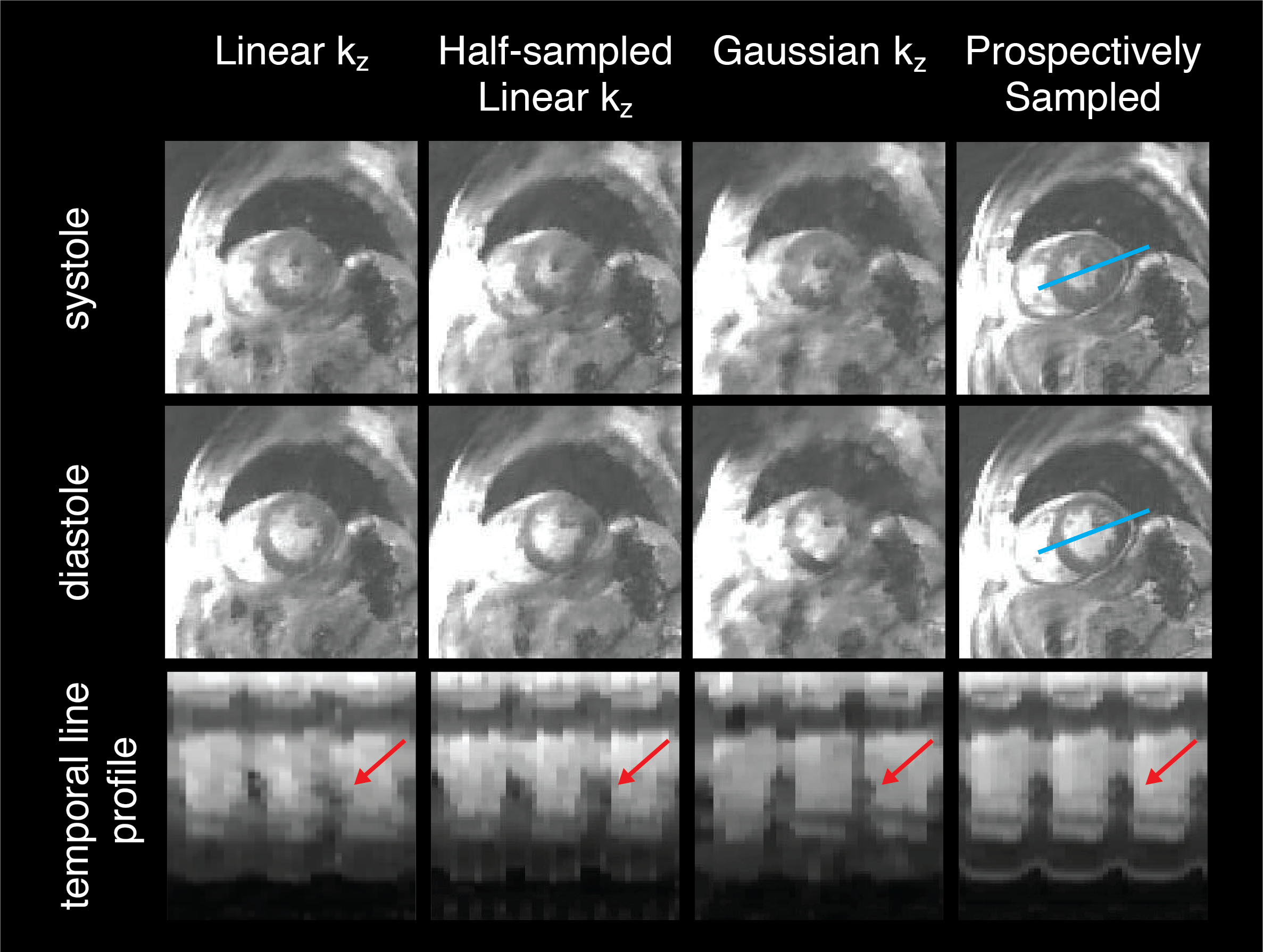
Figure 2: Simulated real-time reconstructions, resampled from a prospectively triggered, fully sampled acquisition. The sampling patterns referred to are described in figure 1. Three different sampling patterns were tested, and compared for image quality to the reference, at systole, diastole and along a temporal line profile across the mid left ventricle (blue line). Visually, the half-kz and gaussian distribution sampling best capture the cardiac motion in simulation (red arrows).
Figure 3: Real-time results, prospectively triggered SoS 3D cine (right) and 2D cartesian cine (left). Three real-time view orders are shown: Linear, Half-kz, and Gaussian, as specified by figure 1. Temporal line profiles along the left ventricle are shown. The gaussian view order shows the least amount of aliasing artifacts when compared to other view orders (red arrows). Gaussian view ordering resolves the most cardiac motion as shown on the temporal line profiles (blue arrows).
Figure 4: Real-time gaussian view-ordered acquisition along with semi-automatic segmentation results. Segmentations are well-defined among basal slices but seem to have larger errors on apical slices (blue arrows).
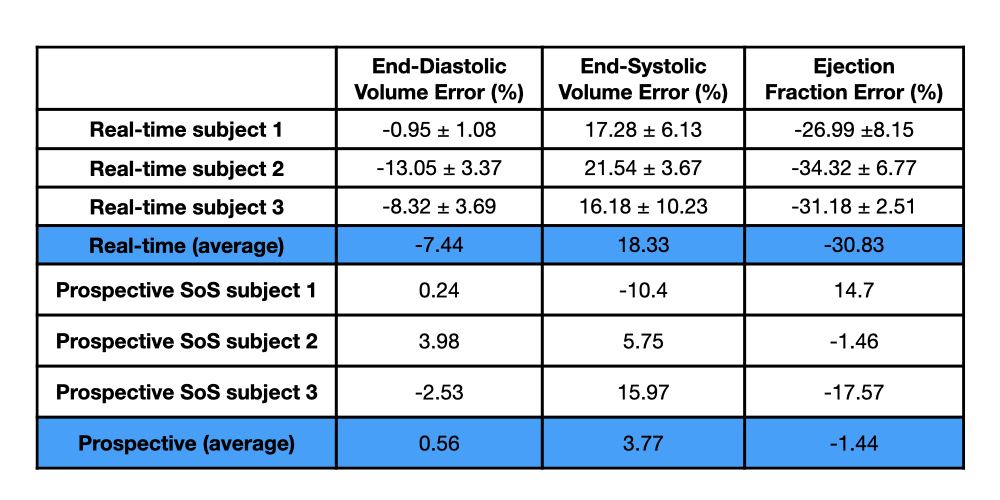
Table 1: Volume error from semi-automatic segmentation, using 8 matched slices from 2D short-axis stack breath-held cartesian cine as the reference. RT-MRI shows a slight underestimation of diastolic volume and an overestimation of systolic volume, with an average error of -7.44% in diastole and 18.33% in systole. Prospectively gated SoS acquisitions more closely match the gated reference with an average error of 0.56% in diastole and 3.77% in systole.