3236
Ultra-fast SWI using 3D-EPI and CAIPIRINHA: a feasibility study at 3-tesla1Department of Neurology, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 2Department of Imaging, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 3Siemens Healthcare Pty Ltd, Brisbane, Australia, 4Siemens Medical Solutions, Los Angeles, CA, United States, 5Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, Los Angeles, CA, United States
Synopsis
Keywords: Data Acquisition, Data Acquisition
Motivation: Conventional gradient echo SWI has a slow acquisition speed, thus limiting the minimal scan time achievable. However, accelerated 3D-EPI sequence can perform fast MR acquisition.
Goal(s): In this study, we evaluated the feasibility of SWI-EPI to generate ultra-fast susceptibility weighted images.
Approach: SWI-EPI combines a 3D (muti-shot) EPI sequence with CAIPIRINHA acceleration to significantly reduce the scan time.
Results: A significant reduction in scan time (up to 70%) was achieved with similar image quality and without any apparent artefacts, thus confirming the feasibility of ultra-fast SWI for future clinical neuro-applications at 3T.
Impact: This study demonstrates the feasibility of ultra-fast SWI-EPI at 3T.
Introduction
Susceptibility weighted imaging (SWI) is a MRI sequence routinely used in clinical imaging to detect blood and iron products in cerebral tissues.1-4 Conventional SWI acquisition relies on a 3D gradient echo (GRE) sequence which has a slow acquisition speed, thus limiting the minimal scan time achievable for standard clinical imaging. To solve this issue, a faster SWI acquisition was recently proposed using wave-controlled aliasing in parallel imaging acceleration (wave-CAIPI SWI) to reduce the scan time by half.5 To further reduce the scan time without compromising image quality, we propose a novel approach, called SWI-EPI, that combines a 3-dimensional echo-planar imaging (3D-EPI)6 sequence with CAIPIRINHA7 to achieve up to 70% reduction in scan time while preserving image quality.Methods
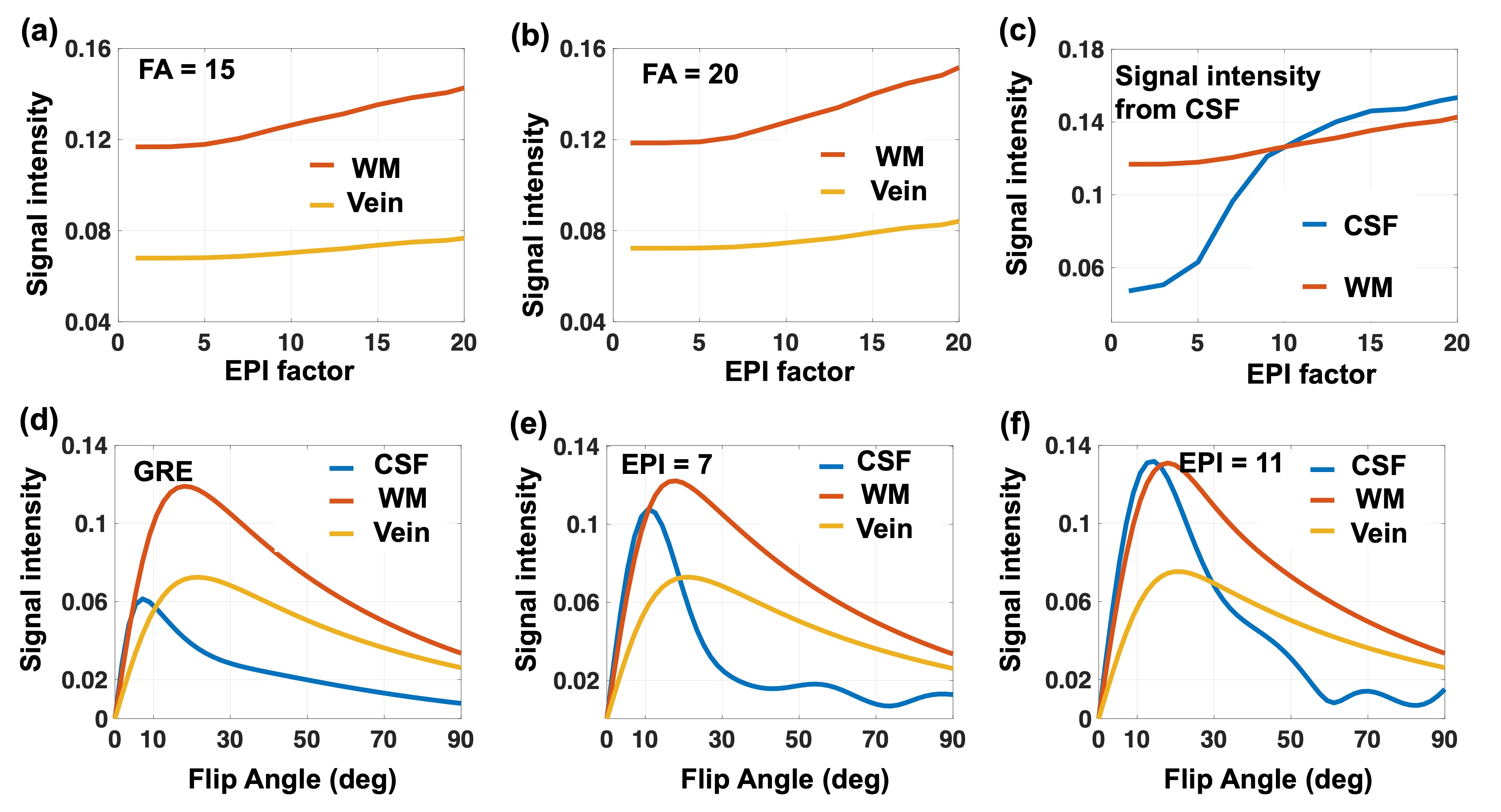
Two healthy controls and one subject with multiple sclerosis (MS) were scanned at Siemens 3T MRI scanner (Erlangen, Germany) with a 20‐channel receiver head coil under an IRB-approved protocol. Standard clinical acquisition parameters were used for all the SWI sequences (SWI-GRE, wave-CAIPI SWI): TE/TR=20/27 ms, slice-thickness=2 mm, flip-angle=15°, voxel-size =0.6×0.6×2 mm, matrix-size=384×312×72. SWI-EPI protocol was created based on research 3D-EPI sequence to match clinical protocols as close as possible, while, TE/TR were slightly modified according to the EPI-factor. Undersampling factors were also adapted according to the type of SWI sequences: R=2×1 (GRAPPA) for SWI-GRE, R=4 for wave-CAIPI SWI and R=1×2 with shift of 1 (CAIPIRINHA) for SWI-EPI. All the SWI images were reconstructed directly on the scanner. To model the effects of the EPI-factor and flip angle (FA) on the signal intensity of the different brain tissues on SWI-EPI, numerical simulations were performed using the Bloch equations. Tissue signal intensity for cerebrospinal fluid (CSF), white matter (WM), and veins were simulated using standard T1/T2 values measured at 3T (CSF:5000/300 ms, WM:832/80 ms and vein:600/25 ms).8-10Results
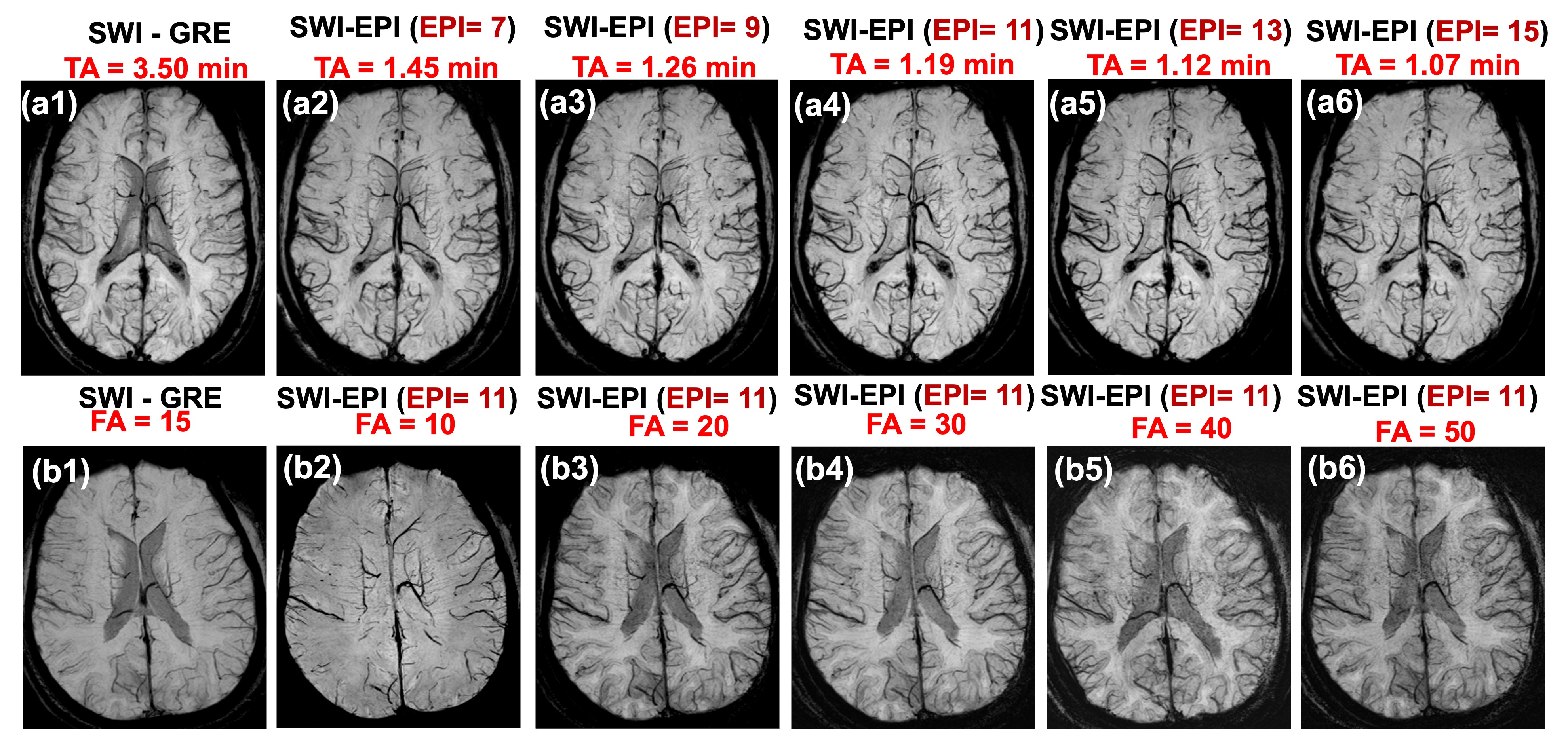
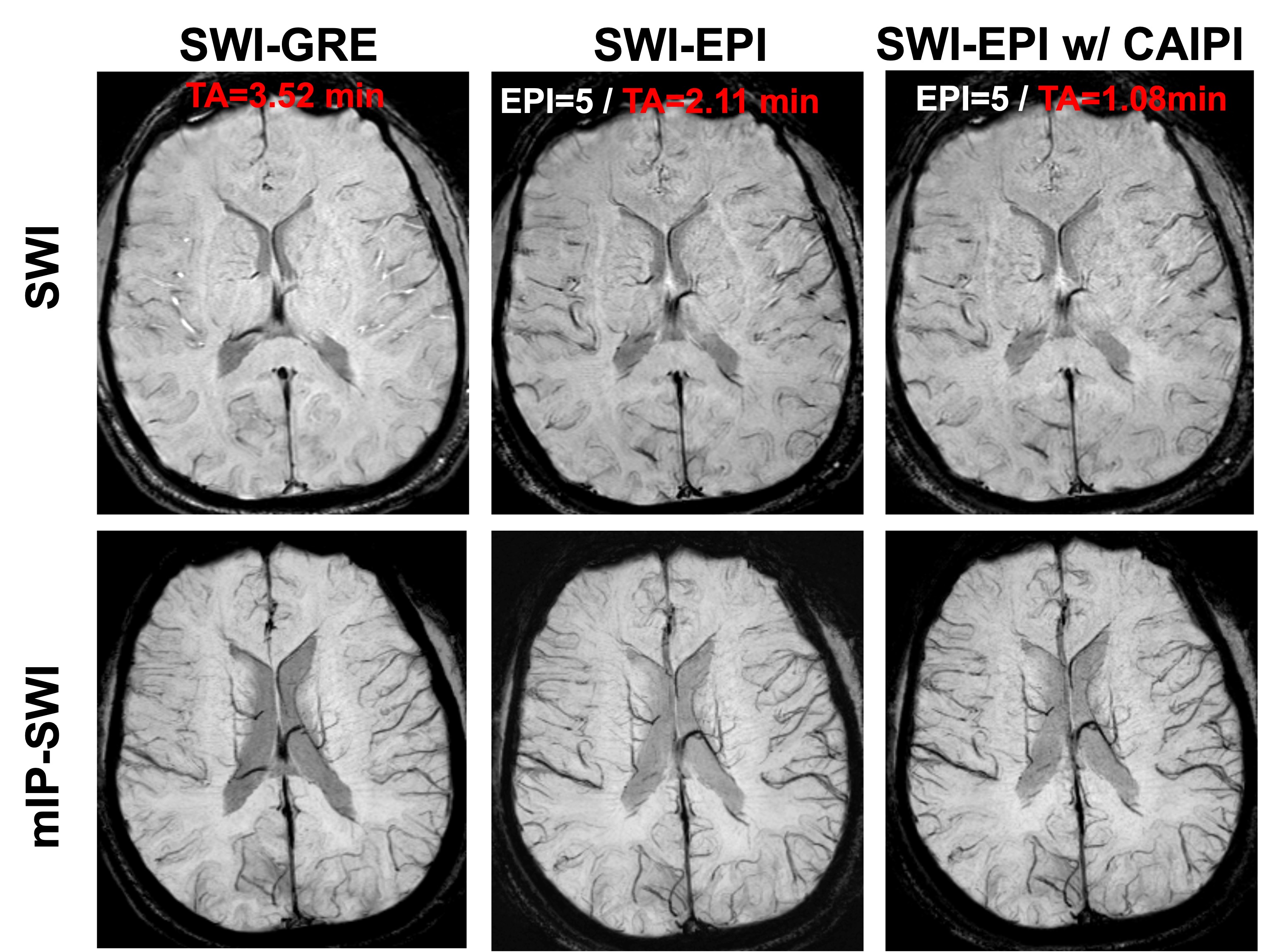
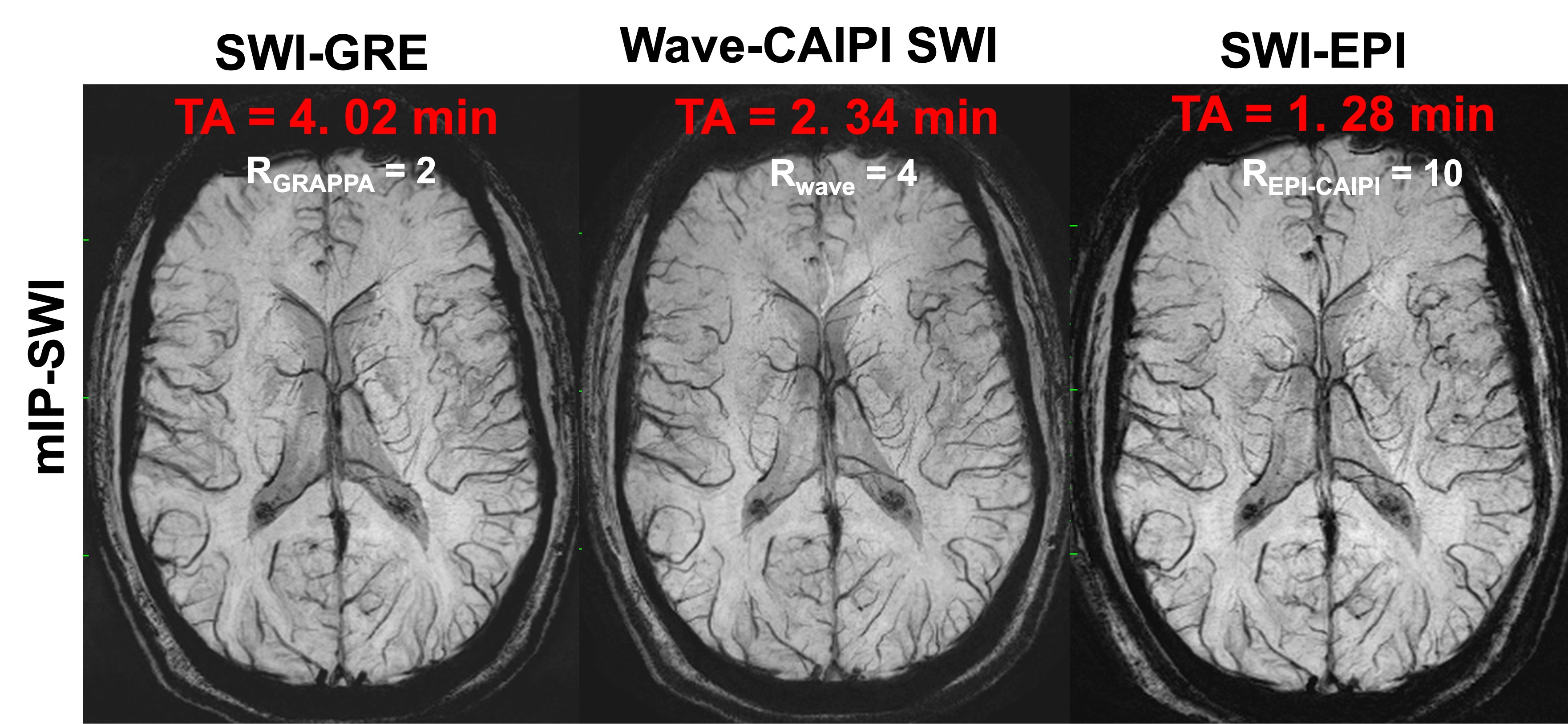
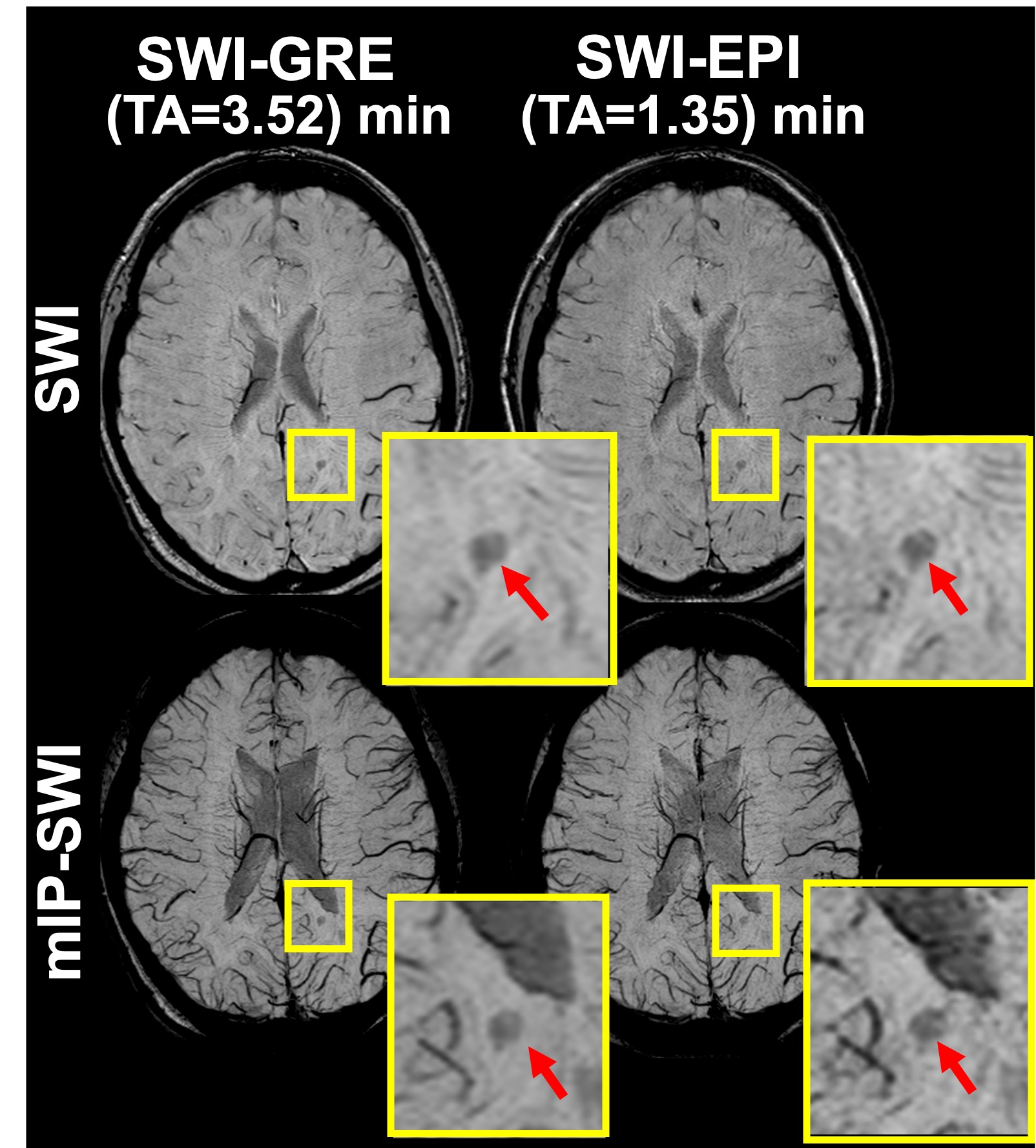
Based on the numerical simulations for SWI-EPI, the difference in signal intensity between WM and veins increased gradually when increasing the EPI-factor (Figure 1 a-b). However, the signal intensity of the CSF showed a marked increase when increasing the EPI-factor (Figure 1 c). To evaluate the optimal FA for each EPI-factor, we then varied the FA values from 0 to 90°and measured the signal intensity change between WM and vein at different EPI-factors (1, 7 and 11). Maximum signal difference was observed at around 15°- 20° (Figure1 d-f).A head-to-head comparison of SWI-GRE images (TA=3.50 minutes) and SWI-EPI images acquired with different EPI-factors (TA=1.45 min to 1.07 min) showed that the image quality was preserved across all accelerated scans (Figure 2). Note that using an EPI-factor of 15 decreased the acquisition time by 70% and this reduction in acquisition time was achieved without any parallel imaging. As expected from the simulations, the tissue contrast between WM and veins gradually increased with higher EPI-factors, whereas the CSF signal intensity changed from hypointense to isointense. Similarly, the CSF signal intensity changed from hypointense to isointense when decreasing FA and the maximal tissue contrast between WM and veins was observed for FA of 20°.To preserve the tissue contrast and the hypointense CSF on SWI-EPI images, FA was subsequently set to 20° and EPI-factor was kept between 3 and 5. The reduction in EPI-factor was compensated by activating the CAIPIRINHA acceleration and we found that a combination of an EPI-factor of 5 with a CAIPIRINHA acceleration of 1 (PE1) x2 (PE2) with shift of 1 decreased the acquisition time down to ~1 minute while preserving the imagequality (Figure 3). Similar image quality was observed when comparing SWI-EPI acquisition (EPI=5 and RCAIPI=1×2 shift 1, TA=1.28 minutes) with standard SWI-GRE(RGRAPPA=2×1, TA=4.02 minutes) and Wave-CAIPI SWI (RWave=4, TA=2.34 minutes) on the same healthy subject (Figure 4). Finally, SWI-EPI acquired on the MS patient displayed similar hypointense brain lesions as SWI-GRE (Figure 5), demonstrating its equal sensitivity to cerebral pathology while providing a 66% reduction in scan time.Discussions
We demonstrated the feasibility of SWI-EPI which combines the 3D-EPI sequence with CAIPIRINHA acceleration to acquire very rapidly SWI images at 3T with similar image quality and contrast to state-of-the-art clinical SWI protocols (SWI-GRE and wave-CAIPI SWI). The two acceleration parameters (EPI-factor and CAIPIRINHA acceleration) offer great flexibility for achieving significant reduction in scan time while providing similar image quality and detection sensitivity toward cerebral vasculature and pathology.Conclusions
This study demonstrated the feasibility of acquiring ultra-fast susceptibility weighted imaging using a combination of 3D-EPI and CAIPIRINHA at 3T. Future studies will investigate the added clinical value of our SWI-EPI approach for the evaluation of neurological disorders.Acknowledgements
We acknowledge the National MS Society (NMSS) RG-2110-38526, National Institutes of Neurological Disorder and Stroke (NINDS) 1U01NS116776-01, and Department of Defense, and Erwin Rautenberg Foundation for research support.References
1. Haacke EM, Mittal S, Wu Z, Neelavalli J, Cheng Y-C. Susceptibility-weighted imaging: technical aspects and clinical applications, part 1. American Journal of Neuroradiology. 2009;30(1):19-30.
2. Mittal S, Wu Z, Neelavalli J, Haacke EM. Susceptibility-weighted imaging: technical aspects and clinical applications, part 2. American Journal of neuroradiology. 2009;30(2):232-52.
3. Haacke EM, Xu Y, Cheng YCN, Reichenbach JR. Susceptibility weighted imaging (SWI). Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2004;52(3):612-8.
4. Duyn JH, Schenck J. Contributions to magnetic susceptibility of brain tissue. NMR in Biomedicine. 2017;30(4):e3546.
5. Chung MS, Lee EJ, Kim S, Kim S-O, Byun JS. Wave-CAIPI susceptibility-weighted imaging achieves diagnostic performance comparable to conventional susceptibility-weighted imaging in half the scan time. European Radiology. 2020;30:2182-90.
6. Sati P, Patil S, Inati S, Wang W-T, Derbyshire JA, Krueger G, Reich DS, Butman JA. Rapid MR susceptibility imaging of the brain using segmented 3D echo-planar imaging (3D EPI) and its clinical applications. Magnetom Flash. 2017;68:26-32.
7. Breuer FA, Blaimer M, Mueller MF, Seiberlich N, Heidemann RM, Griswold MA, Jakob PM. Controlled aliasing in volumetric parallel imaging (2D CAIPIRINHA). Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2006;55(3):549-56.
8. Condon B, Patterson J, Jenkins A, Wyper D, Hadley D, Grant R, Rowan J, Teasdale G. MR relaxation times of cerebrospinal fluid. Journal of computer assisted tomography. 1987;11(2):203-7.
9. Zhao JM, Clingman CS, Närväinen MJ, Kauppinen RA, Van Zijl PC. Oxygenation and hematocrit dependence of transverse relaxation rates of blood at 3T. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2007;58(3):592-7.
10. Wansapura JP, Holland SK, Dunn RS, Ball Jr WS. NMR relaxation times in the human brain at 3.0 tesla. Journal of Magnetic Resonance Imaging: An Official Journal of the International Society for Magnetic Resonance in Medicine. 1999;9(4):531-8.
Figures