3235
Contactless Cardiac Triggering Using Camera PPG in Cardiac MR1Research Laboratories Hamburg, Philips GmbH Innovative Technologies, Hamburg, Germany, 2Philips Healthcare, Hamburg, Germany, 3Digital Standardization & Licensing Research, Philips, Eindhoven, Netherlands, 4Philips Healthcare, Best, Netherlands
Synopsis
Keywords: Data Acquisition, Heart, cardiac triggering
Motivation: Contactless cardiac triggering makes cardiac and cardiovascular MRI (cMRI) more accessible by improving patient comfort, reducing complexity, facilitating swift workflow, and increasing patient throughput.
Goal(s): In this work we demonstrate feasibility of contactless cardiac trigger detection using an in-bore camera in two routine cMRI sequences.
Approach: Building on an existing in-bore camera hardware we developed a cardiac trigger detection method for cMRI that extracts a remote photoplethysmography (rPPG) signal acquired at the patient’s forehead. The quality of the acquired MR images is compared with ECG triggering.
Results: rPPG and ECG triggering delivered comparable image quality in the majority of study volunteers.
Impact: The presented work provides evidence that cMRI is feasible with contactless, camera-based cardiac signal detection. The proposed method allows cMRI without placement of ECG electrodes, thus increasing accessibility of cardiac MR.
Introduction
In current clinical routine cardiac MR (cMR) imaging the cardiac synchronization is typically performed by repeated triggering of the data acquisition based on the R-peak of the Electrocardiogram (ECG). Though being the standard method, a few complications are associated with use of the ECG. The application of ECG patches requires expertise of skilled staff, and it increases the exam time lowering patient throughput. Patients need to be touched which increases risk of infection and many must be shaved which lowers patient comfort. Technically the ECG signal may be perturbed by the magneto-hemodynamic effect and gradient and RF fields.We present an alternative cardiac phase detection and trigger method which uses a video stream from an in-bore camera to derive a remote photoplethysmogram (rPPG). This contactless method greatly facilitates patient comfort and operator workflow. rPPG does not require placement of measurement devices like the fingertip sensor used for contact PPG measurements.
Methods
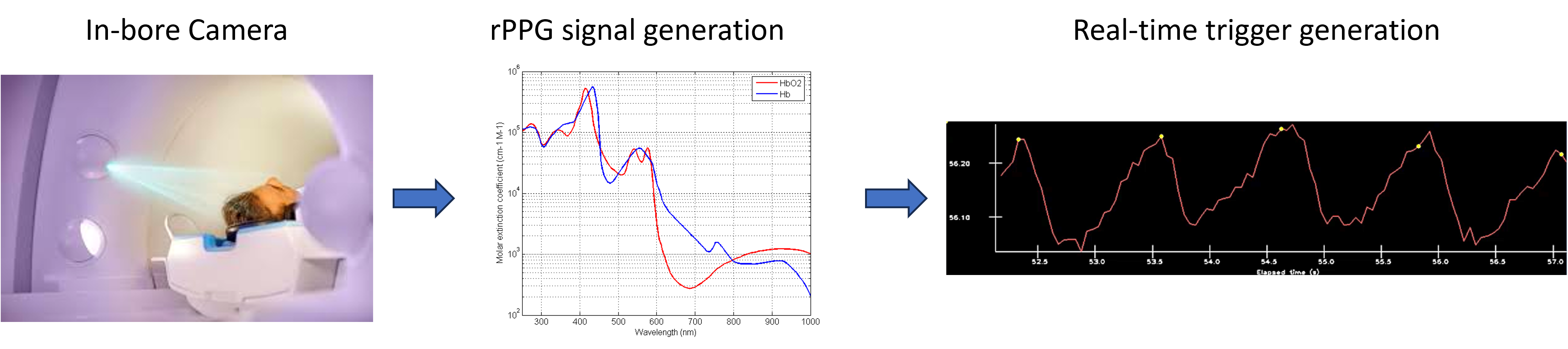
All data was acquired on a clinical MR system (Ingenia Evolution 1.5T, Philips Healthcare, The Netherlands). The product is equipped with an in-bore camera which provides contactless respiration detection and gating. In addition, the video stream from this camera was analyzed in real-time to derive a PPG signal and cardiac triggers to steer the MR acquisition and provide information for reconstruction.The rPPG signal was extracted from the video stream in a multi-step process. First skin pixels are selected based on the pulsatility in the cardiac frequency band [Wang2017]. The raw PPG signal is then computed as the spatial average over all skin-pixels. The raw signal is post-processed by a band-pass filter, to reduce components below the typical cardiac frequencies and high frequent noise. The maxima in this PPG curve are caused by minima of skin blood concentration representing the arrival of the oxygenated blood after systole. Triggers are hence generated at these PPG signal maxima [Wang2022].
Such rPPG triggers derived from the forehead are subject to a physiological delay due to the blood pulse transit time from the heart to the skin. This delay must be considered in prospective triggering as for 3D whole heart (3DWH) imaging.
MR images were acquired in 8 healthy volunteers using CINE (retrospective cardiac-triggered balanced SSFP in breath-hold, TR/TE 3.1/1.56ms, 45ms acquisition/31ms reconstruction per heart phase, acquisition voxel size 1.7 x 1.7 x 8mm³) and 3D whole-heart (3DWH) sequences (respiratory-gated balanced SSFP, diastolic acquisition in 119ms, TR/TE 4.2/2.1ms, acquisition voxel size 1.5mm isotropic). Each sequence was executed twice to compare rPPG and ECG for retrospective and prospective triggering. CINE results were used to determine the resting phase in mid diastole relative to the respective trigger type, and the acquisition delays for 3DWH imaging were set accordingly. Image quality of rPPG triggering was assessed by comparison to ECG baseline.
Results
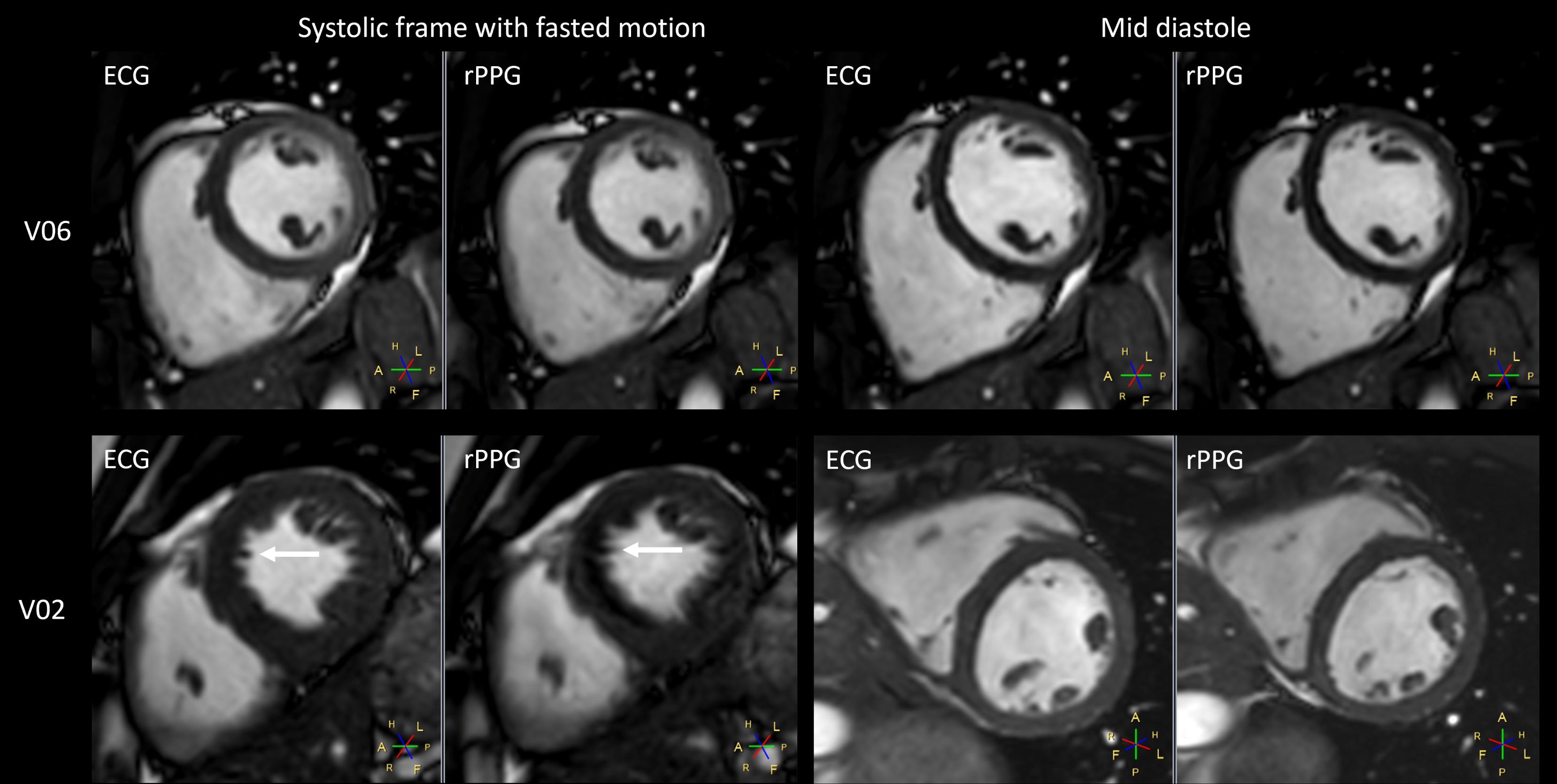
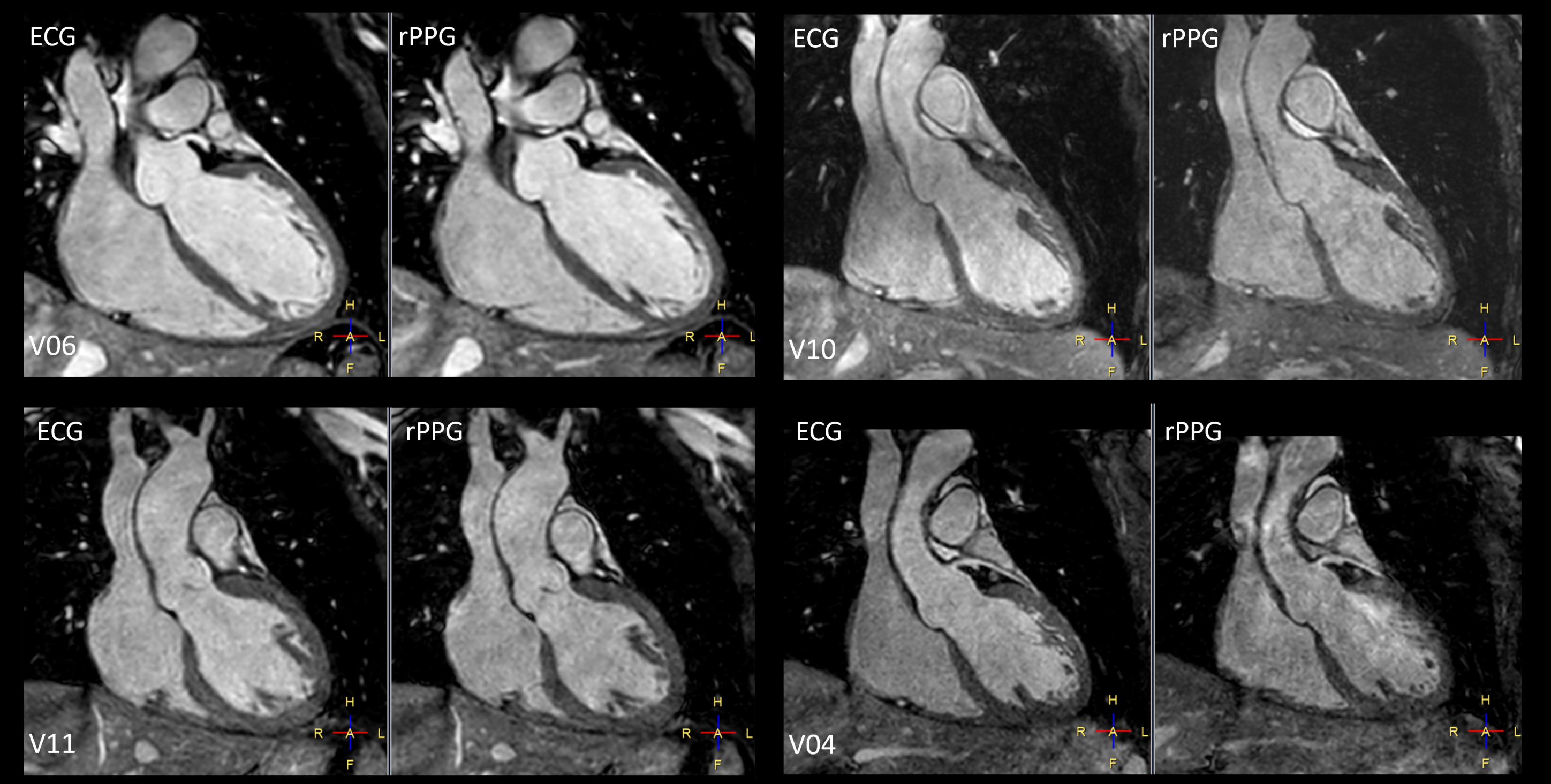
Image quality of CINE images was comparable for both trigger methods for all volunteers (c.f. figure 3). However, the delineation of fast moving structures was affected by some blurring in 3 of 8 subjects as shown in the example of the septal wall in volunteer V02.In 6 of 8 subjects the rPPG triggered 3DWH image quality was comparable to ECG triggering. For both trigger types similar delineations of anatomical structures, coronaries, and valves were obtained (c.f. figure 4).
Discussion
CINE imaging uses retrospective trigger information which requires high temporal accuracy of the trigger detection to represent the cardiac cycle length. The rPPG trigger performs well at this task as can be seen in the good image quality of the rPPG triggered images. The 3D whole heart sequences use a prospective triggering method to steer the MR data acquisition and acquire data during diastole. The rPPG approach reuses the camera and system hardware as already used on clinical scanners for respiratory phase detection and prospective and retrospective gating and triggering (VitalEye in Ingenia Evolution 1.5T, [Harder2019]). It hence complements this method now enabling fully contactless physiological gating and triggering principally applicable to any MR sequence. Further work is required to assess feasibility and implications on image quality of the rPPG approach in broad patient cohort, for complete cMRI exams and other applications.Conclusion
Camera-based rPPG triggering of cardiac CINE and 3DWH imaging is feasible and can deliver comparable image quality to ECG. Even though rPPG trigger has different temporal characteristics than ECG trigger, acquired MR image qualities of the studied volunteer cohort are comparable. If these results can be reproduced clinically and for further scan types, it will greatly simplify patient preparation and increase throughput.Acknowledgements
No acknowledgement found.References
[Wang2017] W. Wang, S. Stuijk, and G. de Haan, “Living-skin classification via remote-ppg,” IEEE Transactions on biomedical engineering, vol. 64, no. 12, pp. 2781–2792, 2017.
Harder2019] F. Harder et al., “Camera-based respiratory triggering improves the image quality of 3D magnetic resonance cholangiopancreatography”, European Journal of Radiology, vol. 120, 108675, 2019.
[Wang2022] W. Wang et al., "Fundamentals of Camera-PPG Based Magnetic Resonance Imaging," in IEEE Journal of Biomedical and Health Informatics, vol. 26, no. 9, pp. 4378-4389, Sept. 2022.
Figures