3230
Investigating ASL-MRI as a Complementary Modality for 18F-FDG PET in Identifying Mesial Temporal Lobe Epilepsy Laterality in Grey Matter1Research Center for Molecular and Cellular Imaging, Tehran University of Medical Sciences, Tehran, Iran (Islamic Republic of), 2Biomedical Engineering and Medical Physics, Shahid Beheshti University of Medical Sciences, Tehran, Iran (Islamic Republic of), 3Bioinformatics and Biophysics, Tarbiat Modares University, Tehran, Iran (Islamic Republic of), 4Medical School, Tehran University of Medical Sciences, Tehran, Iran (Islamic Republic of), 5Pars Advanced and Minimally Invasive Medical Manners Research Center, Pars Hospital, Iran University of Medical Sciences, Tehran, Iran (Islamic Republic of), 6Isfahan Neuroscience Research Center, Isfahan University of Medical Sciences, Isfahan, Iran (Islamic Republic of)
Synopsis
Keywords: Epilepsy, Perfusion, ASL-MRI, 18F-FDG PET, Lateralization of TLE
Motivation: Using non-invasive ASL-MRI as a substitute of 18F-FDG PET for identification of epileptogenic zone in mTLE patients
Goal(s): This study aims to check if there is a correlation between the CBF of ASL-MRI and metabolic data from 18F-FDG PET.
Approach: Brain division into 12 ROIs, including key areas like the amygdala and hippocampus, used BASIL and FSL tools for CBF and SUVr extraction. Used Pearson's and Spearman's rank correlation of SPSS for correlation analysis.
Results: Significant CBF and SUVr correlations in middle temporal gyrus, hippocampus, and superior temporal found in mTLE patients.
Impact: This study affects mTLE patients' accurate and rapid epileptogenic foci location.
Introduction
Nearly 1% of the global population has epilepsy, which causes disability, illness, and mortality [1]. Mesial temporal lobe epilepsy (mTLE) is the most common type of epilepsy in adults, and 30% of patients require surgery since regular anti-seizure drugs don't work [2]. Pre-surgical assessment for mTLE patients during the interictal phase typically relies on 18F-FDG PET, but it has some notable limitations [3]. On the other hand, ASL-MRI is gaining recognition as a valuable method for quantifying cerebral blood flow (CBF) and potentially determining lateralization in mTLE [4, 5]. This study examines whether 18F-FDG PET metabolic data and ASL MRI cerebral blood flow (CBF) maps are correlated in mTLE patients.Methods
Data were rigorously collected from 22 mesial temporal lobe epilepsy (mTLE) patients, 14 men and 8 females, with 10 left and 12 right instances. 52 pairs of label/control ASL images were obtained at Iran's National Brain Mapping Laboratory (NMBL) using the following scanning parameters: post-label delay time of 1,800ms, bolus duration of 700ms, TR of 4100ms, TE of 22ms, field of view (FOV) of 225 × 225 mm², and slice thickness of 4 mm. Additionally, 18F-FDG -PET was performed on all 22 patients utilizing a 64-slice, time of flight General Electric DISCOVERY 690 PET/CT scanner at Iran's Ferdous PET CT Scan center. The Bayesian Inference for Arterial Spin Labeling MRI (BASIL) toolbox, an advanced automated toolkit for CBF mapping pre- and post-processing, was used to handle and analyze PASL-MRI data [6]. Steps in the analysis procedure: FSL's FMRIB's Linear Image Registration (MCFLIRT) applied motion correction to ASL and PET images. Motion-corrected data were smoothed with a 5 FWHM filter to improve signal-to-noise ratio. Smoothed data were registered to MNI space using FSL tools FLIRT and FNIRT. Standardized uptake value ratio (PET) and CBF (ASL-MRI) were created and normalized to the cerebellum mean values in MNI space [7-9]. Division of the brain into left and right hemispheres yielded 12 ROIs. The amygdala, hippocampus, parahippocampal, inferior temporal gyrus, middle temporal, and superior temporal gyri were also bilaterally extracted using Wake Forest University (WFU) Pick atlas toolbox and SPM 12 tools in MATLAB 9.10.0 R2021a on Windows 10 [10]. Mean ROI values were used to calculate a perfusion asymmetry index using the AI equation (Figure 1). SPSS 26.0 was used for statistical analysis. Data normality was tested using the Shapiro-Wilk test. If SUVr and CBF in ROIs were normally distributed, Pearson's correlation was utilized for correlation analysis; otherwise, Spearman's rank correlation was used. The significance level for statistical findings was 0.05.Result
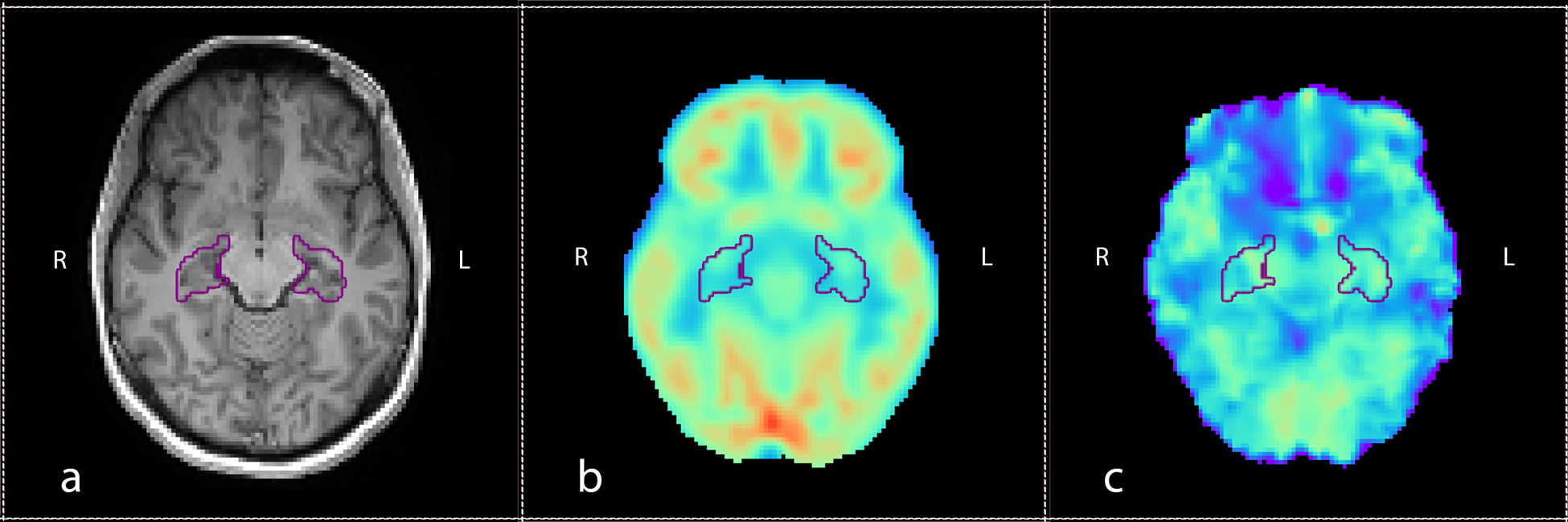
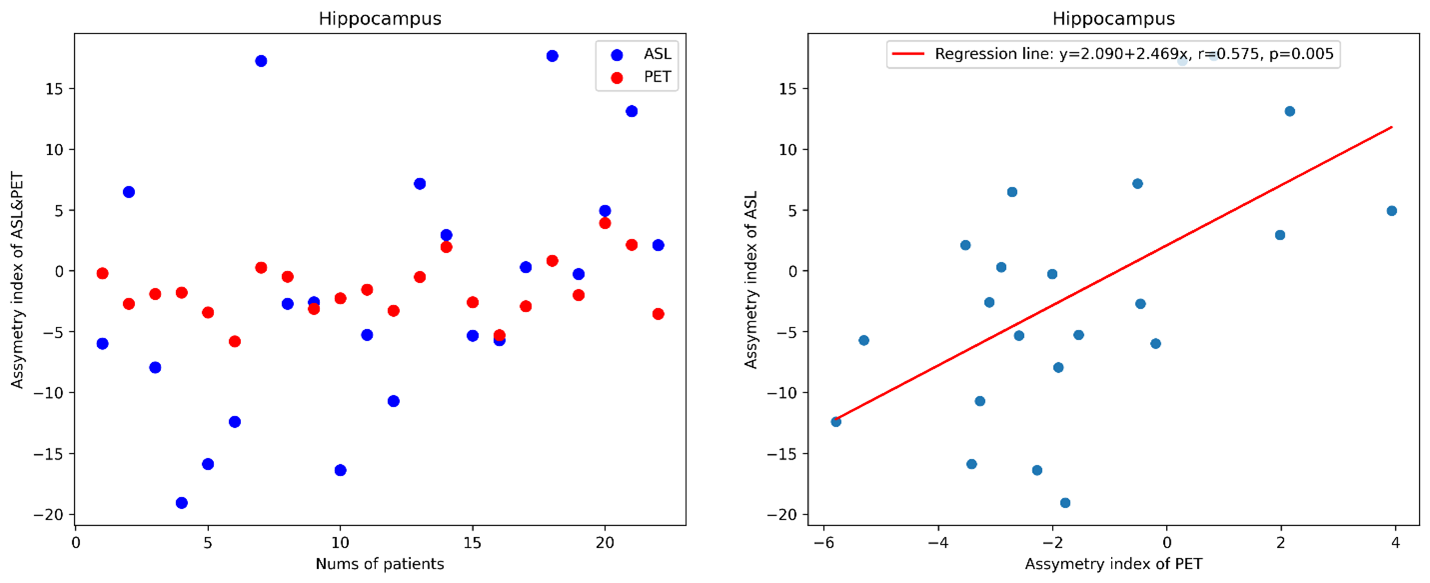
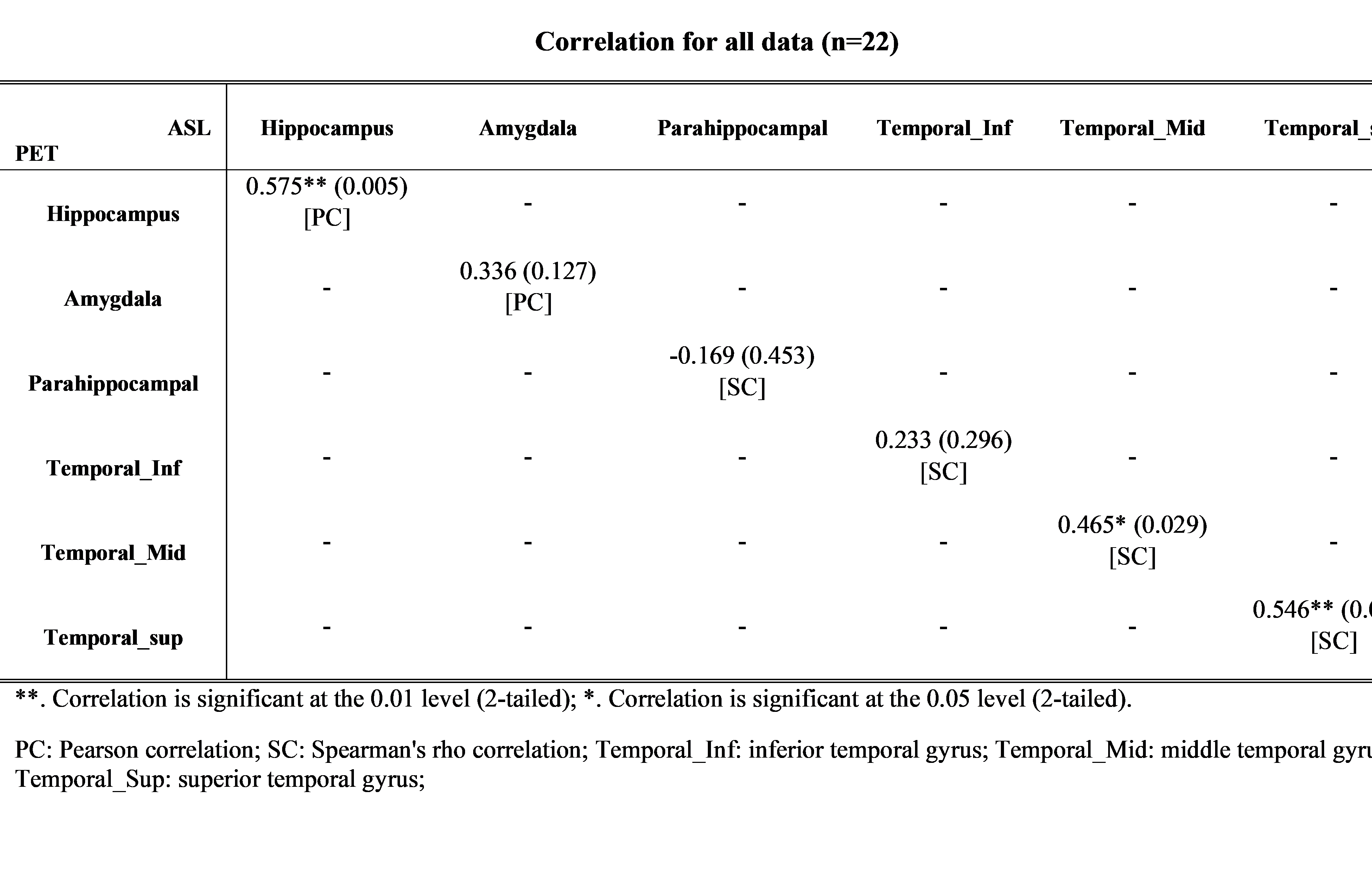
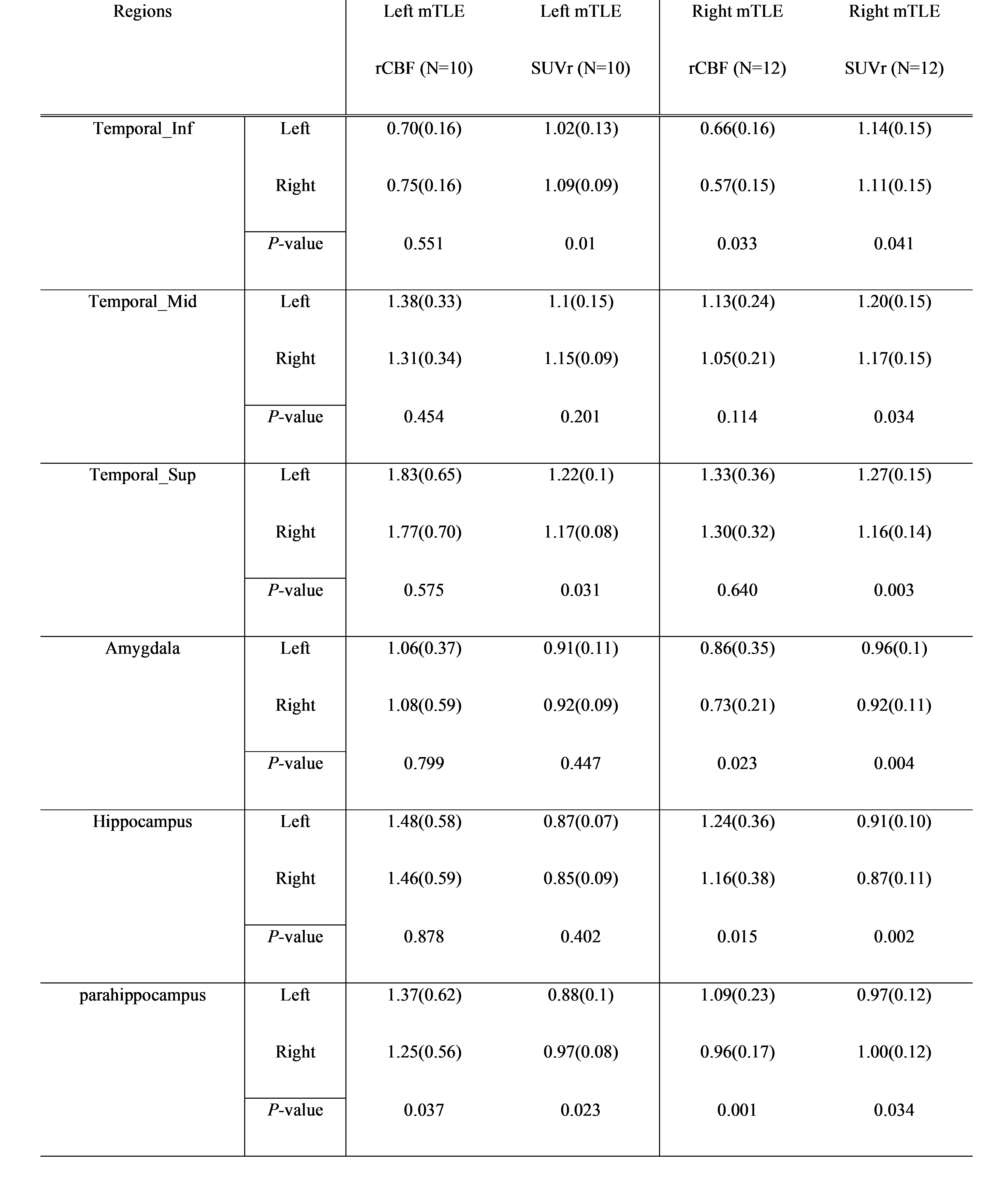
Table 1 shows that CBF and SUVr AI correlated in middle temporal gyrus (r= 0.465, P = 0.029), hippocampus (r= 0.575, P = 0.005), and superior temporal (r= 0.546, P = 0.009). A right mTLE patients had hypoperfusion and hypometabolism in the hippocampus (Figure 2). Figure 3 illustrates the hippocampus's PET and ASL AI values and correlation. Table 2 shows significant intra-group differences in right mTLE rCBF at inferior temporal gyrus, amygdala, hippocampus, and parahippocampus, and SUVr in all regions. For left mTLE, SUVr differed between bilateral regions in parahipocampus, superior temporal gyrus, and inferior temporal gyrus. Only parahippocampus showed a significant difference for rCBF.Discussion
For effective surgery in mTLE patients, precise lateralization and preoperative assessment require multimodal imaging [11]. Although PET hypometabolism has improved lateralization in mTLE patients, there is a preference to reduce radioactive tracer-based imaging. These imaging modalities are scarce and expensive, making practicality difficult. Wolf et al. [12] used continuous ASL-MRI and 18F-FDG PET imaging in 12 mTLE patients. A substantial correlation was found between AI measures from both imaging modalities for important mesial temporal structures like the amygdala, hippocampus, parahippocampus, and uncus. Another study used 18F-FDG PET and pseudo-continuous ASL to image 12 mTLE patients [13]. The AI correlation between both modalities indicated a strong hippocampal correlation. We also identified a substantial connection between 18F-FDG PET and ASL CBF in the hippocampus. In epilepsy studies, the lateral temporal region (the inferior, middle, and superior temporal gyri) is crucial to mTLE [14-16]. ASL and PET data in the superior and middle temporal gyri correlated well in our investigation. Given this region's importance in lateralization, this hypometabolism-hyperperfusion conjunction is significant.Acknowledgements
No acknowledgement found.References
1. Perucca P, Scheffer IE, Kiley M: The management of epilepsy in children and adults. Med J Aust 2018, 208(5):226-233.
2. Sisodiya SM, Whelan CD, Hatton SN, Huynh K, Altmann A, Ryten M, Vezzani A, Caligiuri ME, Labate A, Gambardella A et al: The ENIGMA-Epilepsy working group: Mapping disease from large data sets. Hum Brain Mapp 2020, 43(1):113-128.
3. Sone D, Maikusa N, Sato N, Kimura Y, Ota M, Matsuda H: Similar and Differing Distributions Between (18)F-FDG-PET and Arterial Spin Labeling Imaging in Temporal Lobe Epilepsy. Front Neurol 2019, 10:318.
4. Rahimzadeh H, Kamkar H, Hoseini-Tabatabaei N, Mobarakeh NM, Habibabadi JM, Hashemi-Fesharaki SS, Nazem-Zadeh MR: Alteration of intracranial blood perfusion in temporal lobe epilepsy, an arterial spin labeling study. Heliyon 2023, 9(4):e14854.
5. Fan AP, Khalighi MM, Guo J, Ishii Y, Rosenberg J, Wardak M, Park JH, Shen B, Holley D, Gandhi H: Identifying hypoperfusion in moyamoya disease with arterial spin labeling and an [15O]-water positron emission tomography/magnetic resonance imaging normative database. Stroke 2019, 50(2):373-380.
6. Chappell MA, Groves AR, Whitcher B, Woolrich MW: Variational Bayesian Inference for a Nonlinear Forward Model. IEEE Transactions on Signal Processing 2009, 57(1):223-236.
7. Kojan M, Gajdos M, Riha P, Dolezalova I, Rehak Z, Rektor I: Arterial Spin Labeling is a Useful MRI Method for Presurgical Evaluation in MRI-Negative Focal Epilepsy. Brain Topogr 2021, 34(4):504-510.
8. Verclytte S, Lopes R, Lenfant P, Rollin A, Semah F, Leclerc X, Pasquier F, Delmaire C: Cerebral Hypoperfusion and Hypometabolism Detected by Arterial Spin Labeling MRI and FDG-PET in Early-Onset Alzheimer's Disease. J Neuroimaging 2016, 26(2):207-212.
9. Dolui S, Li Z, Nasrallah IM, Detre JA, Wolk DA: Arterial spin labeling versus (18)F-FDG-PET to identify mild cognitive impairment. Neuroimage Clin 2020, 25:102146.
10. Maldjian JA, Laurienti PJ, Kraft RA, Burdette JH: An automated method for neuroanatomic and cytoarchitectonic atlas-based interrogation of fMRI data sets. Neuroimage 2003, 19(3):1233-1239.
11. Nazem-Zadeh MR, Elisevich KV, Schwalb JM, Bagher-Ebadian H, Mahmoudi F, Soltanian-Zadeh H: Lateralization of temporal lobe epilepsy by multimodal multinomial hippocampal response-driven models. J Neurol Sci 2014, 347(1-2):107-118.
12. Wolf RL, Alsop DC, Levy-Reis I, Meyer PT, Maldjian JA, Gonzalez-Atavales J, French JA, Alavi A, Detre JA: Detection of mesial temporal lobe hypoperfusion in patients with temporal lobe epilepsy by use of arterial spin labeled perfusion MR imaging. AJNR Am J Neuroradiol 2001, 22(7):1334-1341.
13. Wang YH, An Y, Fan XT, Lu J, Ren LK, Wei PH, Cui BX, Du JL, Lu C, Wang D et al: Comparison between simultaneously acquired arterial spin labeling and (18)F-FDG PET in mesial temporal lobe epilepsy assisted by a PET/MR system and SEEG. Neuroimage Clin 2018, 19:824-830.
14. Lim YM, Cho YW, Shamim S, Solomon J, Birn R, Luh WM, Gaillard WD, Ritzl EK, Theodore WH: Usefulness of pulsed arterial spin labeling MR imaging in mesial temporal lobe epilepsy. Epilepsy Res 2008, 82(2-3):183-189.
15. Guo X, Xu S, Wang G, Zhang Y, Guo L, Zhao B: Asymmetry of cerebral blood flow measured with three-dimensional pseudocontinuous arterial spin-labeling mr imaging in temporal lobe epilepsy with and without mesial temporal sclerosis. J Magn Reson Imaging 2015, 42(5):1386-1397.
16. Nelissen N, Van Paesschen W, Baete K, Van Laere K, Palmini A, Van Billoen H, Dupont P: Correlations of interictal FDG-PET metabolism and ictal SPECT perfusion changes in human temporal lobe epilepsy with hippocampal sclerosis. Neuroimage 2006, 32(2):684-695.
Figures