3227
Personalized characterization of corpus-callosum pathology in mesial temporal lobe epilepsy using quantitative brain relaxation atlases1Neuroscience Research Center, Department of Medical and Surgical Sciences, University Magna Graecia, Catanzaro, Italy, Catanzaro, Italy, 2Advanced Clinical Imaging Technology, Siemens Healthineers International AG, Lausanne, Switzerland, 3CIBM Center for Biomedical Imaging, Geneva, Switzerland, 4Institute of Neurology, Department of Medical and Surgical Sciences, University Magna Graecia, Catanzaro, Italy, Catanzaro, Italy, 5Siemens Healthcare srl, Milano, Italy, 6Department of Radiology, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland, 7LTS5, École Polytechnique Fédérale de Lausanne (EPFL), Lausanne, Switzerland
Synopsis
Keywords: Epilepsy, Quantitative Imaging, T1 relaxometry, T2 relaxometry, corpus callosum
Motivation: Investigate callosal integrity in mesial temporal lobe epilepsy (MTLE) using quantitative MRI.
Goal(s): This study aims to investigate the distribution of quantitative T1 and T2 alterations in terms of z-scores in the midsagittal profile of the corpus callosum (CC) in patients with MTLE.
Approach: MP2RAGE sequence for T1 relaxometry and GRAPPATINI for T2 relaxometry were acquired on 9 MTLE patients and the midsagittal distribution of z-scores was investigated.
Results: Callosal alterations in MTLE were located in regions crossed by temporal and frontal fibers. Our findings support the hypothesis that MTLE-related pathophysiological changes extend beyond the temporal lobe and involve various cortical regions.
Impact: This study provides first evidence of qMRI alterations in the corpus callosum of patients with temporal lobe epilepsy. Despite the focal nature of the syndrome, deviations from the norm included fibers connecting temporal and extratemporal cortices.
Introduction
Recently, normative atlases for T1 and T2 relaxation times have been proposed for individualized quantification of brain tissue abnormalities1. In mesial temporal lobe epilepsy (MTLE), the most common form of epilepsy in adulthood, a large body of evidence suggests that MTLE-related pathophysiological changes may extend beyond the temporal lobe, through cortico-cortical and cortico-subcortical networks2. The corpus callosum (CC) might serve as an optimal window to investigate the integrity of different cortical regions, and evidence suggests its involvement in MTLE3.In this study, we described the distribution of quantitative T1 and T2 alterations in the midsagittal profile of the CC, at individual level and without a priori subdivisions of the bundle, in patients with MTLE characterized by different degrees of drug-responsiveness.Methods
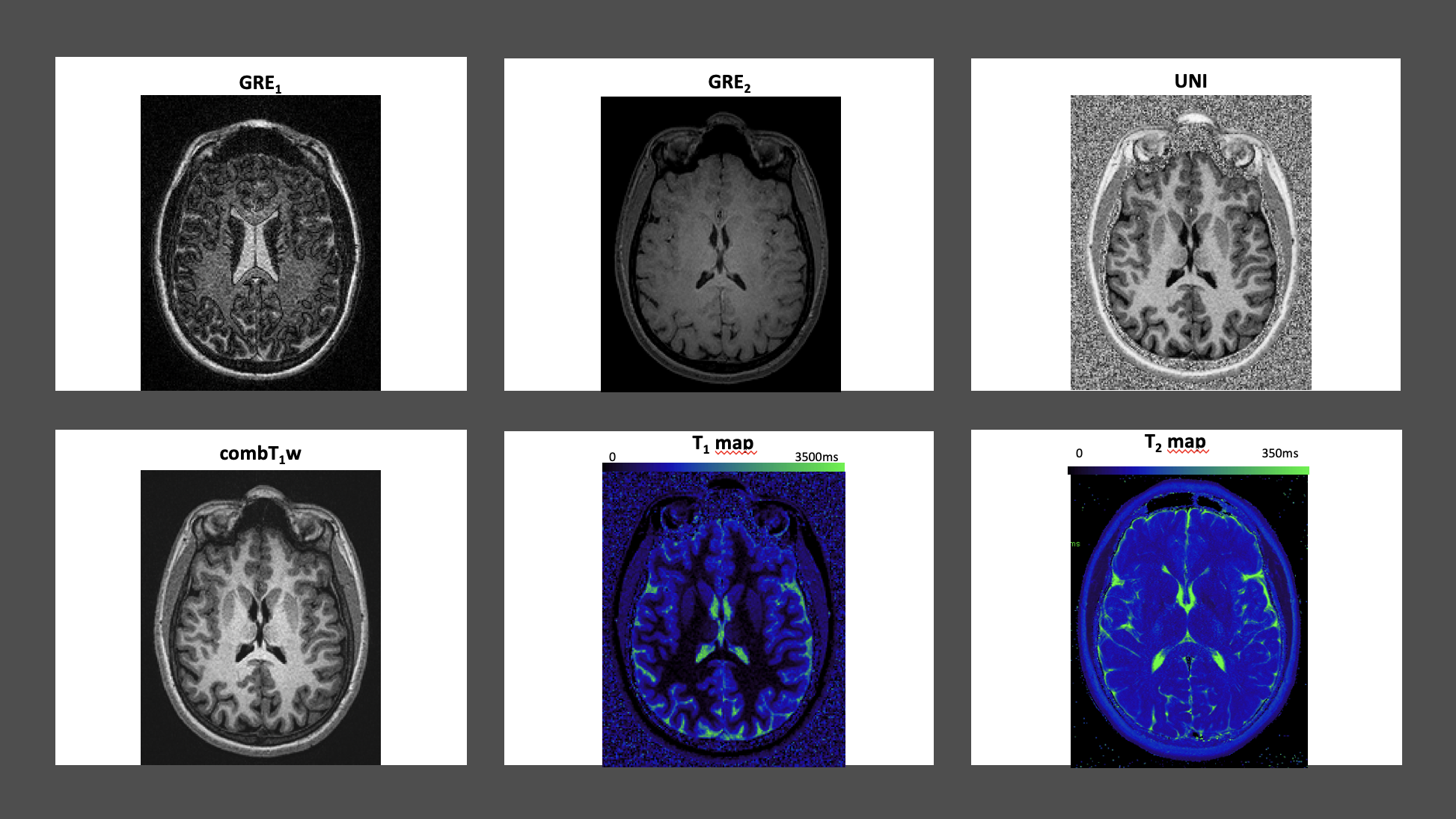
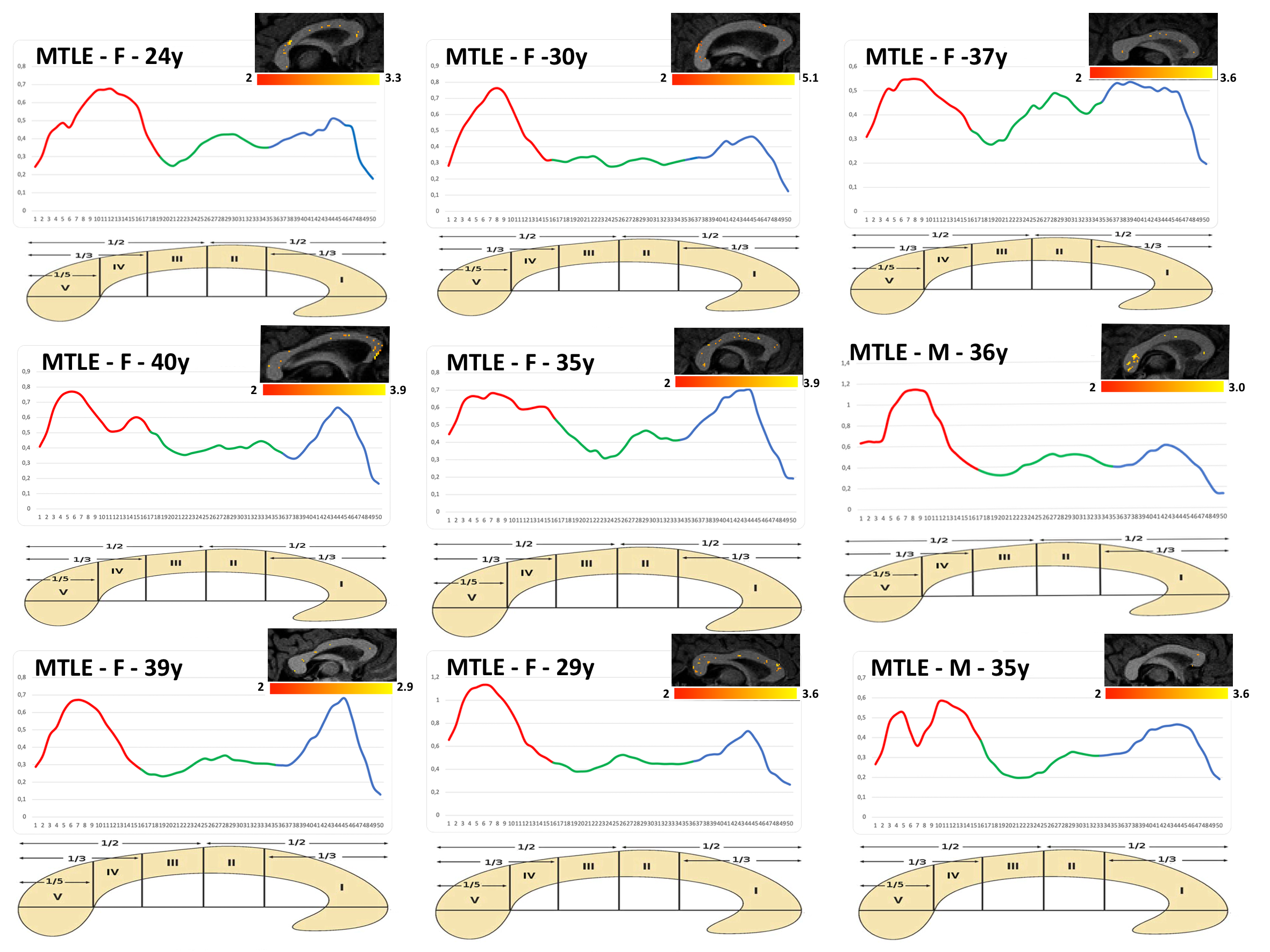
Nine patients (7 females; age: 33.9 ± 5.1) with mesial temporal lobe epilepsy (MTLE) underwent 3T MRI (Biograph mMR, Siemens Healthcare, Erlangen, Germany) using a 16-channel PET-transparent head/neck coil. The protocol included an MP2RAGE sequence4 (TI1/TI2/TE/TR=700/2500/2.96/5000 ms; flip angles 4/5 deg; 1 x 1 x 1 mm3; GRAPPAx3; auto-align Head > Basis) for T1 relaxometry and the research application sequence GRAPPATINI for quantitative T2 mapping5 (TR=4s, 10-fold undersampling, 16 echoes, 10.9:174.4ms, spaced by 10.9 ms; Resolution: 0.45 x 0.45 x 4 mm3). In figure 1 are reported images used of a single subject as example. At the time of the MRI exam, 3 out of 9 MTLE patients were not treated with any anti-seizure medications (ASMs), 4 underwent monotherapy, and 2 were under polytherapy (two or more ASMs). Single-subject comparisons of voxel-wise quantitative parameters against age-/sex matched healthy reference values were obtained following Piredda et al1.Briefly, individual T1 and T2 maps were co-registered onto reference atlases established using linear regression models, to consider each patient’s age and sex when calculating deviations from the healthy population1. For each voxel, such deviations were evaluated as z-scores in WM tissues. For the visualization of results, individual z-score maps were registered into native space using the inverse of the transformation onto the atlas space, and subsequently, a threshold was applied to maintain only voxels with more than 2 standard deviations from the corresponding normative population value (i.e., |z| > 2).To focus the analysis on the CC, we applied an automated method to generate 50 equidistant nodes on the midsagittal profile of the tract6,3 from the T1-weighted UNI image. We then extracted the average absolute T1 and T2 z-scores at each node, to obtain distributions of deviations from the reference atlas across the bundle section. Since no a priori subdivision was used for the CC, Witelson’s scheme7 served as a guide to interpret results.Results
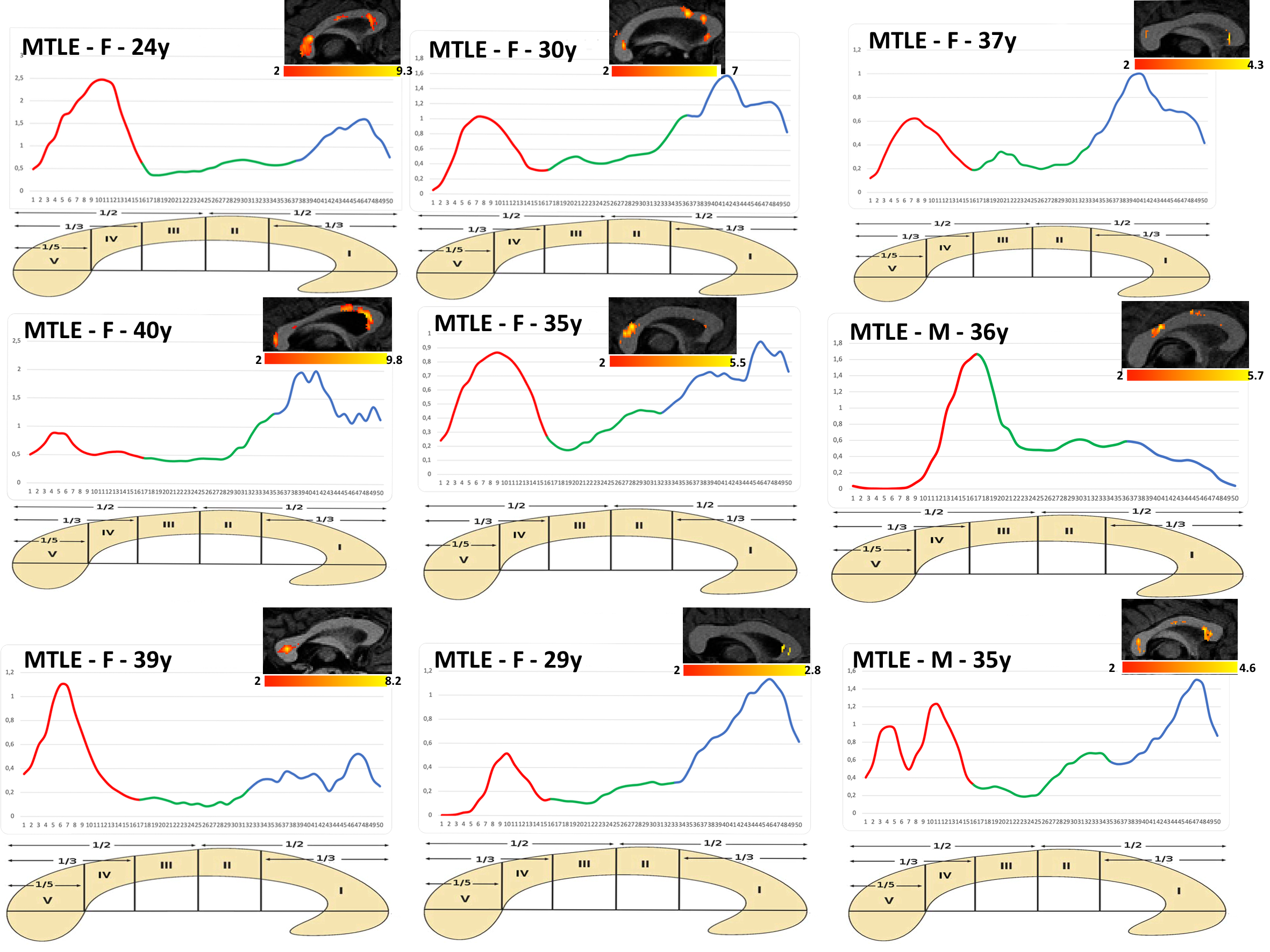
Figure 2 shows the distribution of T1 z-scores across the CC profile. Four out of 9 patients showed alterations limited to posterior regions of CC, in particular in the IV and V quadrants according to Witelson’s scheme (average T1-z-score 0.9). The remaining 5 patients showed instead alterations that encompassed both anterior and posterior regions of the CC (average T1-z-score 0.7). T2 z-scores, as shown in Figure 3, were larger both in terms of cluster size and of absolute z-score (|z| > 2), compared to T1 relaxometry. Two out of 9 MTLE patients showed alterations in the posterior CC region, 4 in anterior the CC region and 3 in both anterior and posterior CC regions.Conclusion
These preliminary results provide evidence that corpus callosum integrity may be hampered in MTLE patients, independently of drug-responsiveness, and with a precise spatial pattern that encompassed, as expected, regions of the CC crossed by temporal fibers, but also the genu of CC, as previously described in drug-resistant MTLE3. Observed deviations of T2 relaxometry seemed more prominent than those observed for T1 values, a finding which deserves further investigation to assess whether different voxel resolution between GRAPPATINI and MP2RAGE may have influenced cluster sizes. Future studies will also focus on understanding how different spatial patterns of deviations from the norm may be associated with individual clinical features of each patient (e.g., seizure semeiology, neuropsychological comorbidities) to monitor clinical status over time.Acknowledgements
Work supported by #NEXTGENERATIONEU (NGEU) and funded by the Ministry of University and Research (MUR), National Recovery and Resilience Plan (NRRP), project MNESYS (PE0000006) – A Multiscale integrated approach to the study of the nervous system in health and disease (DN. 1553 11.10.2022)References
- Piredda GF, Hilbert T, Granziera C, Bonnier G, Meuli R, Molinari F, Thiran JP, Kober T. Quantitative brain relaxation atlases for personalized detection and characterization of brain pathology. Magn Reson Med. 2020;83(1):337-351.
- Larivière S, Rodríguez-Cruces R, Royer J, Caligiuri ME, Gambardella A, Concha L, Keller SS, Cendes F, Yasuda C, Bonilha L, Gleichgerrcht E, Focke NK, Domin M, von Podewills F, Langner S, Rummel C, Wiest R, Martin P, Kotikalapudi R, O'Brien TJ, Sinclair B, Vivash L, Desmond PM, Alhusaini S, Doherty CP, Cavalleri GL, Delanty N, Kälviäinen R, Jackson GD, Kowalczyk M, Mascalchi M, Semmelroch M, Thomas RH, Soltanian-Zadeh H, Davoodi-Bojd E, Zhang J, Lenge M, Guerrini R, Bartolini E, Hamandi K, Foley S, Weber B, Depondt C, Absil J, Carr SJA, Abela E, Richardson MP, Devinsky O, Severino M, Striano P, Tortora D, Hatton SN, Vos SB, Duncan JS, Whelan CD, Thompson PM, Sisodiya SM, Bernasconi A, Labate A, McDonald CR, Bernasconi N, Bernhardt BC. Network-based atrophy modeling in the common epilepsies: A worldwide ENIGMA study. 2020.
- Caligiuri ME, Labate A, Cherubini A, et al. Integrity of the corpus callosum in patients with benign temporal lobe epilepsy. Epilepsia, 2016;57: 590-596.
- Marques JP, Kober T, Krueger G, van der Zwaag W, Van de Moortele PF, Gruetter R. MP2RAGE, a self bias‐field corrected sequence for improved segmentation and T1‐mapping at high field. NeuroImage. 2010;49:1271–1281.
- Hilbert T, Sumpf TJ, Weiland E, et al. Accelerated T2 mapping combining parallel MRI and model‐based reconstruction: GRAPPATINI. J Magn Reson Imaging. 2018;48:359–368.
- Adamson, C., Beare, R., Walterfang, M., Seal, M. (2014), ‘Software pipeline for midsagittal corpus callosum thickness profile processing’, Neuroinformatics, vol. 12, pp. 1–20.
- Witelson, S.F. (1989), ‘Hand and sex differences in the isthmus and genu of the human corpus callosum. A postmortem morphological study’, Brain, vol. 112, no. 3, pp. 799–835.
Figures