3226
Regional cortical thinning and aberrant cortical folding in sleep-related hypermotor epilepsy1Department of Radiology and Huaxi MR Research Center (HMRRC), West China Hospital of Sichuan University, Chengdu, China, 2Department of Neurology, West China Hospital of Sichuan University, Chengdu, China, 3Department of Radiology, The First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou, China, 4Department of Radiology, Huashan Hospital, Fudan University, Shanghai, China, 5Radiology, West China Hospital of Sichuan University, Chengdu, China, 6Department of Radiology, West China Hospital of Sichuan University, Chengdu, China, 7Radiology, West China Xiamen Hospital of Sichuan University, Xiamen, China
Synopsis
Keywords: Epilepsy, Microstructure, Sleep-related hypermotor epilepsy, structural magnetic resonance imaging, surface-based morphometry, cortical thickness, sulcal depth
Motivation: We aimed to investigate the neuromorphometric abnormalities and their relationship with clinical characteristics in patients with sleep-related hypermotor epilepsy (SHE) by structural MRI.
Goal(s): This is the first study to explore cortical microstructural alterations using surface-based morphometry (SBM) analysis in SHE patients.
Approach: SBM analysis was used to evaluate cortical thickness, fractal dimension, gyrification, and sulcal depth.
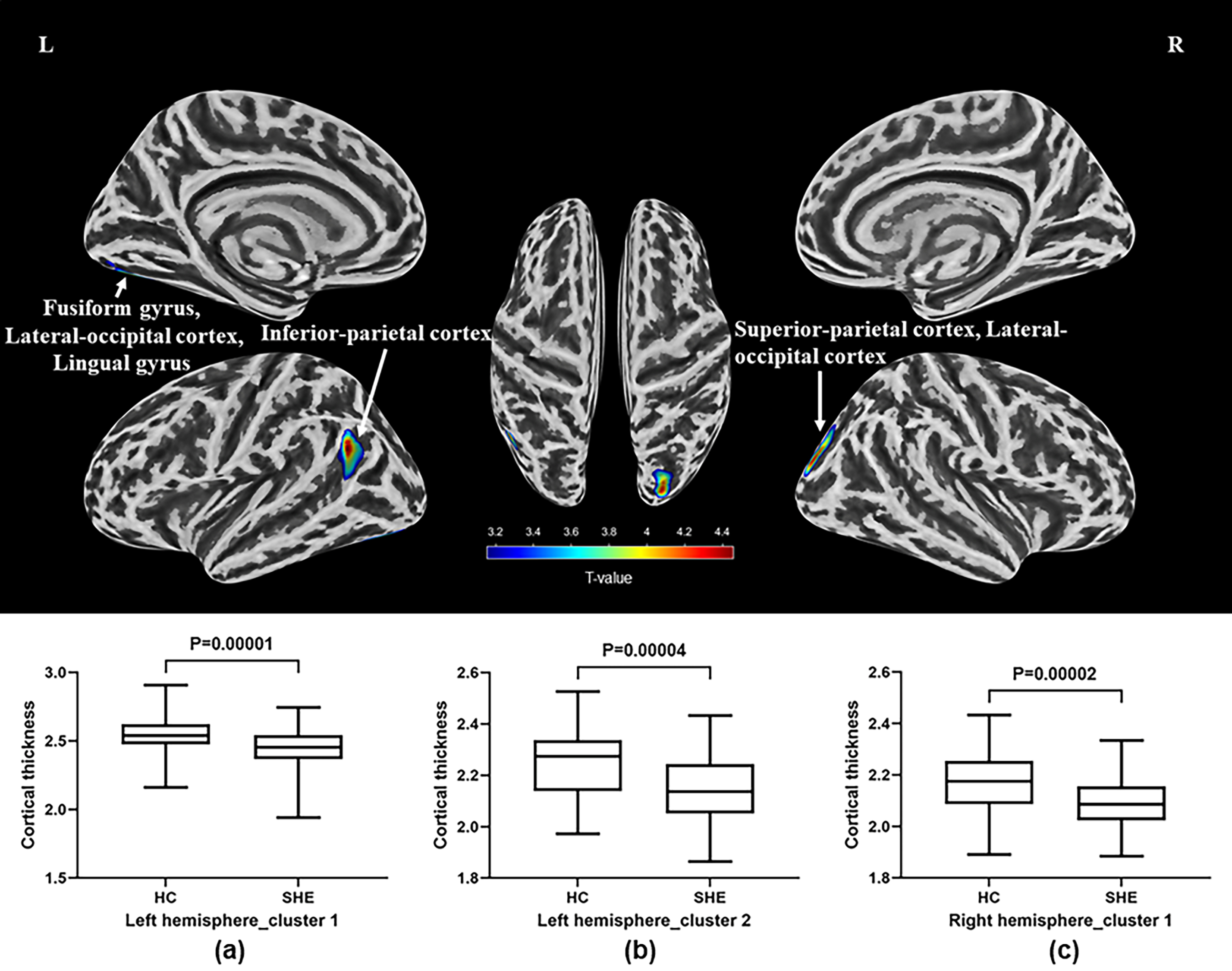
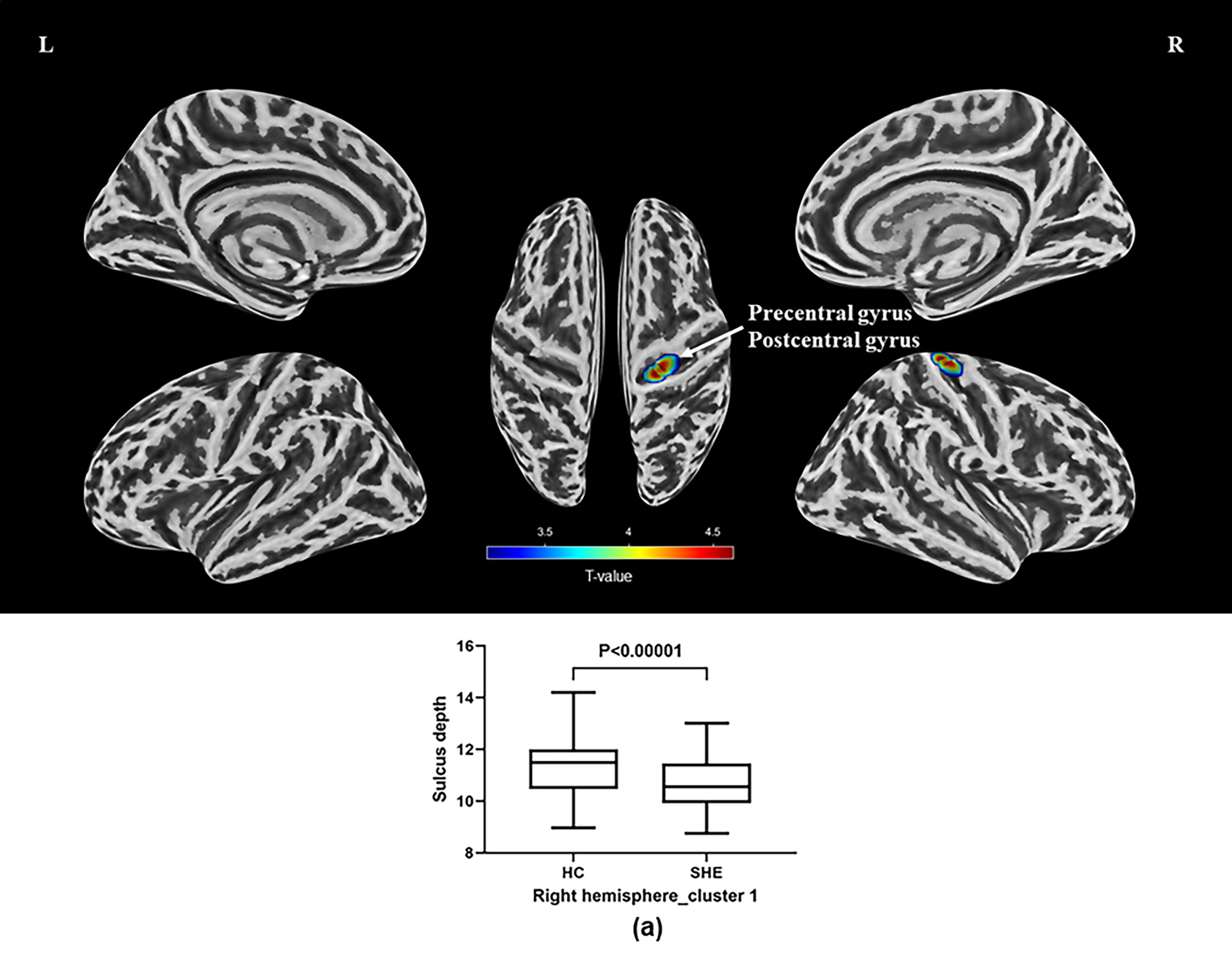
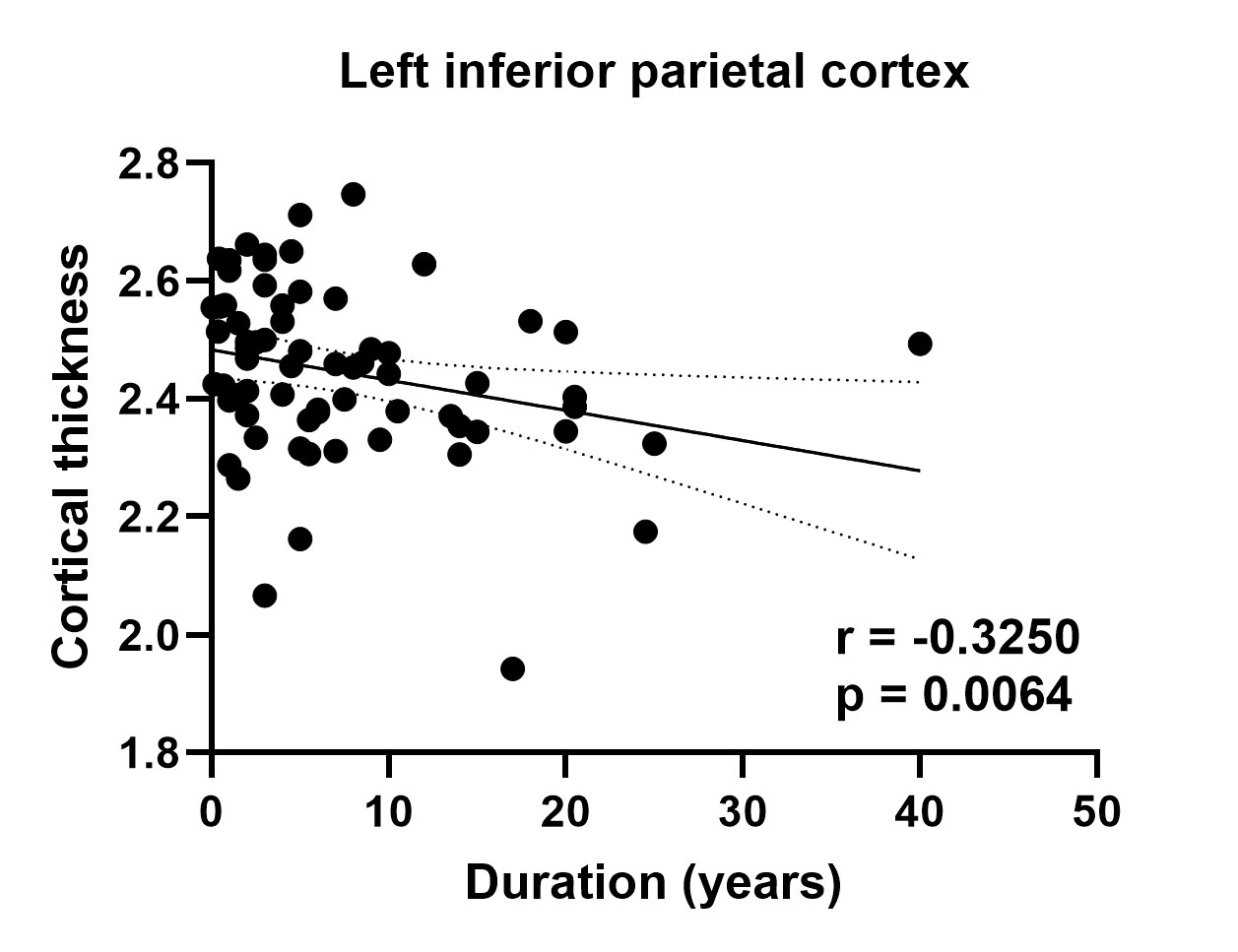
Results: SHE patients exhibited decreased cortical thickness in the left inferior-parietal, right superior-parietal, bilateral lateral-occipital, left fusiform regions, and decreased sulcal depth in the right precentral and postcentral gyri compared to controls. The cortical thickness of left inferior-parietal region was negatively correlated with illness duration.
Impact: These findings demonstrate that aberrated thinning and folding of local cerebral cortices existed in SHE and may be associated with clinical hypermotor semiology. These cortical morphological variations might contribute to understand epilepsy network disturbances and underlying neuropathologic mechanism of SHE.
Introduction
Sleep-related hypermotor epilepsy (SHE), a rare type of focal epilepsy, is characterized by brief and hyperkinetic seizures, predominantly arising during sleep[1, 2]. The majority of SHE patients have normal routine MRI findings and uninformative interictal and ictal electroencephalogram (EEG). The diagnostic criteria of SHE was mainly based on clinical history and seizure semiology[1]. The surface-based morphometry (SBM) analysis has been widely used in epilepsy research to estimate cortical thickness and sulcal depth, characterize the amount of folding, and index brain surface complexity[3]. However, there are no studies using surface-based approaches to explore cortical microstructural variations in SHE, which could help further understand its neuropathophysiological mechanisms.Methods
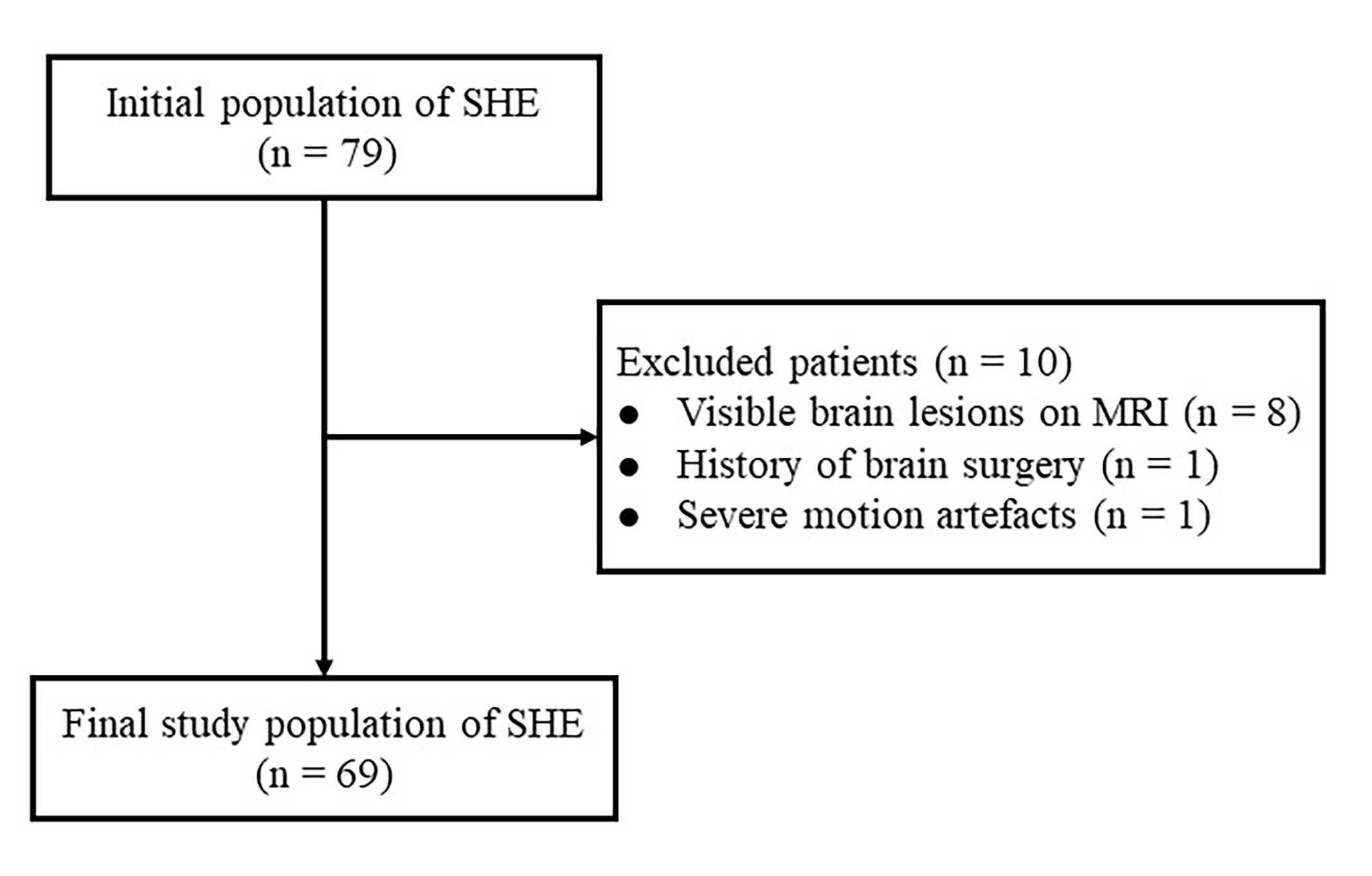
ParticipantsThe study was authorized by the local ethical committee of our hospital. All participants provided written informed consent. 79 patients with sporadic SHE and 69 age- and gender-matched healthy controls (HCs) were prospectively enrolled.
Image acquisition and processing
T1weighted images (T1WIs) were acquired with a Siemens 3.0T MRI scanner (Trio Tim, Erlangen, Germany), using an eight-channel head coil. T1WIs were acquired with a Magnetization Prepared Rapid Gradient Echo (MPRAGE) sequence. The scan parameters were as follows: repetition time/echo time (TR/TE) = 2250/2.6 ms, flip angle = 9°, slice thickness = 1 mm, matrix size = 256 × 256, field of view = 256 × 256 mm2, and acquisition time = 5.43 min. T1WIs were processed using an automated program in the Computational Anatomy Toolbox (CAT12) within SPM12, including two stages: voxel-based processing and surface-based processing[4].
Statistical analysis
The two-sample t-tests were used to between-group comparisons of cortical morphological indices by utilizing age and sex as covariates. Multiple comparisons were conducted by cluster-level family-wised error (FWE) method (p < 0.05).
The two-sample t-test and the Chi-squared test were performed to compare the demographic and clinical data using SPSS 23.0. Pearson or Spearman correlation test was used to assess the association between cortical structural parameters and clinical data.
Results
A total of 69 patients with SHE (mean age = 31.41±11.88 years; male : female = 45:24) and 69 HCs (mean age = 31.51±12.09 years; male : female = 35:34) were prospectively included in this study. Compared with HCs, patients with SHE exhibited significantly decreased cortical thickness in left inferior-parietal, fusiform and lingual, right superior-parietal, and bilateral lateral-occipital cortices (p = 0.00001-0.00004), and shallower sulcus depth in right precentral and postcentral gyri (p < 0.00001). However, no differential brain region was found in between-group comparisons of fractal dimension and gyrification (all P>0.05). Correlation analysis showed a negative correlation between the cortical thickness of left inferior-parietal region and SHE duration (r= -0.325, p=0.0064).Discussion
In this study, we found a bilateral brain atrophy pattern, primarily distributed in the bilateral parietal and occipital, and left fusiform cortices. Previous voxel-based morphometry (VBM) study also reported reduced gray matter volume in the left fusiform and inferior-parietal regions in patients with SHE[5]. Structural MRI studies in temporal lobe epilepsy have demonstrated that cortical thinning potentially result from the seizure-induced damage[6, 7], even in the bilateral and extra-epileptogenic cortical regions[8]. These findings suggest that focal epilepsy may involve brain network dysfunction rather than just impacting epileptogenic zone.The parietal lobe is known to participate in the posterior default-mode network, which is crucial for maintaining consciousness[9]. The microstructural abnormalities in parietal lobule provide a possible explanation for loss of consciousness suffered by SHE patients. The fusiform gyrus has been considered as a key structure for functionally-specialized computations of high-level vision such as face perception and object recognition[10]. The lateral-occipital region belongs to visual cortex. The visual areas of brain were often connected to motor regions for the sensory guidance of movement[11].
Patients with SHE showed decreased sulcus depth in the right precentral and postcentral gyri, which form part of the sensorimotor network (SMN) [12]. A resting-state functional MRI study reported that SHE patients showed higher local intrinsic activity in SMN regions[12]. Involvement of SMN is consistent with the clinical “hypermotor” semiology of SHE. Altered cortical folding could be a structural manifestation of neural network disturbance underlying the seizure. Past study found significantly higher functional connectivity of SMN and thalamus in SHE[13].
We found a negative correlation between epilepsy duration and cortical thickness of left inferior-parietal region. It is possible that the accumulation of microstructural changes or secondarily generalized seizures due to the long-standing nature of disease[14].
Conclusion
SHE-related alterations of cortical thickness and sulcus depth in some cerebral regions may provide a direction for further uncovering the neuropathological process and exploring potential neuro-biomarker of brain impairment in the future.Acknowledgements
This study has received funding by the National Natural Science Foundation of China (Grant No. 82271961, 81621003), the National Key R&D Program of China (2022YFC2009900) and the Sichuan Provincial Foundation of Science and Technology (Grant No. 2019YFS0428).References
[1] Tinuper P, Bisulli F, Cross JH, et al. Definition and diagnostic criteria of sleep-related hypermotor epilepsy. Neurology. 2016;86(19):1834-42.[2] Menghi V, Bisulli F, Tinuper P, et al. Sleep-related hypermotor epilepsy: prevalence, impact and management strategies. Nat Sci Sleep. 2018;10:317-326.
[3] Sharma AA, Goodman AM, Allendorfer JB, et al. Regional brain atrophy and aberrant cortical folding relate to anxiety and depression in patients with traumatic brain injury and psychogenic nonepileptic seizures. Epilepsia. 2022;63(1):222-236.
[4] Dahnke R, Yotter RA, Gaser C. Cortical thickness and central surface estimation. Neuroimage. 2013;65:336-48.
[5] Wan X, Wang W, Wu X, et al. Progressive structural damage in sleep-related hypermotor epilepsy. J Neurosci Res. 2023;101(9):1447-1456.
[6] Bernhardt BC, Worsley KJ, Kim H, et al. Longitudinal and cross-sectional analysis of atrophy in pharmacoresistant temporal lobe epilepsy. Neurology. 2009 May 19;72(20):1747-54.
[7] Kemmotsu N, Girard HM, Bernhardt BC, et al. MRI analysis in temporal lobe epilepsy: cortical thinning and white matter disruptions are related to side of seizure onset. Epilepsia. 2011;52(12):2257-66.
[8] Li W, Jiang Y, Qin Y, et al. Cortical remodeling before and after successful temporal lobe epilepsy surgery. Acta Neurol Scand. 2022;146(2):144-151.
[9] Deng DM, Chen LZ, Li YW, et al. Cortical morphologic changes in recent-onset, drug-naïve idiopathic generalized epilepsy. Magn Reson Imaging. 2019;61:137-142.
[10] Weiner KS, Zilles K. The anatomical and functional specialization of the fusiform gyrus. Neuropsychologia. 2016;83:48-62.
[11] Glickstein M. How are visual areas of the brain connected to motor areas for the sensory guidance of movement? Trends Neurosci. 2000;23(12):613-7.
[12] Liu W, Yue Q, Wu X, et al. Abnormal blood oxygen level-dependent fluctuations and remote connectivity in sleep-related hypermotor epilepsy. Acta Neurol Scand. 2021;143(5):514-520.
[13] Evangelisti S, Testa C, Ferri L, et al. Brain functional connectivity in sleep-related hypermotor epilepsy. Neuroimage Clin. 2017;17:873-881.
[14] Lin JJ, Salamon N, Lee AD, et al. Reduced neocortical thickness and complexity mapped in mesial temporal lobe epilepsy with hippocampal sclerosis. Cereb Cortex. 2007;17(9):2007-18.
Figures